Oral Surgery GIL Contents Preop Medical assessment Case










 ● Relation to")




















- Slides: 32
Oral Surgery GIL
Contents ● Pre-op ○ ○ ○ Medical assessment Case selection ■ Clinical + Radiographic assessment Consent ● Simple Extractions ● Complex Extractions ● Post-op
Pre-op assessments ● Aim of pre-op assessments: ○ ○ Ensure the exo is safe for the patient Ensure exo is achievable for your level of skill and experience ● Medical assessment ○ ○ Contraindications for extractions Medications/Med treatments that are significant to oral surgery ■ Blood thinning medications ■ Bisphonates ■ Radiotherapy
Contraindications ● Absolute vs Relative ○ definition ● Systemic contraindications ○ ○ Uncontrolled Metabolic diseases Myocardial infarction Lymphoma and leukemia Severe coagulopathy eg. bleeding diathesis ● Local contraindications ○ ○ Radiation zone tumour/cancer Severe infections Severe abscess
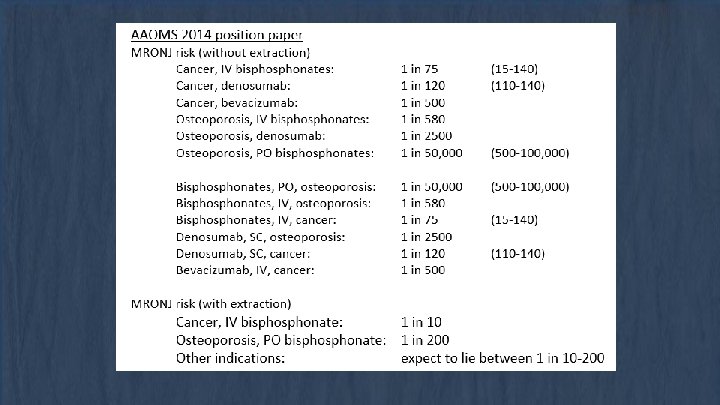
Medications - Bisphonates ● Bisphonates ○ ○ Types ■ N containing vs non-N containing ■ Mode of administration Bisphonates in clinical setting ■ Generic name and Brand name ● Denosumab vs bisphonates ○ Mode of actions ○ Reasons for prescription ● CTX (C-terminal telopeptide crosslinks) ● MRONJ
Medications - Blood “thinners” ● Anti-platelets vs anti-coagulants ○ ○ Differences in mechanism of action Primary vs Secondary Haemostasis ● Types of anti-platelets ○ ○ ● Aspirin: Irreversible cyclooxygenase inhibitors ■ Classed as NSAIDS Clopidogrel: Adenosine diphosphate receptor inhibitors Types of anti-coagulants ○ ○ ○ Warfarin: Vit K epoxide inhibitor Apixaban and Rivaroxaban: Direct Factor Xa inhibitor Dabigatran: Direct thrombin inhibitor ● INR test ● Management of patient on blood thinner
Coagulation cascade
Medications: Blood “Thinners” ● Assessment ○ What questions should you ask a patient taking blood thinners? ● Management ○ ○ Anti-platelets ■ Ensure patient maintains normal dosing of medication unless otherwise instructed by doctor/medical specialist ■ Achieve haemostasis via local measures Anti-coagulants ■ Warfarin ● Check INR levels and treat if in therapeutic range 2 -4 ● Use of tranexamic acid protocol ■ Apixaban, rivaroxaban, dabigatran, heparin, clopidogrel ● No INR test available ● Weigh need for continuous anticoagulation vs need for blood clotting during exo
Radiotherapy ● Patient undergoing radiotherapy in the head and neck region have a risk of developing Osteoradionecrosis of the jaw ● Effects of radiation to head and neck ○ ○ Loss of fine vasculature ■ Adversely affects bone, salivary glands and jaw Dosage vs risk of developing post-op adverse reactions (>5000 rad) ● Treatment planning ○ ○ ○ Before radiation therapy During radiation therapy After radiation therapy ● Signs of necrosis of the jaw
Clinical evaluation ● Access to tooth ○ ○ ○ Mouth opening Inclination of tooth crowding ● Mobility of tooth ○ ○ Hypermobility usually noted in pts with periodontal disease - usually uneventful exos Hypomobility cases should be more carefully evaluated for… ■ Hypercementosis ■ Ankylosis ● Condition of crown ○ ○ Strength of crown ■ Caries or loss of tooth structure ■ Restorations Adjacent teeth ● Age of patient
Radiographic evaluation ● PA or OPG (adv and disadv of each) ● Relation to vital structures ○ ○ ○ Floor of Mx sinus Inferior Alveolar Nerve and vascular bundle Mental foramen ● Evaluation of roots ○ ○ ○ ○ Number of roots Shape of roots Curves + divergences Size Evidence of root caries Root resorption Previous endodontic therapy radiographic signs associated with inferior alveolar nerve damage following lower wisdom tooth extractions
Radiographic evaluation ● Evaluation of surrounding tissues ○ ○ ○ Bone ■ Density of bone Acute periapical pathology Any pathology of surrounding tissues ■ What kinds of pathology noted on a radiograph might affect your treatment?
