New Treatment for HCV G 4 Towards an







 This study done on 60")
 Naïve 84% Arm 1 (12 wks) Overall 77%")





 AUC No of patients Best cutoff")











")










- Slides: 40
New Treatment for HCV G 4 Towards an End to HCV Epidemic in Egypt
Several potential innovative drug targets in HCV NS 2 c E 1 NS 3/4 A A serine protease, essential for posttranslational processing of HCV polyproteins Boceprevir 1 Telaprevir 1 ABT-450/r 2 Sovaprevir 3 Asunaprevir 11 Simeprevir 9 Faldaprevir 12 Danoprevir 12 GS-945113 MK-517214 ACH-806/GS-91321 NS 3 IFN-lambda NS 5 A NS 5 B A type III interferon with a restricted distribution of receptors contributing to a favourable adverse event profile 7 E 2 NS 5 A NS 5 B Multifunctional membrane. An HCV-specific, RNA-dependent associated phosphoprotein, RNA polymerase essential component of the HCV-RNA replication complex Daclatasvir 4 Ledipasvir 4 ABT-2672 PPI-6686 AZ-6894 BMS-8243934 PPI-4614 Nucleos(t)ide analogue Sofosbuvir 10 Mericitabine 15 VX-13520 Non-nucleoside analogue BI-20712716 ABT-3332 ABT-07217 BMS-79132518 Tegobuvir 12 Setrobuvir 12 VX-22219 Filibuvir 12 BMS-9141438 Cyclophilin A Host protein involved in HCV replication through interaction with NS 5 A and the HCV polymerase Alisporivir 5, * SCY-6351 *On clinical hold, Novartis press release 1. Rehman S, et al. Genet Vaccines Ther 2011; 9: 11. 2. http: //clinicaltrials. gov/ct 2/show/NCT 01464827. 3. http: //ir. achillion. com/releasedetail. cfm? releaseid=6989383. 4. Gish R & Meanwell NA. Clin Liver Dis 2011; 15: 627– 39. 5. Coelmont L, et al. PLo. S One 2010; 5: e 13678. 6. http: //clinicaltrials. gov/ct 2/show/NCT 01448200. 7. Miller DM, et al. Ann N Y Acad Sci 2009; 1182: 807. 8. http: //clinicaltrials. gov/show/NCT 01309932. 9. Poordad F, et al. AASLD 2012, abstract 83. 10. Gane E, et al. EASL 2012, poster 1113. 11. http: //clinicaltrials. gov/ct 2/show/NCT 01030432. 12. Delang L, et al. Viruses 2010; 2: 826– 66. 13. http: //www. gilead. com/research. 14. http: //clinicaltrials. gov/ ct 2/show/NCT 01353911. 15. Wedemeyer H, et al. Hepatology 2013 January 24. [Epub ahead of print]. doi: 10. 1002/hep. 26274. 16. http: //www. pipelinereport. org/browse/hcvtreatment/bi-207127. 17. http: //www. pipelinereport. org/browse/hcv-treatment/abt-072. 18. http: //clinicaltrials. gov/show/NCT 01193361. 19. http: //www. vrtx. com/researchdevelopment/pipeline. 20. http: //news. bms. com/press-release/financial-news/bristol-myers-squibbpresent-new-data-hepatitis-c-and-hepatitis-b-compo. [Accessed April 10, 2013].
