Management of Fracture spine Ali Kotb Ali Prof

Management of Fracture spine Ali Kotb Ali Prof. Of Neurosurgery Ain Shams University

Objectives of Learning n n n Describe the basic spinal anatomy and physiology Evaluate a patient with suspected spinal injury Identify the common types of spinal injuries and their X-ray features. Appropriately manage the spinal-injured patient during the first hour from injury. Determine the appropriate disposition of the patient with spine trauma.

Introduction n Vertebral column injury, with or without neurological deficits, must always be sought and excluded in a patient with n n Multiple trauma. Any injury above the clavicle

Introduction n Spine injury n n Cervical spine 55% Thoracic spine 15% Thoracolumbar junction 15% Lumboscaral spine 15%

Beware n Excessive manipulation and inadequate immobilization of a patient with a spinal cord injury can cause additional neurological damage and worsen the patient’s outcome

Anatomy & Physiology n The spinal column consists of 7 cervical, 12 thoracic, and 5 lumbar vertebrae as well as the sacrum and the coccyx. For many reasons, the cervical spine is most vulnerable to injury The thoracolumbarjunction is a fulcrum between the inflexible thoracic region and the stronger lumbar levels. This makes it more vulnerable to injury, with 15% of all spinal injuries occurring in this region.

Spinal Cord Anatomy Spinal cord ends at L 1 n Three tracts can be readily assessed clinically. n n The corticospinaltract The spinothalamic. Tract The posterior columns

Spinal Cord Anatomy n n n If there is no sensory or motor function below a certain level, this is referred to as a complete spinal cord injury. If any motor or sensory function remains, this is an incomplete injuryand the prognosis for recovery is significantly better. Sparing of sensation in the perianalregion (sacral sparing) may be the only sign of residual function.

Standard Neurological Classification of Spinal Cord Injury

Sensory Examination n A dermatomeis the area of skin innervated by the sensory axons within a particular segmental nerve root. The key sensory points are n n n C-5 ----Area over the deltoid C-6 ----Thumb C-7 ----Middle finger C-8 ----Little finger T-4 ----Nipple T-8 ----Xiphisternum

Sensory Examination n A dermatomeis the area of skin innervated by the sensory axons within a particular segmental nerve root. The key sensory points are n T-10 ---Umbilicus T-12 ---Symphysis L-4 -----Medial aspect of the leg L-5 -----Space between the first and second toes S-1 -----Lateral border of the foot S-3 -----Ischialtuberosityarea n S-4 --5 ----Perianalregion n n
 are. n n n n n C-5")
Myotomes n The important key muscle (s) are. n n n n n C-5 -----Deltoid C-6 -----Wrist extensors C-7 -----Elbow extensors C-8 -----Finger flexors to the middle finger T-1 -----Smalll finger abductors L-2 -----Hip flexors L-3 ------Knee extensors L-4 -----Ankle dorsiflexors L-5 -----Long toe extensors S-1 -----Ankle plantar flexors

Reflexes

Nerurogenic. Shock vs. Spinal Shock n Neurogenic shock results from impairment of the descending sympathetic pathways in the spinal cord resulting in loss of vasomotor tone and loss of sympathetic innervation to the heart. The result is: n n Hypotension Bradycardia

Management of Nerurogenic. Shock The blood pressure can often be restored by the judicious use of vasopressors, but adequate perfusuonmay be maintained without normalizing the blood pressure. n Atropine may be used to counteract hemodynamically significant bradycardia. n

Spinal Shock This refers to the flaccidity and loss of reflexes seen after spinal cord injury. The “Shock” to the injured cord may make it appear completely functionless, although all areas are not necessarily destroyed n The duration of this state is variable n

Classifications of Spinal cord Injuries n Level n n Determination of the level of injury on both sides is important. Injury above the T-1 level-------quadriplegia Injury Below the T-1 level-------paraplegia Apart from the initial management to stabilize the bony injury, all subsequent descriptions of the level of injury are based on the neurologic level

Severity of the Neurologic Deficit Incomplete paraplegia n Complete paraplegia n Incomplete quadriplegia n Complete quadriplegia n Signs of incomplete injury may include: n n n Any sensation ( including position sense) or voluntary movement in the lower extremities. Sacral sparing

Morphology n Spinal injuries can be described as, n n n Fractures Fracture dislocations SCIWORA Penetrating injuries All injuries are either stable or unstable All patients with x-ray evidence of injury and all those with neurologic deficits should be considered to have an unstable spinal injury.

