NEONATAL RESUSCITATION NEONATAL PROCEDURES PRESENTED BY MRS BENAZEERA

NEONATAL RESUSCITATION

NEONATAL PROCEDURES PRESENTED BY MRS. BENAZEERA ASSISTANTPROFESSOR DEPT. OF YENEPOYA NURSING COLEGE

LEARNING OBJECTIVES 1. Recall the purpose of Neonatal resuscitation 2. Identify the indication of Neonatal resuscitation 3. List down the article needed for Neonatal resuscitation. 4. Explain the techniques of Neonatal Resuscitation procedure

PURPOSES TO INITIATE RESPIRATION IN A NEWBORN WHO IS ASPHYXIATED OR SPONTANEOUS BREATHING HAS NOT INITIATED.

INDICATIONS • ANTEPARTUM FACTORS • INTRAPARTUM FACTORS

PREPARATION FOR RESUSCITATION • TWO TRAINED PERSONNEL NEEDED • KEEP READY RESUSCITATION EQUIPMENTS

Articles 1. ü ü ü Suctioning Articles: Bulb syringe, suction catheter No 6, 8, 10 mechanical suction

Articles 2. Bag and mask articles ü Infant resuscitation bag with pressure release valve with reservoir. ü Oxygen face mask newborn size ü oxygen with flow meter and tubing

Articles 3. Intubation articles ü Laryngoscope with straight blades ü Extra bulb and batteries for scope, ü Endotracheal tube size-2. 3, 3. 0 and 4. 0 mm]

Articles 4. Medication ü Epinephrine 1: 10. 000 ampoules. ü Normal saline ü Ringer’s Lactate ü Sodium bicarbonate 4. 2. / ü Dextrose 10. /. concentration 250 ml , sterile water 30 ml.

Articles 5. Miscellaneous: ü Radiant warmer ü Stethoscope ü Adhesive tape ü Bandage ü Scissors ü Syringe 1 ml, 5 ml and 20 ml sizes ü Needles No: 21, 22 and 26 G ü Umbilical cord clamp ü Gloves ü warm dry towel

TECHNIQUES OF RESUSCITATION

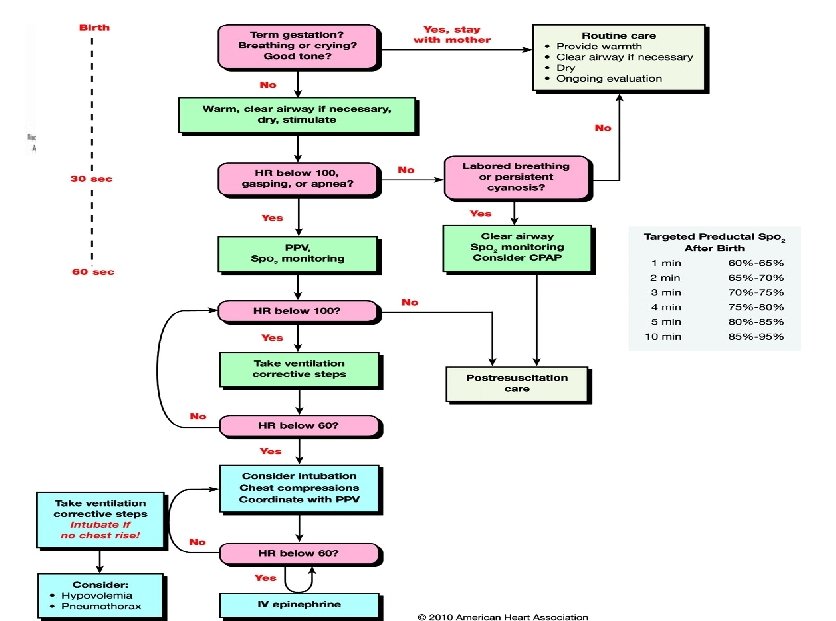
SIGNS TO EVALUATE • PERFORMED WITHIN FEW SECONDS • FIVE QUESTIONS TO BE ANSWERED v Is the amniotic fluid clear of meconium? v Is the newborn breathing or crying? v Is there good muscle tone? v Is the colour pink? v Was the newborn at term?