Characteristics of DAA PI 1 st generation PI 2 nd generation NS 5 A Inh. 1 st generation NS 5 A Inh. 2 nd generation NS 5 B nucleos(t)ide inh. NS 5 B non nucleos(t)ide inh. Efficacy Resistance profile Pangenotypic efficacy Adverse events Drug-drug interaction Good profile Average profile Least favorable profile Schinazi, et al. Liver Int 2014; 34 Suppl 1: 69 -78
Many studies have looked at different ways of combining these compounds NS 5 A NS 3/4 A RBV Alfa • Different genotypes NS 3 /4 A • Treatment-naive Alfa a L In different patient types NS 5 A bd am RBV Lambda NS 5 A V RB RBV NS 5 A NS 3/4 A • Intolerant to previous therapy NS 5 B ( inh nuc ibi tor ) NS 5 B (non-nuc inhibitor) • Null-responders to prior therapy RB V Lambda 5 A NS NS 3/4 A RBV A /4 S 3 N Alfa, peginterferon alfa-2 a; lambda, peginterferon lambda-1 a; RBV, ribavirin This slide represents just a small selection of studies and regimens in current clinical development – other combinations are therefore possible
Sofo+RBV Study Patients Regimen Duration Sofosbuvir and Ribavirin for Hepatitis C Genotype 1 in Patients With Unfavorable Treatment Characteristics Osinusi (2013) JAMA No: 60 treatment-naive patients genotype 1 with bad predictors: (African-American, high BMI, low frequency of IL 28 B CC, viral load and advanced fibrosis) 60 patients Egyptians G 4 Treatment naive and experienced A: 10 non cirrhotic B: 50 All stages of fibrosis: 25 (weight based RBV) 25 (low dose RBV: 600) 12 weeks Sofosbuvir + RBV 12 weeks Or 24 weeks 12 weeks SVR 12 68% 24 weeks SVR 12 93%: G 4 100 patients Treatment naive and experienced Sofosbuvir + RBV 12 weeks Or 24 weeks 12 weeks SVR 12 77% 24 weeks SVR 12 90% Sofosbuvir plus ribavirin in the treatment of chronic HCV genotype 4 infection in Egyptian patients Ruane (2013) Hepatology Egyptian study Response SVR 24 Non cirrhotic: 90% Wight based RBV: 68% Low dose RBV: 48%
Sofo+IFN+RBV Study Patients Regimen Duration Response ATOMIC 316 naïve Sofosbuvir with pegylated genotype-1 interferon alfa-2 a and ribavirin for treatment-naive patients with hepatitis C genotype-1 infection (ATOMIC): an openlabel, randomised, multicentre phase 2 trial Kowdley et al (2013) Lancet A (N: 52): sofosbuvir 12 w +P+R 24 weeks B (N: 109, with 11 of 24 weeks (12 +12) them genotype 4): sofosbuvir +P+R C (N: 155): 12 weeks of sofosbuvir +P+R followed by 12 weeks of either sofosbuvir monotherapy or sofosbuvir +R SVR 24 A: 89% B: 89% C: 87% NEUTRINO Sofosbuvir for previously untreated chronic hepatitis C infection Lawitz (2013) NEJM Sofosbuvir + Peg. IFN + RBV Total 90% (295/327) G 1 a 92% (206/225) G 1 b 82% (54/66) G 4 96% (27/28) G 5/6 100% (7/7) Cirrhosis 80% (43/54) G 1, 4, 5, 6 Naïve n = 327 (G 1 79%) 12 weeks
Sofo and other DAA combination trials Response Duration Regimen Patients Study Cirrhotic TTT failure: With RBV: 100% SVR 12 Without RBV: 70% SVR 12 Non cirrhotic naïve: 6 weeks ttt: 68% SVR 12 8 weeks ttt; 100% SVR 12 8 weeks with RBV: 100% 8 weeks without RBV: 95% 12 weeks Sofosbuvir+ ledipasvir With or without RBV G 1 prior null responders with compensated cirrhosis and in naive, noncirrhotic patients Electron Once daily sofosbuvir/ledipasvir fixed dose combination with or without ribavirin 8 weeks Sofosbuvir+ ledipasvir