Specific Types of Spinal Injuries n Cervical spine injuries can result from n n n Axial loading Flexion Extension Rotation Lateral bending Distraction
 n C-1 Rotary")
Specific Types of Spinal Injuries Atlanto-occipital Dislocation n Atlas Fracture (C-1) n C-1 Rotary Subluxation n Axis (C-2) Fractures n n Odontoidfracturres Posterior element fractures of C-2 Fractures and Dislocation (C-3 through C-7)
 n")
Specific Types of Spinal Injuries Thoracic Spine Fractured ( T-1 Through T 10) n Thoracolumbar. Junction Fractures ( T-11 through L-1) n Lumbar Fractures n Penetrating Injuries n

Types of incomplete SCI Central spinal Syndrome n Anterior spinal Cord Syndrome n Brown – Sequard syndrome n Posterior spinal Cord Syndrome n

Types of incomplete SCI
 and")
Conus Medullaris Syndrome The effect of injury to the sacral cord (conus medullaris) and lumbar nerve roots is usually loss of bladder, bowel and lower limb reflexes. Lesions high in the conus may occasionally represent upper motor neurone defects and function may then be preserved in the sacral reflexes

Cauda Equina Syndrome Injury to the lumbosacral nerve roots results in areflexia of the bladder, bowel, and lower limbs.

Neurologic Examination n n n n Document all findings Level of consciousness Motor strength Sensation to light touch and pinprick Position sense Diaphragm, abdominal, and sphincter function DTRs, plantar reflexes, sacral reflexes Sacral sparing (perineal sensation, sphincter tone)

General Management n n n ü ü n n n Airway Breathing Circulatory Neurologic Classification Spinal Imaging Gastro. Intestinal System Genitourinary System Skin

General Management n Immobilization n n n Remember to immobilize until cervical spine injury is excluded Intravenous fluids Patients with hypovolemiamay not become tachycardiac(may be bradycardiac) Medications In North America methyprednisoloneis given Transfer

Guidelines for screening patients with suspected Injury Patients who are comatose, have an altered level of consciousness, or are too young to describe their symptoms should at least have a lateral and AP c-spine x-ray n When in doubt, leave the collar on n Backboards Never force the neck

Guidelines for screening patients with suspected Injury n Assess the c-spine film for n n n Bony deformity Fracture of the vertebral body or processes Loss of alignment of the posterior aspect of the vertebral bodies (anterior extent of the vertebral canal Increased distances between the spinousprocesses at one level Narrowing of the vertebral canal Increased prevertebral soft-tissue space

Polytrauma

Guidelines For Screening Patients With Suspected Injury

Guidelines For Screening Patients With Suspected Injury

Guidelines for screening patients with suspected Injury

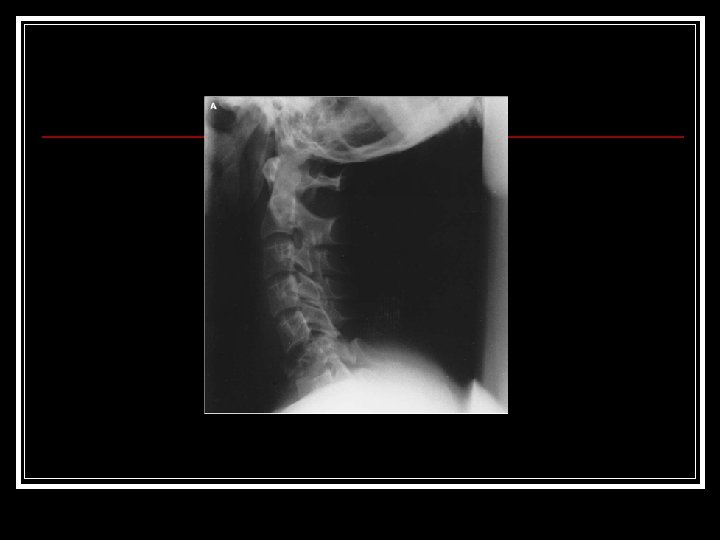
X-Ray Evaluation n Cervical Spine n n n A lateral cervical spine film should be obtained, when indicated, soon after life threatening problems are identified and controlled. Swimmer’s view Open-mouth odontoidview / Oblique view of the odontoidprocess

X-Ray evaluation

Lines Of Alignment On Lateral Radiograph

Hangman’s” Fracture

X-Ray evaluation

X-Ray evaluation

X-Ray evaluation

X-Ray evaluation

X-Ray evaluation

Indications For Thoracic And Lumbar Radiographs Major trauma n Impaired consciousness n Distracting injury n Physical signs of thoracic or lumbar trauma n Pelvic fractures n Altered peripheral neurology n
 spinal columns.")
The three (anterior, middle and posterior) spinal columns.

