Resuscitation and Post Resuscitation Care Jose G Cabanas

Resuscitation and Post Resuscitation Care Jose G. Cabanas, MD MPH FACEP Paul R. Hinchey, MD MBA FACEP Office of the Medical Director Austin-Travis County EMS System

Austin/Travis County EMS n n n Approximately 1. 2 million citizens, 1, 100 square miles, 120 k EMS calls per year 1, 000 cardiac arrests responses per year 14 Fire Departments (1, 500 FF’s, ) EMS Transport Agency (400 Paramedics) EMS Systems are judged by their cardiac arrest resuscitation rates – – Most large cities are 5 -7% King Cnty Wa 35 -45% Wake Cnty NC 38 -42% Austin 38%

Why are we talking about Cardiac Arrest Resuscitation?
 Acute")
Philosophy of Five n Time Dependent – – – n Acute MI (STEMI) Acute Stroke Trauma / Surgical Emergency Intervention Dependent – Cardiac Arrest – Respiratory Distress n Sophisticated providers/systems understand the difference

Time Dependent n n These conditions can not be definitively treated in the pre-hospital environment Requires specialized intervention only available in the hospital Outcomes are improved by early access to definitive intervention Goal is recognition and short scene interval

Intervention Dependent Initial treatment can be delivered in prehospital environment n Outcomes linked to prehospital interventions n Goal is identification and initiation of treatment n Scene intervals are NOT critical n

Updates in Out-of. Hospital Resuscitation and Post Resuscitation Care

Objectives n n n Describe the importance of continuous compressions and controlled ventilations Discuss what to do with the airway/drugs Acknowledge the difficulty of performing continuous compressions and the need for a scripted process Discuss importance of on-scene post ROSC stabilization Describe role of resuscitation centers Identify questions for the future

Why do we worry about CA n Represents < 1% of our calls but… n > 70% of CA arrests occur outside the hospital n Definitive management of cardiac arrest is in the prehospital environment

“Stated succinctly, if ACLS care in the field cannot resuscitate the victim, ED care will not resuscitate the victim. ” 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Part 7. 2: Management of Cardiac Arrest)

Priorities in OOHCA Changed n n n Emphasis on compression Limit interruptions from ANYTHING Goal is to maximize % of time in compressions Single D-fib every two minutes – – Precharge monitor before break Follow d-fib immediately by compressions Decreased importance of ventilations – Fewer number of breaths – Each delivered more slowly

So if you had to push a car, would you push a few feet and stop…. . only to start again a few minutes later?

So how important are compressions?

Compression fraction article Circulation 2009

If compressions are the most important therapy when do you move the patient…. .
: 106")
Prehospital Emergency Care 2011; 15(1): 106
 N = 108 % (25 th, 75 th) Scene Correct Rate% Median:")
Results (Pre-Feedback) N = 108 % (25 th, 75 th) Scene Correct Rate% Median: 44. 8 (9. 54, 59. 6) Mean: 38. 49 CI (33. 2, 43. 78) Transport Correct Rate% Median: 11. 16 (5. 83, 39. 32) Mean: 23. 16 CI (18. 35, 27. 97) Scene Correct Depth% Median: 40. 94 (15. 96, 73. 29) Mean: 45. 06 CI (38. 76, 51. 37) Transport Correct Depth% Median: 8. 88 (2. 62, 49. 01) Mean: 26. 37 CI (20. 12, 32. 63)
 N = 35 % (25 th, 75 th) Scene Correct Rate% Median:")
Results (Post-Feedback) N = 35 % (25 th, 75 th) Scene Correct Rate% Median: 48. 16 (14. 68, 62. 36) Mean: 43. 6 CI (34. 61, 52. 59) Transport Correct Rate% Median: 19. 0 (9. 52, 60. 22) Mean: 32. 78 CI (23. 21, 42. 33) Scene Correct Depth% Median: 75. 73 (36. 23, 95. 07) Mean: 66. 86 CI (56. 57, 77. 16) Transport Correct Depth% Median: 14. 0 (4. 78, 90. 78) Mean: 42. 04 CI (27. 98, 56. 11)

How about ventilations?