YES ROUTINE CARE • PLACING NEWBORN ON MOTHERS ABDOMEN • DRYING AND COVERING • WIPING NEWBORN MOUTH AND NOSE USING CLEAN CLOTH

NO INITIAL STEPS OF RESUSCITATION

PROVISION OF WARMTH • • • PREHEAT THE RADIANT WARMER RECEIVE NEWBORN IN A DRY AND WARM LINEN PLACE BABY UNDER WARM SOURCE DRY BODY WRAP IN ANOTHER SHEET

POSITIONING • EXTEND THE HEAD BY PLACING ROLLED TOWEL UNDER SHOULDER

CLEARING AIRWAY • If no meconium - suction secretions from mouth and nose - mouth first then nose

üIf meconium present - suction before delivery of shoulders -continue initial steps of resuscitation ü If newborn is depressed -suction under supervision of laryngoscope -Intubate trachea and suction

TACTILE STIMULATION • SLAPPING /FLICKING THE SOLE OF THE FEET • GENTLY RUBBING THE BACK • IF NO RESPONSE START BAG AND MASK

ADMINISTRATION OF OXYGEN • ADMINISTER HIGH CONCENTRATION OF OXYGEN • REGULATE FLOW AT 6 L/MIN • USE MASK

CHECK HR, RESPIRATION, COLOUR • Spontaneous breathing with HR >100/min Continue administration of oxygen • If apnea/ gasping/cyanosis after 30 sec Assisted ventilation by bag and mask

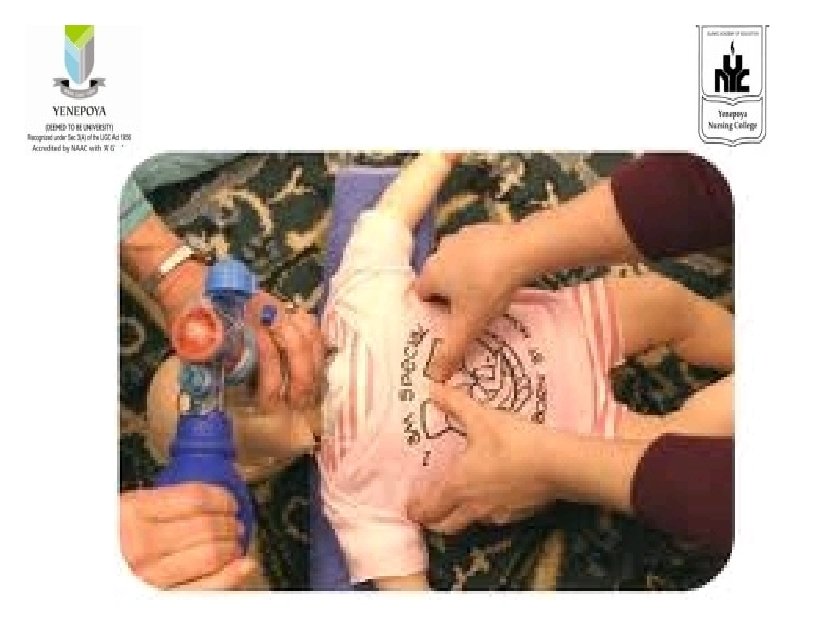
POSITIVE PRESSURE VENTILLATION • Cover the mouth, nose and tip of chin • Administer at a rate of 40 -60 /minute • Hold mask using left hand compress bag using finger tip

If no improvement in color, heart rate or breathing • Check for air leakage • Blocked airway • Inadequate pressure

• • • Reapply mask Reposition head Check for secretions Ventilate with mouth slightly opened Increase pressure of ventilation Recheck the resuscitation bag