With or without RBV G 1 treatment-naive, noncirrhotic LONESTAR (2) Sofosbuvir and ledipasvir fixeddose combination with and without ribavirin in treatment-naive and previously treated patients with genotype 1 hepatitis C virus infection (LONESTAR): an openlabel, randomized, phase 2 trial Sofosbuvir+simeprevir with or without RBV G 1 Noncirrhotic and cirrhotic, treatment-naıve and prior null responder COSMOS (3) SVR results of a oncedaily regimen of simeprevir (TM 435) plus sofosbuvir (GS-7977) with of without ribavirin in cirrhotic and noncirrhotic HCV genotype 1 treatment naıve and prior null responder patients SVR 12 in prior null for 12 or responders with F 0 -F 2 24 weeks fibrosis were 93% (in both 12 and 24 weeks). In cirrhotics: SVR 4: 100% (in both null responders and naïve) 24 weeks. 1) (1) Gane (2013), Hepatology 2) Lawitz (2013), Lance, 3) Jacobson (2013), Hepatology
SOF + RBV: In genotype 4 SVR 12 (%) This study done on 60 Egyptians (G 4) living in USA 20% of them are cirrhotics. 21/31 12 Week SOF + RBV 27/29 11/14 14/14 24 Week SOF + RBV 12 Week SOF + RBV 24 Week SOF + RBV All Ruane PJ, et al. EASL 2014. P 1243 Ruane PJ, et al. AASLD 2013. Abstract 1090 Treatment naïve 10/17 12 Week SOF + RBV 13/15 24 Week SOF + RBV Treatment experienced Ruane PJ, et al. EASL 2014. P 1243
Sofosbuvir+ Ribavirin in G 4 (Egypt) Naïve 84% Arm 1 (12 wks) Overall 77% Exper 70% 100 patients (20% C, 3 centers) Naïve 92% Arm 2 (24 wks) Overall 90% Exper 89% (Esmat, et al AASLD. 2014)
• In 51 patients GT 4, received SOF + RBV for 12 weeks, SVR in 39 (77%) – Pts who were treatment naïve, Fibrosis stage<F 3, and baseline viremia <600, 000 IU were 9 pts. All showed SVR (100%) – Pts who were either treatment experienced, and/or fibrosis stage >F 2 and viremia level >600, 000 IU showed SVR (71%) (12 pts of whom 8 were treatment experienced) – P value 0. 01 (S)
0= naïve, Fibrosis <F 3, viremial<600, 000 IU 1= treatment experienced, and/or fibrosis ≥F 3, viremial >600, 000 IU
SOF STUDIES 1. Lawitz et al. DDW 2013. 2. Ruane et al. EAS L 2014. Poster 1242. 3. Esmat et al, AASLD. 2014 EGYPTIAN
Non invasive detection of hepatic fibrosis Fib-4 Formula http: //gihep. com/calculators/hepatology/fibrosis-4 -score/
Non invasive detection of hepatic fibrosis Fibroscan
Non invasive diagnosis of Advanced hepatic fibrosis(>F 2) AUC No of patients Best cutoff sensitivity specificity PPV NPV accuracy LR+ LR- *Fib-4 0. 71 36841 1. 45 0. 69 0. 63 0. 28 0. 90 0. 63 1. 9 0. 49 ♠Fibroscan 0. 82 231 9. 5 0. 82 0. 87 0. 68 0. 93 0. 86 6. 52 0. 20 Fibroscan Fib-4 ≤ 1. 45 >1. 45 ≤ 9. 5 Do not treat Wait or Do liver biopsy >9. 5 Wait or Do liver biopsy Treat *National Committee for control of viral hepatitis, NNTC data , Jan 2014 ♠ Esmat et al, Arab Journal of Gastroenterology 14 (2013) 109– 112
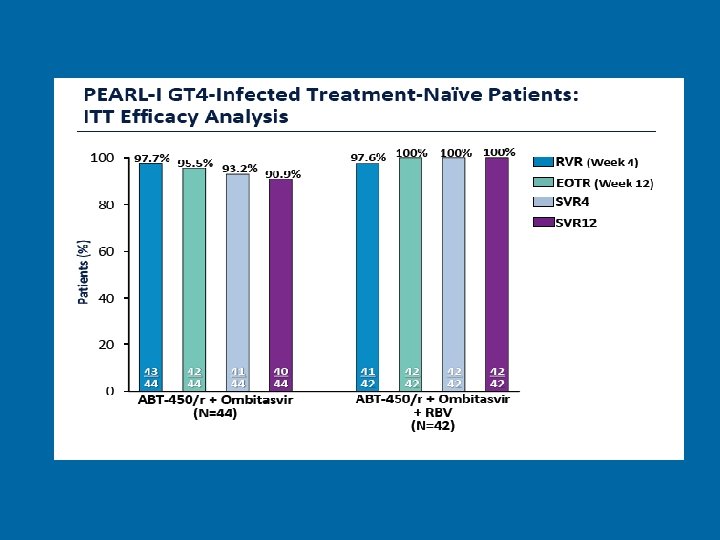
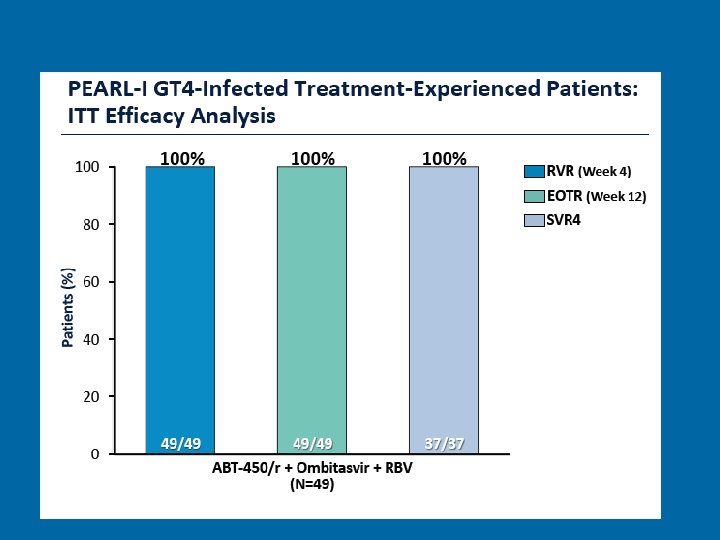
PEARL 1 INTERFERON-FREE REGIMENS OF ABT-450/R + ABT-267 WITH OR WITHOUT RIBAVIRIN In 135 Ch HCV GENOTYPE 4 Patients Treatment-naive and Peginterferon/RBVexperienced patients with chronic HCV GT 4 infection were enrolled. Treatment-naive patients received ABT-450/r (150/100 mg QD) + ABT-267 (25 mg QD) ± weight-based RBV for 12 weeks. Experienced patients received the RBV-containing regimen for 12 weeks. Hezode EASL 2014 Ab 58