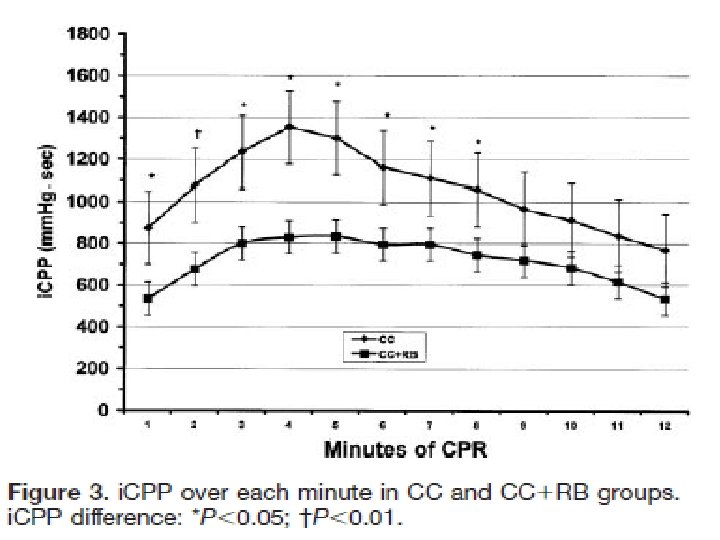
Importance of controlled Ventilation n Normal inspiration is negative pressure – Encourages blood return to the chest n Artificial ventilation is positive pressure – Reduces blood return to the chest n n The faster the ventilation rate the higher the mean intrathoracic pressure Higher MIP reduces cerebral emptying and reduces blood return to the heart

Survival in hyperventilation

STOP Hyperventilating n n n Telling providers not to hyperventilate is ineffective High adrenaline situation Tendency to ventilate faster and faster Requires conscious effort to slow rates Need constant reminder – Timing device – Goal directed ventilation

How to Deliver Ventilations n n Goal is to oxygenate primarily and ventilate as a secondary consideration Must provide continuous uninterrupted compressions Traditional method is endotracheal intubation but increases interruption in compresions So is this a paradigm that needs to be challenged?
")
Interrupt CPR…not ME n n n 100 Cardiac Arrests CPR interruptions 2* (1 -9) 1 st ETI interruption 46. 5 s* (7 -221 s) Total all ETI interruption 109. 5 s* (13 -446 s) 1/3 > 1 min; ¼ > 3 min ETI Interruptions 23% of all * Indicates median values reported Wang et al Ann Emerg Med. 2009

But an advanced airway is a better airway…. .

n n Retrospective analysis of OOHCA 1, 294 Cardiac Arrests – – – n n 79% received intubation 10% BVM 4% Combitube/EOA After adjusting for age, bystander CPR, witnessed arrest and initial rhythm OR for BVM vs Advanced airway was 4. 5

What is best vascular access? n n Goal is vascular access by any means that does not interrupt compressions Preferably rapid reliable access that does not detract from other tasks Based on assumption that the drugs do anything…. more on this later IO access can be achieved in < 10 sec but which site should be used?
 used tibial site first – Initial")
n n 88 Cardiac arrest 56 (65. 9%) used tibial site first – Initial success rate 89. 7% – 3 (5. 8%) dislodged n 18 (34%) used humerus first – Initial success rate 60% – 6(33%) dislodged n Overall success rates – Tibia 84. 5% – Humerus 40%

So what about the drugs? n n Most recent quandary Standard of care is currently being challenged Will be a major change in management in your career Who will make the first step…