Positive pressure ventilation for 30 sec Assess heart rate, color, breathing • HR >100, COLOR IMPROVING • HR< 60 • FREE FLOW OF OXYGEN • CHEST COMPRESSION

CHEST COMPRESSION • Firmly support neonates back • Two trained personnel needed-chest compression and vantilation

SITE • LOWER ONE THIRD OF STERNUM RATE • 3 CHEST COMPRESSIONS AND 1 BREATH • COMPRESS CHEST TO A DEPTH OF ONE THIRD OF A. P DIAMETER OF CHEST • EVALUATE AFTER 30 SEC • IF HR <60 CONTINUE CHEST COMPRESSION • IF HR >60 CONTINUE VENTILLATION

METHODS TWO FINGER THUMB TECHNIQUE

INDICATIONS TO SUCTION TRACHEA SUSPECTED DIAPHRAMATIC HERNIA NON RESPONSE TO BAG AND MASK VENTILLATION PROLONGED POSITIVE PRESSURE VENTILLATION REQUIRED • ADMINISTER EPINEPHRINE • •

MEDICATIONS • ADRENALINE – STIMULATE HEART • NALOXONE - POOR RESPIRATORY EFFORT NARCOTIC ADMINISTRATION TO MOTHER • VOLUME EXPANDERS- ACUTE BLOOD LOSS

TERMINATION OF RESUSCITATION • IF HR NOT IMPROVED WITH CENTILLATION AND CHEST COMPRESSION AND ADRENALINE • NO HR AND BREATHING AT BIRTH AND NOT INPROVED AFTER 10 min OF RESUSCITATION

https: //www. youtube. com/watch? v=euz. RICXcfg k

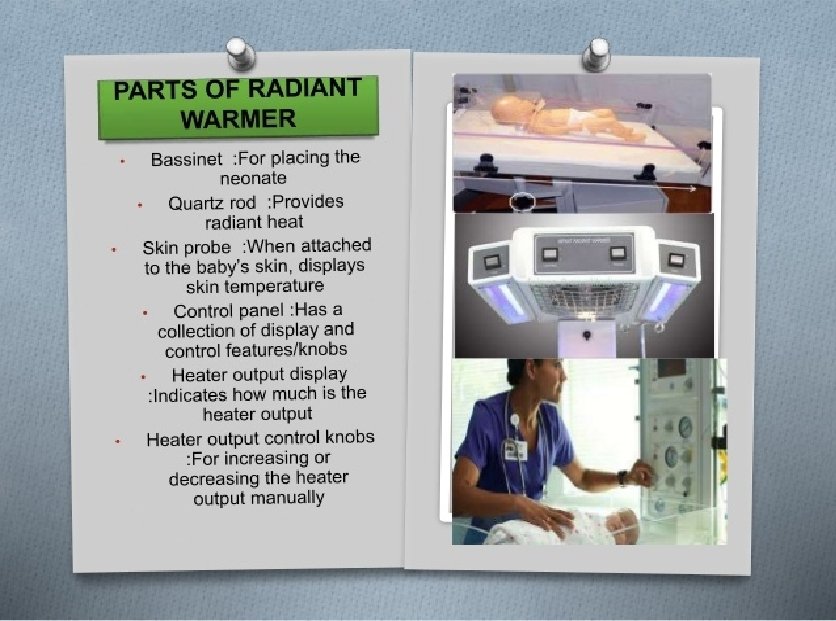
Radiant warmer

Learning objectives 1. 2. 3. 4. Define radiant warmer Explain the purpose of radiant warmer List down the parts of Radiant warmer Discuss the care of neonate in radiant warmer

Definition The radiant warmer is a electronically based device which is used to maintain the body Temperature.

