Pulmonary Hypertension An Overview of Updated Classification Diagnostic




:")



















- Slides: 25
Pulmonary Hypertension: An Overview of Updated Classification, Diagnostic Algorithm and Treatment Options Shilpa Johri, MD, MBBS, FCCP Pulmonary Associates of Richmond
Objectives: • • • Definition and updated classification of PH Clinical presentation in patients with PH Work up algorithm in suspected PH Identify predictors of increased morbidity and mortality Review management guidelines Clinical case examples Conflict of Interest • • • Consultant and Advisory Board: Gilead Sciences Speaker’s Bureau: Gilead Sciences and Bayer Pharmaceuticals Research funding: Bellephoron Therapeutics and United Therapeutics
Definition of Pulmonary Hypertension • General definition –Mean PAP ≥ 25 mm Hg at rest, measured by right heart catheterization • Hemodynamic characterization of PAH –Mean PAP ≥ 25 mm Hg, PAWP ≤ 15 mm Hg, elevated PVR (> 3 Wood Units) Hoeper, et al. J Am Coll Cardiol. 2013; 62(25): S 42 -50.
Hemodynamic measurements • Cardiac output: 5 L/min • Systemic BP: 120/80 mm. Hg • PAP: 25/10 mm. Hg • PAWP: 10 -12 mm. Hg • Mean PAP : 15 -20 mm. Hg – (SPAP + 2 x DPAP)/3 • PVR : 0. 5 – 2 WU – Mean PAP- PAWP/ CO
Clinical Classification of Pulmonary Hypertension Simonneau, et al. J Am Coll Cardiol. 2013; 62(25): S 34 -41.
Clinical Classification of Pulmonary Hypertension- 5 th World Symposium at Nice 1. Group I PAH Idiopathic Heritable • BMPR 2 • ALK-1, ENG, SMAD 9, CAV 1, KCNK 3 • Unknown Drug- and toxin-induced Associated with: • • • Connective tissue disease (7 -12% of patients with scleroderma) HIV infection (0. 5% of patients with HIV) Portal hypertension (2 -6% of patients with portal hypertension) Congenital heart disease (10% of the adults with CHD) Schistosomiasis (5% of affected patients) 1’ Pulmonary venoocclusive disease 1” Primary pulmonary hypertension of new born Simonneau, et al. J Am Coll Cardiol. 2013; 62(25): S 34 -41.
Clinical Classification of Pulmonary Hypertension- 5 th World Symposium at Nice 2. PH owing to left heart disease 2. 1. Left ventricular systolic dysfunction 2. 2. Left ventricular diastolic dysfunction 2. 3. Valvular disease 2. 4. Congenital/acquired left heart inflow/outflow tract obstruction and congenital cardiomyopathies 4. CTEPH 5. PH with unclear multifactorial mechanisms 5. 1. Hematologic disorders: chronic hemolytic anemia, myeloproliferative disorders, splenectomy 3. PH owing to lung diseases and/or hypoxia 5. 2. Systemic disorders: sarcoidosis, pulmonary Langerhans cellhistiocytosis: 3. 1. Chronic obstructive pulmonary disease lymphangioleiomyomatosis, neurofibromatosis, 3. 2. Interstitial lung disease 3. 3. Other pulmonary diseases with mixed restrictive vasculitis 5. 3. Metabolic disorders: glycogen storage disease, and obstructive pattern Gaucher disease, thyroid disorders 3. 4. Sleep-disordered breathing 5. 4. Others: tumoral obstruction, fibrosing 3. 5. Alveolar hypoventilation disorders mediastinitis, chronic renal failure, segmental PH 3. 6. Chronic exposure to high altitude 3. 7. Developmental lung diseases Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013; 62(25 Suppl): D 34 -D 41
55 year old Caucasian female with history of HTN was referred for exertional dyspnea for 4 years Actively working with frequent travel- started finding it difficult to walk through airports with hand baggage Previous work up had included a negative stress test (3 years ago), negative left heart cath (2 years ago) and relatively unremarkable echo with PASP estimated at 35 one year ago, CTA negative for pulmonary emboli 2 years and 6 months ago. Was on treatment with beta blockers and benzodiazepines were added for dyspnea attributed to anxiety She worsened to a point where she had to stop several times before she could reach her seat in the 13 th row during basketball games at UNC Accentuated P 2 on exam, both previous CTA s showed dilated central PA
CT scan 2 years apart RHC: PAP 91/39, mean 60, PAWP 5, Sv. O 2 79%, TDCO 6. 97, PVR 7. 89 Wood Units Sequential therapy, currently on 3 agents
PAH distribution Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013; 62(25 Suppl): D 34 -D 41
Epidemiology of PAH • • • Prevalence in the U. S. - 15 -50 cases/million • Modern day: Patient survival has dramatically improved as treatment options for PAH have increased Only 1/3 to 1/2 of those are diagnosed and treated Historically: Due to rapid progression of morbidity and mortality, once patients were diagnosed with pulmonary hypertension they were described as entering “the kingdom of the near-dead” Mc. Goon, et al. J Am Coll Cardiol. 2013; 62(25): S 51 -9.