X-Ray evaluation

Anticoagulation Apply antiembolism stockings n If there are no medical or surgical contraindications give low molecular weight heparin within 72 hours n

Initial Bladder Bowel Management Avoid overdistension n 12– 14 Ch silicone Foley catheter n Beware of paralytic ileus: patients should receive intravenous fluids n for at least the first 48 hours after injury n

Risk Of Acute Peptic Ulceration With Haemorrhage Treat with proton pump inhibitor or H 2 receptor antagonist n Continue treatment for three weeks n

Drug Treatment In Spinal Cord Injury n If methylprednisolone is given, administer at the earliest opportunity: n n 30 mg/kg intravenously and then infusion of 5. 4 mg/kg/h for 23 hours if commenced within 3 hours of injury. If treatment is started 3– 8 hours after injury, the infusion is continued for 47 hours.

Joint And Limb Care Daily passive movement of joints n Splints for hands of tetraplegic patients n Early internal fixation of limb fractures often required n

Trauma Re-evaluation Following spinal cord trauma, occult injuries can easily compromise recovery or aggravate disability. n Complete clinical re-assessments must be performed regularly during the first month after injury n

Skull Traction Used To reduce dislocation n To relieve pressure on spinal cord in case of burst fractures n To splint the spine n

Skull Traction Used

Skull Traction Used

Objects Of Early Transfer To A Spinal Injuries Unit To prevent further spinal cord damage by reduction and stabilisation of spine n To prevent secondary neuronal injury n To prevent medical complications n To expedite all aspects of rehabilitation n

Objectives Of Medical Management Prevent further damage through reduction and immobilisation n Prevent secondary neuronal injury n Prevent medical complications n

Biochemical Disturbances n Hyponatraemia n n n Acute —due to excessive intravenous fluids Chronic —systemic sepsis excessive oral fluid intake drug induced e. g. carbamazepine Treatment n n n treat sepsis —control fluid intake —review drugs
 Hypercalcaemia n Symptoms—constipation n Treatment—hydration")
Biochemical Disturbances n n furosemide, potassium supplements demeclocycline (occasionally) Hypercalcaemia n Symptoms—constipation n Treatment—hydration n achieve diuresis oral disodium etidronate or intravenous disodium

Factors that Aggravate Spasticity Urinary tract infection or calculus n Infected ingrowing toenail n Pressure sores n Anal fissure n Fracture n Contractures n

Management of Spasticity n n n Treat factors that aggravate spasticity Improve comfort/posture Manage pain Passively stretch spastic muscles Regular standing Oral therapy n baclofen n n tizanidine dantrolene n diazepam

Management of Spasticity n n n n Botulinum toxin Motor point injections Implanted drug delivery system for administration of intrathecal baclofen If the above fail, are contraindicated, or are unavailable: tendon release and/or neurectomy, and other orthopaedic procedures intrathecal block (rarely used) 6% aqueous phenol absolute alcohol

Treatment of Contractures Gradual stretching splints n Tenotomy n Tendon lengthening n Muscle and soft tissue division n

Prevention Of Pressure Sores Regular relief of pressure n Regular checking of skin, using mirror n Avoid all pressure if red mark develops n Suitable cushion and mattress, checked regularly n Avoid tight clothes and hard seams n

Prevention Of Pressure Sores

Treatment of Pressure Sores Conservative complete relief of pressure n if slough, treat with desloughing agent or excise n treat general condition, e. g. correct anaemia n Surgical direct closure if possible, with removal of underlying bony prominence n

Nursing Aims Identify problems and prevent deterioration n Prevent secondary complications n Maximise functional recovery n Support patients and relatives n Educate patients to take control of their lives. n

Nursing Aims

Sensory Deprivation Familiarisation of environment n Interpretation of incoming stimuli n Higher levels of cognitive functioning n Reality orientation n Decision-making role n

Sensory Deprivation

Sensory Deprivation

Nutrition Nil by mouth initially n Nutritional risk assessment n Parenteral/enteral feeding n Education: n n n diet feeding aids

Physiotherapy

Physiotherapy

Physiotherapy

Occupational Therapy

Later Management and Complications n Predisposing factors n n n n Nature of original bony injury Age at injury Level of lesion Completeness of lesion Inadequate treatment of bony injury Laminectomy without stabilisation and fusion Gross leg deformities

Later Management and Complications

Spinal Cord Injury In The Developing World n The challenges n n n Poor financial resources Other health priorities make it difficult to allocate significant means for spinal cord injury care Inadequately trained and poorly paid staff Inadequate social help Poor housing conditions Architectural and social barriers

Spinal Cord Injury In The Developing World

Summary n n Attend to life-threatening injuries, minimizing any movement of the spinal column Establish and maintain proper immobilizationof the patient until vertebral fractures or spinal cord injuries have been excluded Obtain a lateral c-spine x-ray, when indicated, as soon as life-threatening injuries are controlled Document the patient’s history and physical examination so as to establish a baseline for any changes in the patient’s neurologic status.

Summary Obtain early consultation with a neurosurgeon and /or an orthopedic surgeon whenever a spinal injury is suspected or detected. n Transfer patients with vertebral fractures or spinal cord injury to a definitive-care facility n
- Slides: 84