Purposes 1. To maintain the body temperature just after the birth 2. To observe the child under the proper light source 3. To suction or resuscitation the baby in case of any obstruction or cyanotic episode. 4. To introduce the medication for long duration e. g. : IV administration

Care of the child in Radiant warmer 1. Check the physician order and instruction 2. Keep the warmer on before placing the baby and set the temperature as prescribed 3. Place the sheet over the mattress and tuck it properly 4. Raise the side rails properly 5. Place the baby carefully on the mattress 6. Do the observation of baby under the observation light

7. Provide the feed to the baby intermittently to prevent the dehydration 8. Do not touch the child without hand washing. 9. Maintain hygiene of the child 10. Attend the alarming sign when in on conditions.

Care of child with incubator

Introduction üIncubator is an apparatus for maintaining an infant, especially a premature infant, in an environment of controlled temperature, humidity, and oxygen concentration. üIncubators have simple alarm system to alert the clinical staffs if there is any danger of overheating of the device.

Principle of Incubator 1. Infant incubator helps to protect the baby from noise, infection, and excessive handling. 2. Temperature is controlled machine

Purpose of Incubator ü Maintain their own temperature with clothing and wrapping. üclose observation. üRisk of abnormal heat loss. üInfection/ or the potential to develop sepsis.

TYPES OPEN BOX

TYPES Portable and non portable

Close type

STEPS Step: 1: Prepare the incubator 1. Pre-warmed to a temperature appropriate to the infant’s age, size and condition. 2. Use in Air mode and must always be switched on with the motor running if in use for a baby. 3. Check and record the incubator temperature hourly. 4. Position away from draughts or direct sunlight

STEP 2: Care of Baby 1. Maintain axilla temperature between 36. 5°C and 37. 2°C 2. Access baby by using the portholes, limit opening of large door as this interferes with air temperature. 3. Ensure baby is nursed naked apart from a nappy. 4. Position baby utilizing rolled towels/cloth nappies to provide boundaries that support ‘nesting’ and flexion of limbs but keeping face clear

STEP 3: Adjusting incubator temperature in NICU is 35 degrees �Re-check the temperature within half an hour of making any adjustment.

STEP 4: Monitoring �Axilla temperature is taken on admission into the incubator and rechecked in the first hour. �Temperature is documented 4 -6 hourly as per the condition.

STEP 5: Use of Humidification Is utilized for incubator care of preterm babies only – NOT required for babies >32 weeks.

Cleaning and sterilization �When the incubator is occupied, it should be cleaned daily with mild detergent. �Humidifier chamber must be emptied and cleaned daily, fill with fresh distilled water.

Cleaning and sterilization �After seven days neonate should be sifted to another incubator and used incubator should be cleaned with antiseptic solution. � 1 -2 ml of Glacial acetic acid or vinegar can be added to water in the humidifier to prevent bacterial growth.

Phototherapy Care for the infant under phototherapy

Objectives 1. 2. 3. 4. 5. 6. Define phototherapy List Indication of phototherapy Understand the mechanism of phototherapy List the benefits of phototherapy Enumerate the side effects of phototherapy Apply the nursing care for infant’s receiving phototherapy Care for the infant under phototherapy
 is a way of treating jaundice. Special lights")
What is phototherapy? Phototherapy (light therapy) is a way of treating jaundice. Special lights help break down the bilirubin in baby's skin so that it can be removed from his or her body. This lowers the bilirubin level in your baby's blood. Care for the infant under phototherapy

What is phototherapy? Application of fluorescent light to the infant’s exposed skin used to breakdown the bilirubin in the skin Care for the infant under phototherapy

Indication of phototherapy • Treatment of Hyperbilirubinemia • The phototherapy will help the liver to process bilirubin, bringing your baby's level down to normal • Prevent Kernicturus Care for the infant under phototherapy

