Pediatric Resuscitation Adel Ahadi MD Assessment n 30














/4 ETT depth")





 – LIDOCAINE –")



 • Actions:")




 • Uses:")






- Slides: 42
Pediatric Resuscitation Adel Ahadi , MD
Assessment n 30 second rapid cardiopulmonary assessment is structured around ABCDE’s. • • • Airway Breathing Circulation Disability Exposure
Heimlich for Infants 5 back blow 5 Chest thrusts
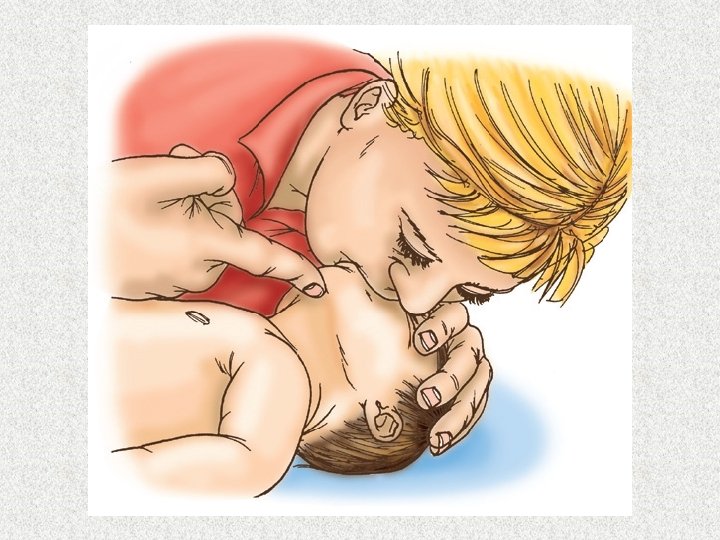
Clearing the Mouth
Heimlich for children> 1 year
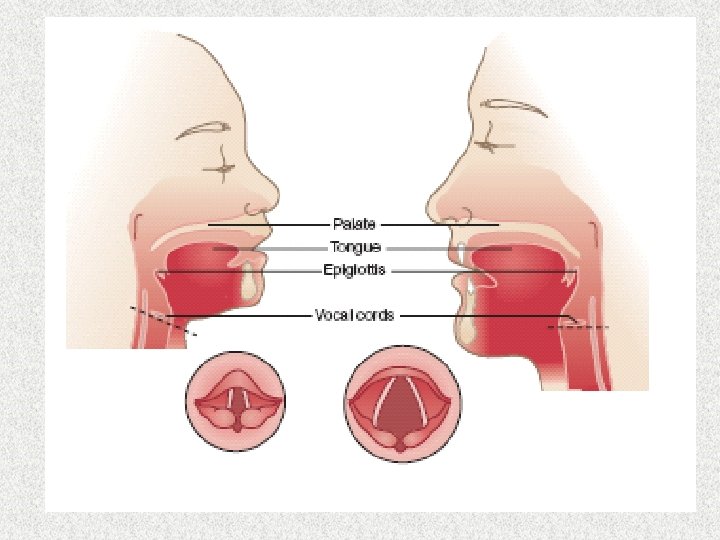
Airway n Airway must be clear and patent for successful ventilation. • • Position Suction Administration of oxygen Bag-mask ventilation
Airway Management Head Tilt-Chin Lift Avoid extreme hyperextension Jaw Thrust
Breathing n n Breathing is assessed to determine the child’s ability to oxygenate. Assessment: • Respiratory rate • Respiratory effort • Breath sounds • Skin color
Breathing Look-Listen-Feel
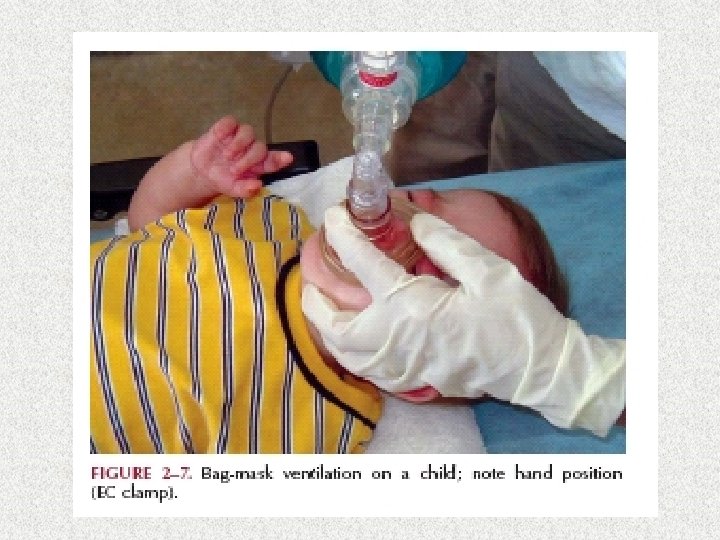
Bag-Mask Ventilation • Clear, plastic mask with inflatable rim • Place fingers on mandible to avoid provides atraumatic seal compressing pharyngeal space • Hand on ventilating bag at all times to • Proper area for mask applicationmonitor effectiveness of spontaneous bridge of nose extend to chin breaths • Maintain airway pressures <20 cm • Continous postitive pressure when H 2 O needed to maintain airway patency
Circulation In infants 1 finger breadth below intermammary line v 2 fingers or thumbs encircling v At least 100/minute v 1/3 to 1/2 of chest v Brachial or femoral pulse is used to check for pulse
Circulation In older children the lower third of the sternum v Maintain continuous head tilt with hand on forehead v One hand v 100/minute v 1/3 to 1/2 of chest v Carotid pulse is used to check for pulse
Intubation Ø Ø Ø Indications Failure to oxygenate Failure to ventilate Failure to protect the airway Anticipation of worsening clinical course