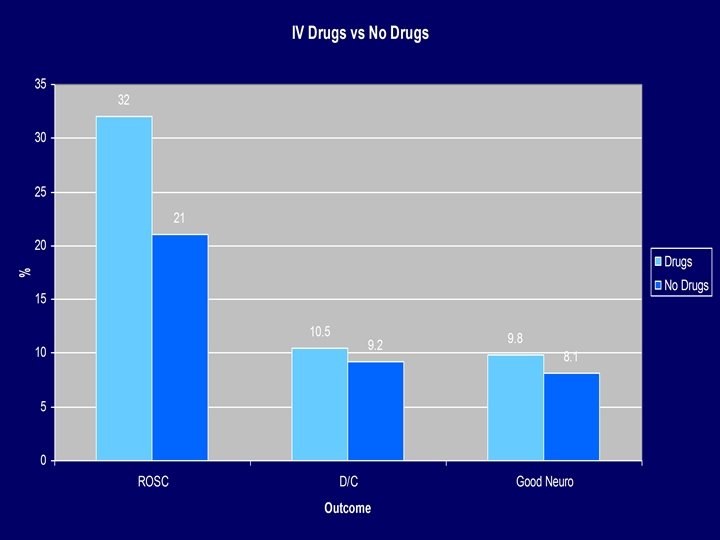
n 851 patients with OOHCA randomized to: – 418 given IV drugs – 433 given no drugs n n Primary outcome hospital discharge Also looked at: – – – Hosp admission with ROSC Neuro outcome at discharge Survival at 1 year

Running the Arrest n n n CA is not the most diagnostically challenging condition so thought to be “EASY” EXECUTION is anything but… Conflicting interests of multiple tasks and the need for continuous uninterrupted compressions and infrequent occurence

Task Interruptions n n n n Airway interventions and IVs Ventilations Pulse checks Rhythm analysis Defibrillation Changing compressors Patient movement

We have limited awareness of task time in complex processes…. so these interruptions should be engineered and choreographed to minimize their impact…. .

>20 second pause for defibrillation. Appears that a ventilation was given before the compressions resumed. Compressions resume 10 seconds after shock delivery.

Long pause for ventilations. Then short sequence of compressions during defib charging. Compressions resumed approximately 5 seconds after shock 1 delivered.

Why engineer the process? n Creates uniformity: – – – n Accurate assessment of outcomes Linking specific interventions to outcomes Baseline for future modification In the process it: – – – Improves outcomes Improves efficiency Reduces errors


Professional CA resuscitation is to CPR …. …. what a pit crew is to changing tires

Pit Crew Model n n Same name…many versions CPR – Maximize compression fraction – Effective compression(rate/depth) – Provider fatigue n n Controlled ventilations Defib – Pre-charge @1: 45 – Emphasis on Shock/Don’t’ shock

Current Goal: Less than 10 second break in every 2 minute cycle of CPR

Staying Alive or Another One Bites the Dust? n n Staying alive 103 bpm 30: 2 – – n 100 compressions/min =18 s for compressions 5 s break for ventilations every 30 compressions? 18 of every 23 s in active compression is 78% NOT counting other breaks in CPR Pit Crew – – – Continuous compressions w/asynchronous ventilation 10 s break every 2 min is 92% 5 s break every 2 min is 96%

So we went to the simulation lab and now it’s ALL choreographed….


Need cpr checklist © 2010 Paul R. Hinchey

Some Scenarios

Scenario 1 78 y/o Wal-Mart greeter suffers cardiac arrest in the front of a store: 1. Where do you work the cardiac arrest? Would this be different if it were in his house? 2. When do you begin transport to the hospital? 3. If unsuccessful when do you terminate the resuscitation?

Scenario 2 78 y/o Wal-Mart greeter has been resuscitated from CA and is being transported when he re-arrests: 1. What would you instruct your crews to do if they were 20 min out from the hospital? 2. What if they were 5 min out?

Scenario 3 78 y/o suffers CA at home. Wife does 2 min dispatcher directed CPR. Pt has ROSC and wakes up. Walks to couch. Crews find in CHF and treat appropriately w/meds and CPAP. FF ride w/crew to hosp. While pulling into ED bay pt goes into CA: 1. What do you want your crews to do?