M E C H A N I SM O F WORKING Care for the infant under phototherapy

Assessment should be Before Phototherapy • • • GA Of the baby Weight The baby Postnatal Age Types of Jaundice the level of jaundice Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy Proper covering and shielding of gonad. Assessskin exposure. Proper position. Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy Cont’ Assessand adjust thermoregulation device. Promoting elimination and skin integrity. Hydration. Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy. -Assure effective of phototherapy -provide eye protection Eyes are covered with eyepatches to prevent damage to the retina by the. Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy- continue • Baby is placed naked 45 cm away from the tube lights in a crib or incubator. • If using closer, monitor temperature of the baby. • Baby is turned every two hours or after each feed. Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy • During phototherapy, the bilirubin level in baby’s blood will be checked at least once every day. Phototherapy is stopped when the bilirubin level decreases. Care for the infant under phototherapy

Nursing Care for Infant Receiving Phototherapy • Temperature is monitored every two to four hours. – Weight is taken at least once a day. – More frequent breastfeeding or 10 -20%extra fluid is provided. – Urine frequency is monitored daily. • Serum bilirubin is monitored at least every 12 hours. • Phototherapy is discontinued if two serum bilirubin valuesare<10 mg/ dl. Car e or f theinfan t nder u phot other apy

Promoting infant parent interaction. Care for the infant under phototherapy

Side effect of phototherapy • • Bronze – baby syndrome. Loss , greenish stool. Transient skin rashes. Hyperthermia. Increasing metabolic rate. Dehydration. Electrolyte disturbance. Care for the infant under phototherapy

Exchange and transfusion

Exchange transfusion is replacement of circulating blood by withdrawing blood and injecting donor’s blood in equal amounts.

Purposes 1. To prevent accumulation of bilirubin in the blood above dangerous level 2. To prevent kernictures. 3. To prevent hemolysis 4. To raise the HB levels at birth when HB is less than 15 mg 5. To replace red blood clots which have poor oxygen releasing capacity.

• To remove toxic metabolism • To treat irreversible acidosis, sepecticemia • Neonatal jaundice with serum bilirubin level of 20 mg/dl or more in full term and 15 mg /dl in preterm infants[Rh OR ABO incompatibility. • Hemolytic disease of the newborn-cord HB 10. /. or less, cord bilirubin 5 mg/dl or more

Article ü Blood exchange transfusion kit containing – Bowel, kidney tray, suture scissors, toothed forceps, curved mosquito forceps, dressing forceps, surgical towel, syringes 10 and 20 cc, pads and bandages. ü Dressing pack ü Sterile scalpel blade ü I. V stand

Article • • Injection Heparin and normal saline Resuscitation equipments Oxygen source. 3 or 4 way stopcock Umbilical vein catheter Gloves and mask Specimen container Cord tie

Article • Scissor to cut the adhesive plaster • Emergency drugs –Adrenalin, calcium gluconate, Inj aminophylline • Fresh blood for transfusion.

CARE AND PROCEDURE ü Procedure should be explained properly to the parents and care taker. ü Take the informed written consent from the parents as per the international accepted rights of children ü The blood of donar should be cross matched. ü The blood should be fresh and not more than 5 days old ü Immobilize the baby on cross splint

CARE AND PROCEDURE ü Do the cleaning of umbilical stumps by the dressing pack. ü The all apparatus should be primed with the saline and heparin injection in a bowl, to prevent sticky. ü Now cut the umbilical cord less than 2. 5 cm from the skin surface. ü Attach the ligature and insert the catheter into the vein

CARE AND PROCEDURE • Fill the catheter with donor blood before procedure to prevent from air embolism • Do the transfusion. • Record the central venous pressure after the insertion of catheter • Check the vital signs and conditions of the baby • Test the blood sample after and pre-procedural blood----check Hb & biliubin level.

CARE AND PROCEDURE ü Remove the catheter and give the cord tie at umbilicus, apply tincture benzoin at umbilicus and secure with adhesive tape. ü Keep the equipment in proper after wash ü Do the proper recording and reporting.