Current and future regimens containing the new DAAs for genotype 4 patients Phase III Naive Experienced Phase IIb Experienced Naive 100 SVR (%) 100 Experienced No data for DCV/PR 27/28 SOF/PR 1 NEUTRINO 11/14 10/17 SOF/RBV 2 12 wk 1. Lawitz et al. DDW 2013. 2. Ruane et al. EAS L 2014. Poster 1242. 3. Moreno et al. EASL 2014. Poster 1319. 4. Hézode et al. EASL 2014. 4. Hézode et al. AASLD 2012. Poster 755. 14/14 13/15 SOF/RBV 2 24 wk 29/35 41/72 SMV/PR*3 RESTORE 42/42 37/37 ABT-450/r + Ombitasvir +RBV*4 PEARL-I (SVR 4 only in experienced) 12/12 DCV 60 mg/PR*5 COMMAND-1
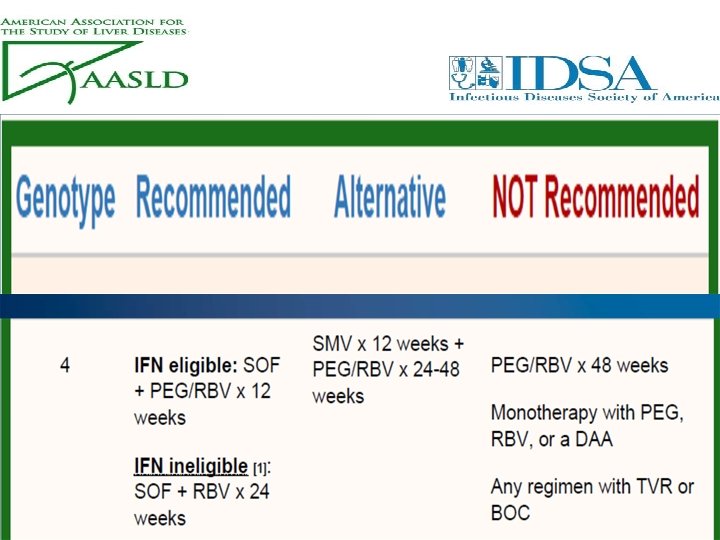
EASL Guidelines: Treatment of HCV GT 4 infection Treatment Options Recommendation status: Regimen Comments by authors Option 1 B 1: PR + SOF 12 wks „appears the most efficacious and the easiest to use “ Evaluated in TN Neutrino SVR 96% 27/28 No data in TE Option 2 B 1: PR+ SMV 12 wks + additional PR for either 12 or 36 wks TN: SVR 89% 31/35 Prior Relapsers: SVR 86% 19/22 Non Responders 57% 41/72 (12 wks SMV + PR; 24 wks total duration for TN & relapsers including cirrhosis and 48 wks for Prior partials and nulls including those with cirrhosis) Option 3 B 1: PR + DAC 60 mg 24 wks B 2: 12 wks TT + additional PR for either 12 or 36 wks: (24 wks total duration for TN & relapsers including Theoretically effective, few data available SVR 100% in 12/12 COMMAND 1 trial cirrhosis and 48 wks for Prior partials and nulls including those with cirrhosis) C 2: R + SOF 24 wks „only preliminary data is available in Egyptian pts“ TN 12 wks treatment: SVR 79% 11/14 TN 24 wks treatment: SVR 100% 14/14 TE 12 wks treatment: SVR 59% 10/17 TE 24 wks treatment: SVR 93% 14/15 Option 5 B 2: SOF+SMV 12 wks „no data with this combination- it is likely that data from Cosmos can be extrapolated“ Option 6 B 2: SOF +DAC (60 mg) 12 wks TN or 24 wks TE Option 4 IFN intolerant or ineligible Consider adding RBV in patients with predictors of poor response or in pts with cirrhosis Consider adding RBV in patients with predictors of poor „no data with this combination- it is likely that data can be extrapolated“
COST EFFECTIVENESS CHART SVR % 100% 120, 000 L. E 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% COST/PT P/R 48 12, 000 L. E P/R/SOF 12 WK 9600 L. E *NAÏVE, NON CIRRHOTIC, LOW VIREMIA, R/SOF 24 WK 12, 600 L. E *R/SOF 12 WK 6600 L. E
Eradication of HCV in Egypt Overcoming the Barriers
Annual mortality assumed at: 50/100, 000 Or 5/1000 for HCV positive patients
Annual mortality assumed at: 50/100, 000 Or 5/1000 for HCV positive patients
Overcome the Barriers • Ideal drug • Decrease incidence • Mass treatment
Ideal Drug It is important for patients treatment but more important for control and eradication of any infectious disease
Decrease incidence • Blood safety. • Avoid unneeded injection. • Auto destructive syringes. • Infection control. • Media awareness. • Case detection and treatment by Ideal drug
HCV in EGYPT from Control to Eradication To decrease HCV prevalence to< 2 % in Egypt in 10 years(Mathematical modeling) Effective treatment SVR > 90% Annual treatment of 250. 000 to 300. 000 patients Decrease incidence by prioritize treatment to most frequent injectors J. viral hepatitis, 2014