Take Home Message n n n CA is not as easy as once thought Pre-hospital providers must be the experts Its all about compressions Airway, drugs, etc are a big ? If you want to do this well you must have universally understood goals and plan

Post Resuscitation Care

Post-Cardiac Arrest Syndrome n Post-cardiac arrest brain injury – Responsible for 68% of deaths of patients who survived to ICU admission (Lever, 2004) n Post-cardiac arrest myocardial dysfunction – LV dysfunction, myocardial stunning, cardiogenic shock n Systemic ischemia/reperfusion injury – Inflammatory response, impaired vasoregulation, oxygen delivery and utilization, resulting in hypotension / MSOF n Persistent precipitating pathology – STEMI, Toxic Ingestion, Hypoxia, Hemorrhage, etc.

Phases of Post-Cardiac Arrest Syndrome

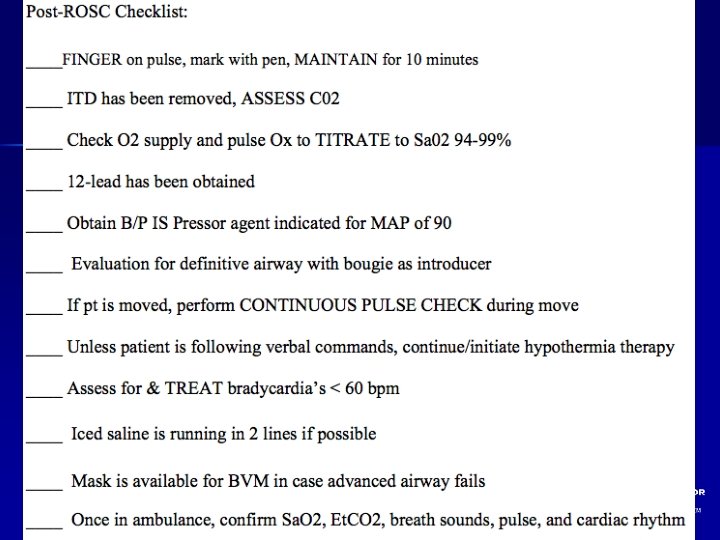
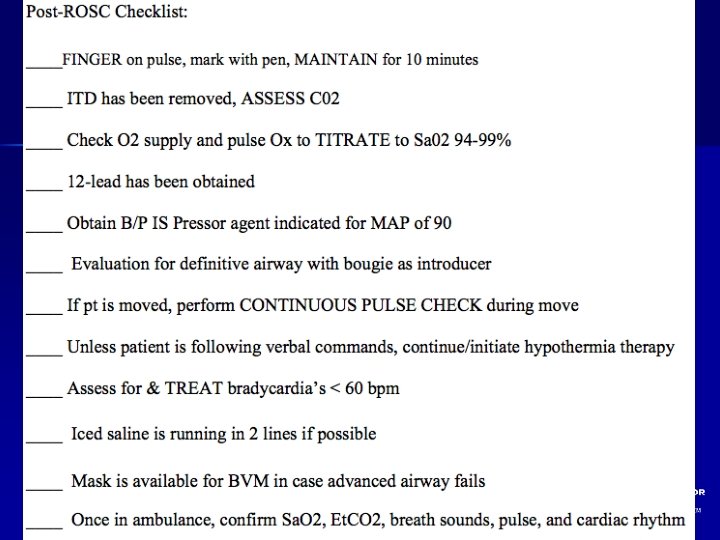
Post-Resuscitation Care n Goals of Post-Arrest Care – – n Maintain Hemodynamic Stability Preserve the Brain Avoid hyperventilation Prevent re-arrest Elements of Post-Care include – – – Vasopressor titration Therapeutic Hypothermia Early Cardiac Catheterization Sedation Glucose and Electrolyte Management

Post Cardiac Arrest Care n n The first 20 minutes after ROSC is the Immediate Phase of Post Cardiac Arrest Syndrome Patients in these phases may be critically ill and benefit by immediate treatment AT SCENE: – This is a better strategy for patient survival than rapid movement to the vehicle and rapid transport delaying or deferring key interventions – Failure to initiate immediate aggressive treatment may result in re arrest of patient or increased morbidity

n 1, 199 Cardiac Arrests n ROSC in 27. 4% n Rearrest in 36% n Time to rearrest – Median 3. 1 min (1. 6 -6. 3)