Important point during procedure v. Blood should be slowly warmed to the infants body temperature v. Fresh heparinized blood is used. v. About 20 -30 ml of blood is with-draw and about 10 -20 ml blood is placed each time v. After transfusion place the baby in a radiant warmer v. Observe the umbilicus for finding and bleeding

complication Ø Umbilical vein perforation Ø Cardiac arrest Ø Hypoglycemia, Hypocalcaemia Ø Bacterial sepsis Ø Metabolic acidosis Ø Thrombocytopenia

BABY BATH � INTRODUCTION Child rearing practices during the first year vary from country to country. The amount of bathing that is done is also inconsistent across cultures. Unless contra indicated most infants and children can be bathed in a basin at the bedside or on the bed, or in a standard bath tub located on the unit which is often conveniently adapted for pediatric use.

DEFINITION � B a b y bath is defined as cleaning the skin of the baby for promoting hygiene and comfort in the home setting.

OBJECTIVES 1. To keep the baby’s skin clean. 2. To refresh the baby. 3. To stimulate the circulation. 4. To prevent any skin infection. 5. To closely observe the body for evidence of any abnormalities and to note infant’ growth and development. 6. To induce sleep.

ASSESSMENTOFTHESKINBEFORE BATH � Colour � Moisture � Temperatu re � Texture � Turgur � Vascularity � Edema � Pruritis

� Rashes � Lesions � Erythema � Infection � Inflammatio n � Hirutism

TYPESOF BATH LAP BATH Bathing the baby keeping on the lap. Here the mother sits on a stool and can sponge and change his dress on her lap itself. So there is no need of having additional stool.

� SPONGE BATH Bathing the child in bed.

TUB BATH This is the common method of giving bath to the baby.

GENERALINSTRUCTIONSFOR GIVING BATH � U s e warm room and warm water. � B a t h quickly and gently. � D r y quickly and gently. � N e v e r leave the baby unattended in a bath tub or table. � T h e infant is given bath after the cord falls and umbilicus is well healed. (within 7 th-10 thday. )

� T h e ideal time for bathing a baby is before the second feeding; taking care that the baby is not tired or hungry. � B a b y should not be bathed within an hour he is fed because moving may cause vomit. � T h e r e should be a fixed time for bath, which will help the baby to form a habit on an orderly schedules.

� T h e newborn’s temperature regulating system is underdeveloped, So meassure the temperature of water to avoid overheating or chillness. 98 -100 or 37 -38 ) � T h e clothing should be selected based on the environment and weather. � T h e soap used should be mild and without hexachlorophene base and avoid using talcum powders, because it containes zink stearate which irritates the respiratory tract.

ARTICLESREQUIRED � H o t water � T e p i d water � Buckets-2 � Mug-1 � M i l d soap � H a i r oil � S w a b sticks-4. � C o t t o n balls.

� K-basin � Thermomet er � C l e a n cloths � Betadine � N o r m a l saline � L o w stool � Apron

PRELIMINARYASSESSMENTOFTHE CHILD ANDSITUATION � Identify the child and check doctor’order for any specific instruction about bathing the baby. � G e t further instructions from the ward sister. � Assess the general condition of the baby and need for bathing. � F i n d out from the mother whether the child had his feeding within the previous one hour.

� D e c i d e the type of bath to be given and find out the proper place for the same. � C h e c k the articles in the unit. � Collect the individual soap and towel from the mother if possible.

PREPARATIONOFTHE ENVIRONMENT AND EQUIPMENT � C l o s e windows to keep off draught and to provide privacy. � Collect all the articles in readiness before beginning the procedure. � K e e p the table against the wall, place the tub or basin on one end of the table and the tray with articles on the other end conveniently so that the baby will be protected on 3 sides and there is less chance of the baby’s rolling of the table.

� P l a c e makintosh and towel over the table, wash hands and wear apron. � S e e whether the baby is wet with urine or motion. If so clean the part. � B r i n g the baby wrapped in a towel to the bath table.

NURSING ACTION 1. Explain procedure to the mother and encourage her Participation. RATIONALE 1. To reduce anxiety and to win co-operation.

NURSING ACTION RATIONALE 2. Pour water into the tub and adjust temperature by checking with the elbow or dorsal side of the palm. 2. Prevents chances of hypothermia or scalding.

