Neonatal Sepsis Definition n Clinical syndrome of systemic


: – Culture proven infection within the first 3")


: – Group B Streptococcus (GBS) – E.")
: – Staphylococcus aureus – Gram negative bacilli")


 Not doing well")







 CNS Manifestations:")
 urine, saliva, blood, CSF for CMV-specific Ig. M 2)PCR 3)CBC - anemia,")







 – Carbapenem (meropenem) – +")

- Slides: 30
Neonatal Sepsis
Definition n Clinical syndrome of systemic illness accompanied by bacteremia occurring in the first month of life n Mortality rate is high – Higher rates in premature infants – Neonatal sepsis is a common cause of morbidity and mortality
Types • Early Onset Sepsis (EOS): – Culture proven infection within the first 3 -7 days of life • Late Onset Sepsis (LOS): – Culture proven infection after 7 days of life – UTI, pneumonia, meningitis, osteomyelitis, NEC
Early Onset n First 3 -7 days of life n Usually multisystem fulminant illness with prominent respiratory symptoms (probably due to aspiration of infected amniotic fluid) n High mortality rate n Typically acquired during intrapartum period from maternal genital tract – Associated with maternal chorioamnionitis
Late Onset n occur after the first week of life n Usually have an identifiable focus – Most often meningitis or sepsis – Nosocomial or focal infection
Etiology: EOS • Early Onset Sepsis (EOS): – Group B Streptococcus (GBS) – E. Coli – Listeria monocytogenes (gram +ve) • Due to maternal or perinatal factors
Etiology: LOS • Late Onset Sepsis (LOS): – Staphylococcus aureus – Gram negative bacilli ie. Klebsiella – pseudomonas • Nosocomial or focal infection
Risk Factors • • Prematurity Low birthweight PROM > 18 hours Maternal peripartum fever or infection Resuscitation at birth Multiple gestation Male sex Invasive procedures
Causes of increased incidence of infection in neonates • • • Poor antibody response Poor neutrophil response Poor complement activation Impaired macrophage activity Poor T cell function Reduced placental Ig. G
Clinical Manifestation • • • poor suckling Feeding intolerance Lethargy(poor activity) Not doing well Hypo/hyperthermia Vomiting, Abdominal distention Apnea, RD Seizures Clinical signs and symptoms are nonspecific
Differential Diagnosis 1 - RDS 2 - Metabolic disease 3 - Hematologic disease 4 - CNS disease 5 - Cardiac disease
Investigation 1 - blood culture 2 - CBC with differential White blood cell count and differential – Neutropenia can be an ominous sign Platelet count – Late sign Acute phase reactants – CRP rises early, monitor serial values Other tests: bilirubin, glucose, sodium