Post-Resuscitation Care n Focus should be on restoring perfusion – Perfuse the myocardium – Perfuse the brain n n Fluids and pressors for MAP >90 Remove the ITD Initiate hypothermia Obtain 12 lead EKG THEN move the patient

Barriers in Post-Cardiac Arrest Care n n n Post– cardiac arrest patients are treated by multiple teams of providers Variation in post-cardiac arrest treatment and patient outcome between institutions. Limited reliability of early prognostication (<72 hours after arrest)

Journal Iowa Medical Society, November 1964

Therapeutic Hypothermia HACA 2002 Bernard 2002 Idrissi 2001

ILCOR Advisory Statement • Unconscious adult patients with ROSC after out-of-hospital VF cardiac arrest should be cooled to 32°C - 34°C for 12 - 24 hours • Possible benefit for other rhythms or in-hospital cardiac arrest

Editorial Comments n “The reason hypothermia has not become the standard of care for postresuscitation is simple. Emergency and EMS physicians have failed to make it so. ” – Mennegazzi and Callaway, PEC 2005

“The Future” n 720 j Defibrillation? n Hands on Defibrillation? n Intra-arrest cooling? n Mechanical CPR and AC/DC CPR? n Regional Receiving Facilities?

Knowledge Gaps n Impact of Prehospital Cooling in Outcomes? – – – n n n Continuous temperature in the Field? Rate of Cooling? Target? How Long? Urban vs. Rural EMS? ALS Vs BLS? How do we train Providers?

Take Home Message n Resuscitation is not over with ROSC n Post-Cardiac Arrest Patients need to be treated with a high sense of urgency. n Patients should receive hypothermia specially if initial rhythm was VF/VT. n Hypothermia is not a substitute for other key components in the Chain of Survival

Take Home Message n n Post-resuscitation/cardiac specialty hospitals should receive patients directly from the field or in prompt transfer Coordination between EMS, EM, ICU, and Cardiology is a must!! Engage all stakeholders in your system Management of Cardiac Arrest is evolving rapidly!! EMS Medical Directors must keep up


Questions?

Out-of-Hospital Initiation of Therapeutic Hypothermia with Cold Saline Improves Survival in Patients with Return of Spontaneous Circulation in the Field. Jose G. Cabanas MD, MPH / Brent Myers MD, MPH Wake County EMS System

Authors • • • Brent Myers MD, MPH, Wake EMS/Wake. Med Jose G. Cabanas, MD, Wake EMS/Wake. Med Ryan Lewis, MS, EMT-P, Wake EMS Valerie De Maio, MD MSc, Wake. Med Graham Synder, MD, Wake. Med Gay Beneveides, MD, Wake. Med Robert Denton, MD, Rex Healthcare Daniel Licastese, RN, Rex Healthcare Robert Lee, MS MA, Wake. Med
")
Disclosure • This Project was supported by the SAEMS Physio-Control Award (2008)

Objective To determine the impact on survival of a standard postresuscitation care protocol that includes prehospital initiation of therapeutic hypothermia in patients with return of spontaneous circulation (ROSC) in the field.

Methods Observational cohort • “Before and after” – Introduction of Therapeutic Hypothermia for patients with prehospital ROSC • Post-resuscitation patients are selectively transported to one of 2 high volume PCI centers • Wake County NC - pop. 897, 000 • April 2005 through December 2008 •

Cardiac Arrest Response • • All calls receive EMD from a single, high-volume center Fire first response with AED and compressions Paramedic response with transport ambulances (2) Supervisory response at paramedic level
![Protocol Revision • [Apr 2005 -Oct 2006]: Continuous compressions, controlled ventilations • [Oct 2006](http://slidetodoc.com/presentation_image/23ed9ae44a81188122f67a9bf7ebf2df/image-79.jpg "Protocol Revision • [Apr 2005 -Oct 2006]: Continuous compressions, controlled ventilations • [Oct 2006")
Protocol Revision • [Apr 2005 -Oct 2006]: Continuous compressions, controlled ventilations • [Oct 2006 -Dec 2008]: Induced Hypothermia after ROSC