Mechanisms of Pathology for PAH Endothelin pathway Prostacyclin pathway Nitric oxide pathway Endothelial cells Preproendothelin L-arginine Proendothelin Arachidonic acid Prostaglandin I 2 NOS Nitric oxide Endothelinreceptor A Endothelin-1 Endothelinreceptor antagonists Endothelinreceptor B s. GC stimulator Prostaglandin I 2 GTP Exogenous nitric oxide c. GMP Phosphodiesterase type 5 Vasodilatation and antiproliferation Vasoconstriction and proliferation Phosphodiesterase type 5 inhibitor Adapted from: Humbert, et al. N Engl J Med. 2004; 351: 1425 -1436. c. AMP Prostacyclin analogues Vasodilatation and antiproliferation
Mechanisms in PAH Excessive pulmonary vascular remodeling Sustained vasoconstriction In situ thrombosis Increased pulmonary vascular resistance Tuder, et al. J Am Coll Cardiol. 2013; 62(25): S 4 -12.
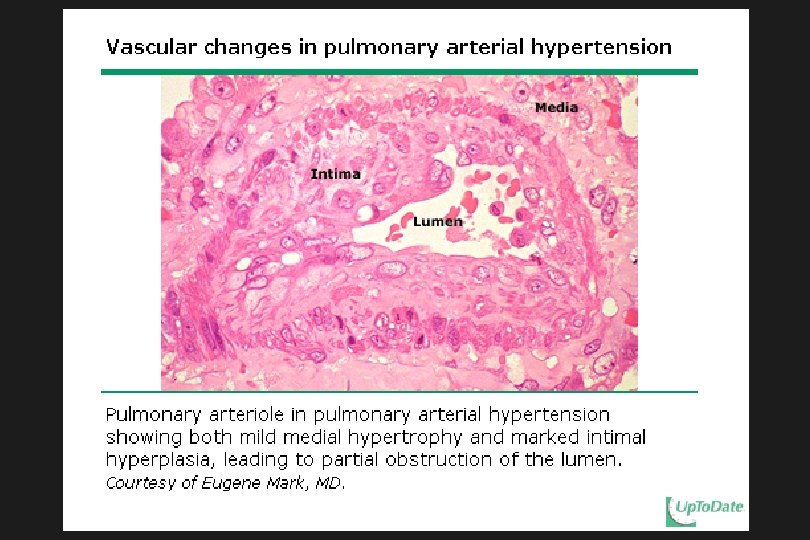
Pathology of PAH
Symptoms • Clinical symptoms • Other non-specific symptoms in patients with PAH –Unexplained dyspnea on exertion –Presyncope –Signs of right ventricular dysfunction –Fatigue, weakness, angina, abdominal distension, edema Suspect PH? Galie, et al. Eur Heart J. 2009; 30: 2493 -2537. Hoeper, et al. J Am Coll Cardiol. 2013; 62(25): S 42 -50.
Diagnostic Algorithm for PAH RHC is MANDATORY to confirm the diagnosis of PAH Hoeper, et al. J Am Coll Cardiol. 2013; 62(25): S 42 -50.
Diagnostic Approach to PAH Mc. Laughlin, V. V. et al. J Am Coll Cardiol 2009; 53: 1573 -1619
Chest X-Ray and ECG in PAH Mc. Laughlin, V. V. et al. J Am Coll Cardiol 2009; 53: 1573 -1619
Echocardiography for PAH • • Evaluate left heart Evaluate valves Evaluate for structural lesions Evaluate right heart size Estimate right sided pressures Measure indices of RV function • TAPSE • Tei index Evaluate for pericardial effusion
6 Minute Walk Test • • • Easy to perform Functional assessment during office visits Assess response to therapy Primary end point of clinical trials Performed according to stated ATS guidelines to ensure reproducibility
6 Minute Walk Test • • • Correlation between RV function and cardiac output Correlation with prognosis 3 year survival in patients with 6 MWD of < 332 m: 20% 3 year survival in patients with 6 MWD of > 332 m: 92% Current goal directed therapy: aim for 380 m Miyamoto, S, Nagaya, N, Satoh, T. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension: Comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2000; 161(2 Pt 1): 487– 492.
RHC is more than just measuring pressures! Cardiac output: 5 L/min Cardiac index: 2. 5 -3. 5 L/min/m 2 PVR (mean PAP-PAWP/ CO): 0. 6 to 2. 5 WU Pulmonary artery saturation (PA sat): 70% Acute vasoreactivity test for PAH: Positive if decrease of >/= 10 in m. PAP to < 40 without drop in cardiac output Agents: i. NO, adenosine, epoprostenol Consider exercise, volume loading, LHC as indicated
9/2011: 52 YO man at NYHA FC III (long distance runner, 10 K 62 mins), was unable to run a soccer field lap with his son >> DOE with 1 flight of stairs >> DOE level ground. Stress echo: Resting RVSP 85 -90 which rose to 110 -120 mm. Hg post exercise. RHC – 10/2011 NYHA FC III PAP: 83/21 Diltiazem m. PAP: 42 360 mg m. PAWP: 11 TDCO: 6. 27 PVR: 344 Post i. NO Data PAP: 47/10 m. PAP: 22 TDCO: 6. 46 PVR: 86 RHC 5/2013 NYHA FC I 10 K time of 56 mins!! Echo: enlarged RV PAP: 64/22 (36) TDCO: 6. 83 m. PAWP: 15 PVR: 245 Post i. NO Data PAP 43/14 (23) PVR: 126 TDCO: 6. 3 SBP: 102/65, HR 62 Tadalafil 40 mg added 10 K off limits! 8/2013 - 3/2018 RVSP ~ 50 - 60 Normal RV NYHA FC I 10 K still off limits Vasoreactive PAH Excellent prognosis !
Survival In PAH- Depends On The Right Ventricle Patient 1 PASP 90 Normal RV size and function Patient 2 PASP 50 Dilated RV with reduced function