Tracheal Tube- size and depth? Children > 1 year: ETT size: (Age+16)/4 ETT depth (lip): ETT size x 3
Laryngoscope Blades Straight Better in younger children with a floppy epiglottis
Laryngoscope Blades Curved Better in older children who have a stiff epiglottis
Confirmation of ETT Placement Ø Ø Seeing tube go through cords Clinical Confirmation v Water vapor seen inside tube v O 2 Saturation v Chest rise v Equal breath sounds v No sounds over epigastrium CO 2 Detection / Esophageal Detector Devices Chest X-ray NO single technique is 100% reliable
Acute Deterioration after Intubation D. O. P. E: Displacement Obstruction Pneumothorax Equipment failure
Inadequate Improvement after Intubation? Ø Ø Ø Inadequate Tidal Volume Excessive Leak Around The Tube Leak or Disconnection in Ventilator System Inadequate PEEP Inadequate O 2 Flow from Gas Source Air Trapping and Impaired Cardiac Output
Routes for Drugs in CPR n n Intravascular Intraosseous Endotracheal (LANE) – LIDOCAINE – ATROPINE – NALOXONE – EPINEPHRINE Note: flush each medication with 3 -5 ml of NS
IV Solutions n Crystalloid solution • Normal saline 20 ml/kg bolus over 20 minutes • Lactated ringers
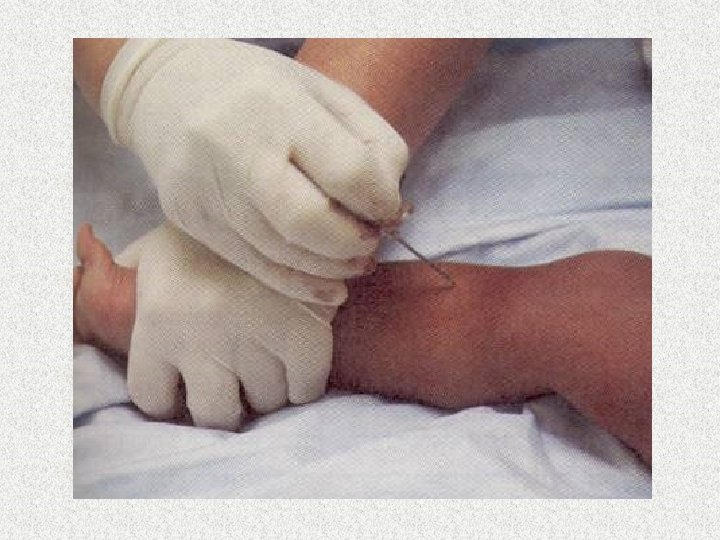
Vascular Access – New Guidelines n New guidelines: in children who are six years or younger after 90 seconds or 3 attempts at peripheral intravenous access – Intraosseous vascular access in the proximal tibia or distal femur should be initiated.
Glucose n n n 10% to 25% strength Action: increases glucose in hypoglycemia Dosing: 0. 5 – 1 g/kg
Pediatric Resuscitation Fluids & Medications n Epinephrine (a & b adrenergic stimulator) • Actions: vasoconstriction, increases contractility, heart rate, relaxes smooth muscle • Uses: cardiac arrest, symptomatic bradycardia, hypotension • Dose: 0. 01 mg/kg (0. 1 ml/kg of 1: 10, 000 solution) – May repeat every 3 -5 min – Continuous 0. 1 -1 mg/kg/min