Criteria for Induced Hypothermia • • • ROSC after cardiac arrest not related to trauma or hemorrhage Age 16 years or greater Female without obviously gravid uterus Initial temperature >34 C Patient with advanced airway (no RSI) Patient remains comatose without purposeful response to pain

Data Collection • • All EMS records are maintained in an electronic database Records with any of the following characteristics are reviewed to determine if cardiac arrest occurred: • • EMS Patient Disposition = cardiac arrest CPR procedure is recorded Defibrillation is recorded Induced Hypothermia Procedure
")
Inclusion Criteria • All adult patients resuscitated from out of hospital cardiac arrest (OHCA) prior to hospital arrival, regardless of initial rhythm, were included if they had ROSC in the field.

Exclusion Criteria • • Age less than 16 Obvious traumatic origin of arrest EMS witnessed arrest Arrest not in EMS control • Prison facilities • Out-of-system intercept • Arrests under direction of non-EMS physician
 Neurologically intact survival was defined")
Outcome Measures • • • Discharge from hospital (primary) Neurologically intact survival was defined as CPC 1 or 2 at time of hospital discharge. 2 blinded physician reviewers from each hospital independently assigned CPC scores based on patient discharge records
 227 After (26 Months)")
Included Patients / Phase All Phases N=640 Before (17 Months) 227 After (26 Months) 413
 Male sex Bystander witnessed arrest Bystander CPR")
Patient and EMS Characteristics Mean age (yrs) Male sex Bystander witnessed arrest Bystander CPR Mean Response (mins) Initial rhythm VF/VT Before After (n=227) (n=413) 66 64 62% 60% 45% 32% 38% 39% 5. 6 35% 38% NOTE: no statistically significant difference between study periods

Multivariate Odds of Neuro Intact Survival Factor Odds 95% CI Age 0. 97 0. 96 -0. 98 Bystander CPR 1. 44 . 94 -2. 19 Vfib 8. 58 5. 5 -13. 1 Hypothermia (After) 1. 95 1. 23 -3. 09

Survival to Hospital Discharge for All Rhythms 35 28. 8% 30 25 20 17. 2% Before 15 After 10 5 0 Survival NOTE: statistically significant difference p value <0. 0163

Survival to Hospital Discharge for All Rhythms 60. 0% 50. 0% 40. 0% 30. 0% Before After 20. 0% 10. 0% Overall* VF/VT *Difference in overall survival was significant with a p-value of 0. 0163 PEA Asystole

Percent of Survivors Neurologically Intact 90 80 70 33 Survivors 60 112 Survivors 50 CPC 1&2 40 CPC 3&4 30 20 10 0 Before After NOTE: no statistically significant difference between study periods

Limitations • • • Protocol-driven pre- and postresuscitation cardiac arrest care Hawthorne effect Intention-to-treat analysis

Conclusion • Out-of-hospital standard post-resuscitation care protocol that includes induced hypothermia for all patients with ROSC significantly improved survival to hospital discharge in this EMS system

www. wakeems. com
 • Providers: 1,")
Wake County EMS • Annually 70, 000+ 911 calls (700 OHCA) • Providers: 1, 500 BLS, 225 ALS, 17 APPs • Tiered response incl. dispatch assisted CPR, first responder apparatus and paramedic supervisor to high acuity calls • Serve 7 hospitals of 3 health care systems, incl. 2 PCI capable facilities • Annual protocol updates in April Utstein style data collection template •

Survival to Discharge – VF/VT 60 54. 5% 50 41. 8% 40 30 Before After 20 10 0 Survival NOTE: no statistically significant difference between study periods
 – – – n Decrease metabolic")
Optimizing Neurologic Resuscitation n Mild Induced Hypothermia (IH) – – – n Decrease metabolic demand 4, 5, 6, 7 Inhibits inflammatory cascade 12, 14, 15 8, 11, 14, 15 IH is time sensitive Hemodilution 12, 13 – Normal saline dilution as part of hypertensive reperfusion strategy n Hypertensive reperfusion – Use of vasopressors to target MAP of 90