� N u r s i n g action 3. Undress the baby. 4. Place the head of the baby on your nondominant palm and support the body with the forearm. Rationale 3. To made ready for bath 4. Safeguards the baby from slipping.

� NURSING ACTION 5. Close ears with the thump and middle finger of the nondominant hand. RATIONAL 5. Prevents entry of water.

NURSING ACTION 6. Wipe the eyes from inner canthus to outer canthus with cotton swabs. 7. Dip hand in water and wipe face taking care that no water goes into the mouth of infant. RATIONALE 6. It prevents entry of debris and microorganisms into the lacrimal gland. 7. Follows the principle less contaminated to most contaminated area.

NURSING ACTION RATIONALE 8. Wet hair and apply soap or shampoo gently wash the scalp. Rinse with water and dry hair with towel. 8. Drying immediately prevents hypothermia.

NURSING ACTION 9. Place the baby into the tub with shoulders neck and head supported by the nondominant hand the trunk and legs in water. RATIONALE 9. To start washing trunk.

NURSING ACTION. 10. Wet the baby’s neck, chest, hands, abdomen, legs and perineum. 11. For cleaning back and buttocks transfer the baby to the other hand in such a way that neck and chest are supported over the palm, by holding the baby securely. RATIONALE

NURSING ACTION 12. Apply soap concentrating on skinfolds and rinse with the water 13. Spread the towel over a flat surface. Place the baby on it and dry. RATIONALE 12. prevents skin irritation. 13. For better covenience

NURSING ACTION RATIONALE 14. With the swab 14. To prevent umbilical infection. stick swab the inner and outer circle of cord. . 15. and cover in the Dress the baby blanket or towel. 15. To prevent from hypothermia.

CONTRAINDICATIONS OFBABY BATH � Hypothermia. � Convulsions. � Bronchopneumonia. � Congenital cyanotic heart desease. � F r e s h burns. � Critical illness. � P r e m a t u r e infants.

AFTERCARE � W a s h and replace the articles in the proper place. � R e c o r d the type of bath, any abnormal findings on the skin with date and time. � H a n d over the baby to the mother for feeding. � B e f o r e discharge demonstrate it to the mother, so that she can bath her infant at home.

CONCLUSION • Bathing provides a opportunity to the nurse to identify any developmental peculiarities and superficial skin infections which should be brought to the notice of physician.
Little")
BIBLIOGRAPHY 1. Adelli Pilliteri, ‘MATERNAL NEWBORN NURSING, CARE OF GROWING FAMILY’ 2 NDED. (1976)Little Brown and company, Philadelphia. 2. Adelli Pillitteri, CHILD HEALTH NURSING, CARE OF THE CHILD AND FAMILY, Lippincot, (1999)Los Angels. Californi. 3. Dorothi. R. Marlow , Barbara. a. Reeding ‘TEXT BOOK OF PEDIATRIC NURSING(1988)W. B. Saunder’s company, Philadelphia. 4. Hockenberry Wilson ‘wong’s nursing care of infants and childre’ 8 th ed. (2007), mosby publishers.

5. C. P. Thresiamma, FUNDAMENTALS OF NURSING PROCEDURE MANNUAL FOR GENERAL NURSING AND MIDWIFERY COURSE, (2003), 2 nd ed. jaypee publishers, Newdelhi. 6. O. P. Ghai, Paul v. k, Piyush Guptha, ’GHAI ESSENTIALS OF PEDIATRICS(2005), 6 th ed. CBC publishers, New Delhi. 7. Annamma Jacob, ‘CLINICAL NURSING PROCEDURES, THE ART OF nursing’ 2 nd ed. Jaypee Publishers, newdelhi. 8. Meharban Singh ’Care If New Born’(2004)6 th ed. Sagar publications, newdeihi. 9. CMC ‘procedure mannual’Vellore.
- Slides: 123