Amiodarone n n n Used in atrial and ventricular antiarrhythmic Action: slows AV nodal and ventricular conduction, increase the QT interval and may cause vasodilation. Dosing: IV/IO: 5 mg / kg bolus
Adenosine n n n Drug of choice of symptomatic SVT Action: blocks AV node conduction for a few seconds to interrupt AV node re-entry Dosing • First dose: 0. 1 mg/kg max 6 mg • Second dose: 0. 2 mg/kg max 12 mg
Pediatric Resuscitation Fluids & Medications n Sodium Bicarbonate • Uses: severe metabolic acidosis with effective ventilation, hyperkalemia, hypermagnesemia, tricyclic poisoning • Dose: 1 m. Eq/kg (1 ml/kg of 8. 4%) IV – may repeat every 10 min • Side effects: metabolic alkalosis, impaired O 2 release, pseudohypokalemia, hypocalcemia, decreased VF threshold, Na+/water overload
Pediatric Resuscitation Fluids & Medications n Calcium Chloride • Uses: hypocalcemia, hyperkalemia, hypermagnesemia, Ca+ channel blocker overdose • Dose: 20 mg/kg of Ca. Cl 10% – Administer over 10 -20 seconds – Flush before and after administration • May cause bradycardia
Pediatric Resuscitation Fluids & Medications n Dopamine (dopamine & b adrenergic stimulator) • Uses: inadequate cardiac output, hypotension, enhanced splanchnic blood flow & urine output • Dose: 2 to 20 mg/kg/min • May cause tachycardia, arrhythmias, and hypertension
Pediatric Resuscitation Fluids & Medications n Naloxone • Narcotic antagonist • Reverses effects of respiratory depression, sedation, hypotension, hypoperfusion • Dose: 0. 1 mg/kg; 2 mg for children over 5 yo or 20 kg • May abruptly reverse narcotic depression – Nausea, tachycardia, hypertension, tremulousness, seizures, arrhythmias, asystole, pulmonary edema
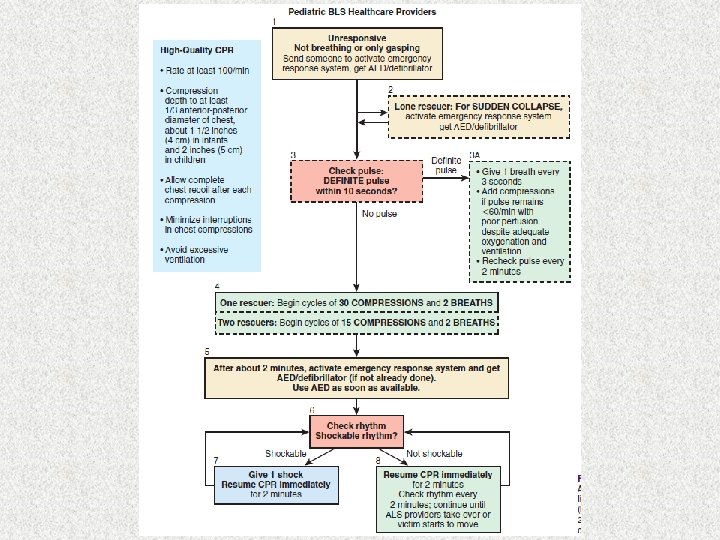
Pediatric Arrest n n Most often respiratory Lone-rescuer • 5 cycles CPR, then activate EMS n Two-rescuer CPR • 15 : 2
PALS Tachycardia Algorithm
Pediatric ALS n n n No vasopressin or atropine Pediatric AED attenuator if available IO access if no IV
PALS Bradycardia Algorithm
THE END