Circulation 2007

n Standardized post resuscitation bundle: – – – Cardiac catheterization Therapeutic hypothermia Hemodynamic maintenance Ventilator management Electrolyte/glucose control Prognostication
 Treatment period 34/61(56%)")
n n Outcome –CPC 1 or 2 Control period 15/58 (26%) Treatment period 34/61(56%) OR 3. 61 (CI 1. 66 -7. 84, p=0. 001)


The device that allows us to oxygenate the patients brain and myocardium and causes the… LEAST interruption in compressions

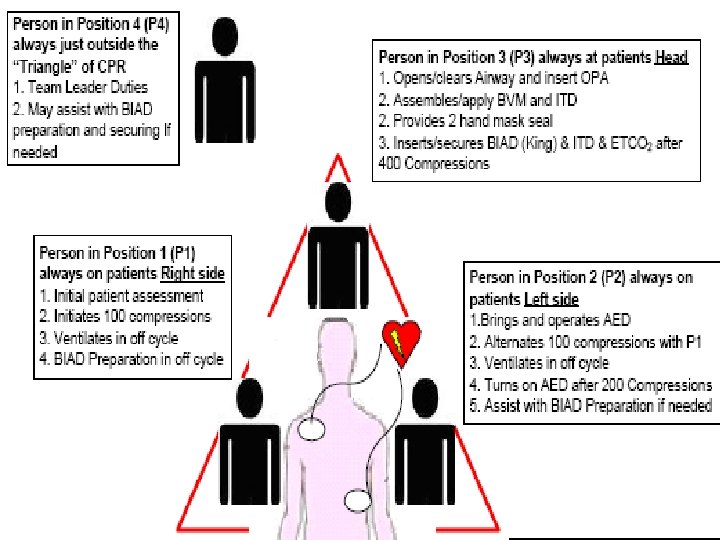
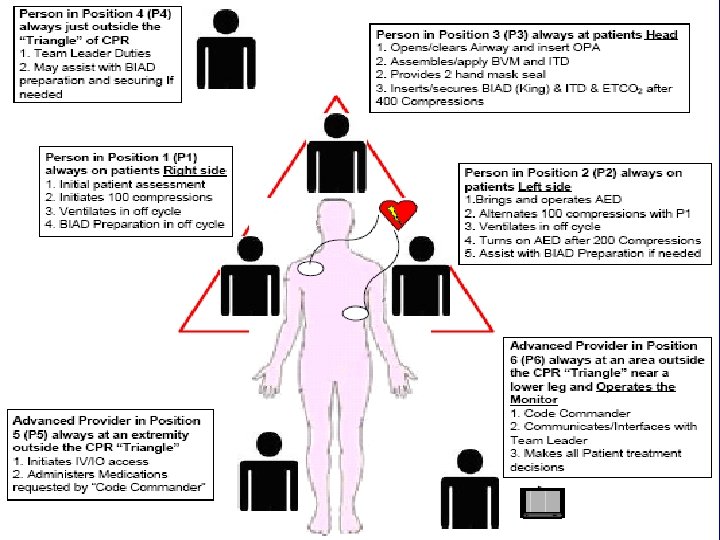
Pit Crew CPR n n Went to simulation to design highly scripted process that allows intervention without interruption Tasks assigned to positions rather than individuals because individuals change

OOHCA What matters! n For first 2 cycles concentrate on compressions – – – Get on the chest as quick as possible Compress hard and fast (do NOT exceed 120) Minimize interruptions n n If on monitor compress up to delivery of shock Resume compressions immediately regardless of pulse or rhythm – BVM ONLY – Control ventilation (use your blinky light)
 place King Airway – –")
OOHCA What matters! n After 2 cycles (4 min) place King Airway – – n Don’t stop compressions! ETI only if unsuccessful with BIAD Place gastric tube via KING or OG/NG Control your ventilations Recheck tube with each patient movement

OOHCA What matters! n Continue resuscitation – – n Rhythm/Pulse check only at 2 min Change compressor q 1 min regardless of fatigue Run checklist to assure overlooked errors Careful consideration of causes Do NOT move the patient unless: – You are in potential danger – You are in a public place – Other situation not suitable to leave the body
- Slides: 106