HCV Treatment guidelines (Draft)
• Priority for treatment will be directed towards patients with F 3 and F 4. • No differentiation in treatment priority will be established based on the previous treatment experience.
• Assessment of fibrosis stage will be performed by using a combination of both Fibroscan results and FIB 4 score. F 3 -4 stage will be considered if both Fibroscan result is more than 9. 5 and FIB 4 score is more than 1. 45. If both results are below these cut-off values, patient will not be assigned as a treatment priority. If one of these two methods is above the cut-off value while the other is below, performing liver biopsy or re-assessment after one year is recommended to rule out the fibrosis stage of the patient.
• Upper GI endoscopy is mandatory in the following circumstances: a. Histological evidence of cirrhosis by liver biopsy b. Fibroscan > 19. 2 K. Pa c. Platelet count < 100, 000
• Patients who are eligible to receive Interferon (according to the currently used inclusion/exclusion criteria for combined IFN/RBV treatment)will be treated with daily Sofosbuvir (400 mg) and weight-based RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) plus weekly PEG for 12 weeks. • Recommended regimen for patients who are not eligible to receive IFN is daily Sofosbuvir (400 mg) plus weight-based RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]) for 24 weeks
• Inclusion criteria for treatment will be expanded to adapt for more advanced liver fibrosis patients (who will be treated with Interferon free regimen) as defined with the presence of one or more of the following; – Child score up to 8 – Total bilirubin ≤ 3 – Albumin ≥ 2. 5 – Platelet count ≥ 50, 000 – Prtothrombin concentration ≥ 50% – Hemoglobin concentration ≥ 10 mg • Otherwise, waiting for new DAAs combination is advised.
• Patients with more decompensated liver disease will be excluded from treatment until enough data will be available and this will be applied to: – Child C patients with scores ≥ 9 – Presence of ascites (except after control) – Patients with HCC except after successful radical curative intervention (4 months after resection or successful local ablation) evident by triphasic CT. – Presence of large risky esophageal varices (except after prophylactic management)
• Age limits for treatment legibility will be above 18 years and below 70 years for all patients while BMI will be accepted up to 35. • The same rules will be applied for all patients regardless the source of payment and there will be no role for patients' preferences in deciding the treatment regimen.
• For special population groups; priority for treatment will be offered for post liver transplantation, post kidney transplantation patients and combined HCV/HBV infection regardless the fibrosis stage • . Other groups like Pediatric age group and kidney disease patients will be kept for discussion after the availability of enough data.
• Patients with documented extra-hepatic manifestations will be prioritized for treatment according to the same guidelines. • Treatment experienced patients should not start evaluation for new treatment regimens except after 6 months from cessation of interferon therapy.
Ga ma l Es ma t