Consent ● How to gain informed consent? ○ ○ ○ What is the problem? What are the treatment options What they will expect during each treatment option What will they expect after tx What Risks are there for the treatments ● No treatment can proceed without patients consent. Consent can also be revoked at any time of treatment. ● What risks and adverse events can happen with exo?
Risks and Adverse reactions re: Extractions ● Iatrogenic damage ○ ○ ○ Slipping of instruments Overzealous use of instruments Incorrect use of instruments ● Swallowing of tooth and instruments ○ Inhalation - asphyxiation or infections ● Damage to vital structures ○ ○ OAC Nerve damage ● Displacement of tooth/root ○ ○ ○ Mx sinus Infratemporal space Submandibular space ● Inability to remove all or part of tooth
Local Anaesthesia ● Mandibular ○ ○ IANB, Lingual, Long Buccal Blocks Infiltrations ● Maxilla ○ Buccal and Palatal Infiltrations ● Failed anaesthesia ○ ○ Intraligamental Intrapulpal
Procedures of Simple Extractions 1. Loosening of soft tissue attachment from cervical portion of tooth 2. Break PDL 3. Break interdigitation of bone via expansion of socket a. Luxating the tooth b. Wedging c. Use of dental forceps 4. Delivery of tooth via extrusive force a. Specific technique for different teeth
Instruments ● Elevators ○ ○ ○ Straight: Luxator, Couplands Curved: Cryer, Warwick James Picks: Root picks ● Forceps ○ ○ Various Not all types of forceps available at ADH ● Handpieces ○ ○ Impact Air Surg. XT
Elevators ● D/d ∝ F ○ D = diameter of blade, d = diameter of handle ● Used to expand socket through various movements
Couplands ● Designed for wheel and axis motions ● Place in so that both blades touch the tooth (roughly perpendicular to long axis)
Luxator ● Designed to wedge and lever ● ● Tip should be parallel to long axis of tooth Expands socket Breaks PDL Pushes tooth out
Cryer and Warwick James ● Used to gain access to posterior teeth as they are curved ● Essentially uses the pointy tip to elevate teeth out ● Relies on wheel axle motions due to design
Forceps ● Mx ○ ○ ○ Upper uni Stubbies Right, Left Upper molar Root forceps ● Md ○ ○ ○ Lower anterior Lower molar Hawksbill Cowhorn Root forceps
Forceps ● Choose angle depending on location of tooth ● Shape of blade important ○ Want them to encircle crown as much as possible ● Movements ○ ○ Apical Torsional ■ Safe movement, unlikely to break tooth (single rooted teeth) Lateral ■ Bucco-palatal ■ Risk of tooth breaking but should be mobile at this point ■ Figure 8 on lowers Tractional
Apical ● Prevents fracture by pushing centre of rotation apically
Circular roots ● Anterior, lower premolars
Oval Roots ● Upper premolars
Upper molar ● 3 roots
Lower Molar ● 2 roots
Post-ops ● “Oh, thank God it’s out” ● Surgicel? ○ ○ Blood thinners TXA if warfarin ● Sutures? ○ ● ● Loose gingiva usually promotes healing Gauze for 30 mins - 1 hour Salt water rinse No smoking or alcohol Etc
Surgicals 1. Assess the tooth a. Planning essential, should know exactly what you are doing before touching the patient b. Determine whether bone needs to be removed c. Section tooth 2. Visualisation and Access a. May require flap to be raised b. 2 anterior 1 posterior or 1 anterior and 1 posterior if relieving incision placed 3. Bone Removal a. May not be required 4. Deliver Tooth 5. Smoothen sharp edges on bone 6. Suture
Happy Exo!