3 - Urine cultures 4 - Lumbar puncture 5 - Tracheal aspirates
Radiology 1 - Chest X ray – Obtain in infants with respiratory symptoms – Difficult to distinguish GBS or Listeria pneumonia from uncomplicated RDS 2 - Renal ultrasound in infants with accompanying UTI
Treatment Empiric Antibiotic Therapy • EOS – Ampicillin and Gentamicin • LOS – Vancomycin and Gentamicin • Duration Uncomplicated sepsis Meningitis 10 -14 days 21 days
Supportive therapy n Respiratory n. Oxygen and ventilation as necessary n Cardiovascular n. Support blood pressure with volume expanders n Hematologic n. Treat DIC with FFP n CNS n. Treat seizures with phenobarbital n Metabolic n. Treat hypoglycemia/hyperglycemia and metabolic acidosis
Congenital Infections
Cytomegalovirus 90% of infants with congenital CMV infection are clinically silent 1) CNS Manifestations: • microcephaly , intellectual impairment • sensorineural hearing loss , seizures 2) Reticuloendothelial : • hepatomegaly/splenomegaly • jaundice , hepatitis • thrombocytopenia (with petechiae and purpura) 3) Others : low birth weight (< 2500 gm) pneumonitis , chorioretinitis
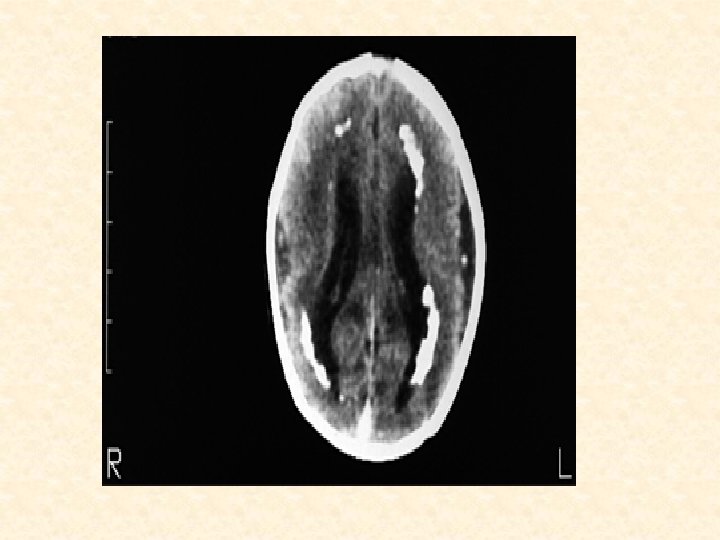
Investigation 1) urine, saliva, blood, CSF for CMV-specific Ig. M 2)PCR 3)CBC - anemia, thrombocytopenia 4)conjugated , unconjugated hyperbilirubinemia 5)elevated hepatic transaminases 6) CSF -- elevated protein content 7) Imaging Studies: CT (Head) - periventricular calcifications Treatment ganciclovir
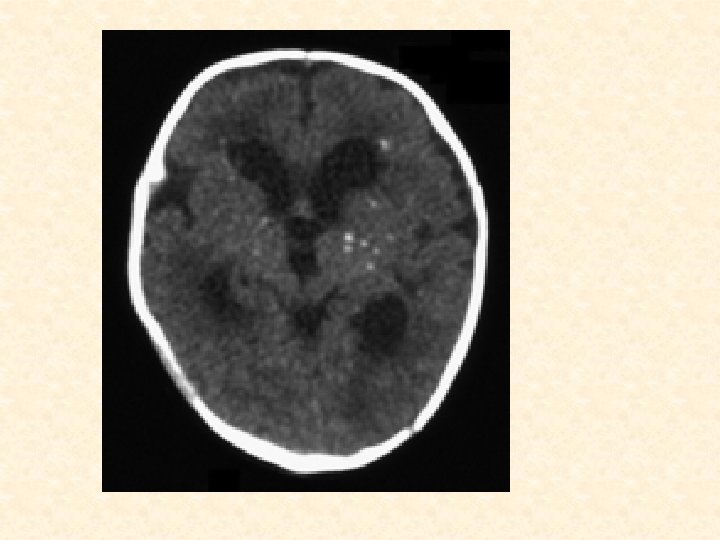
CONGENITAL TOXOPLASMOSIS • Caused by : Toxoplasma gondii Routes of Transmission : Primary Maternal Infection Acquired by: the ingestion of raw meat or contact with cats CLINICAL FEATURES: 70% of infants are asymptomatic • Ocular Manifestations • Chorioretinitis, microphthalmias • optic nerve atrophy, blindness • CNS Manifestations • Hydrocephalus, motor and intellectual retardation • seizures , sensorineuronal hearing loss • classic triad of congenital toxoplasmosis : chorioretinitis, hydrocephalus, and intracranial calcifications.
Investigation • Isolation of T. gondii from placenta or cord blood • Serology • measures Ig. G T. gondii antibody • Ig. M antibody test • Imaging Studies • CT (Head) – intracranial calcifications(scattered through the brain tissue)
CONGENITAL RUBELLA caused by an RNA virus , Vaccine-preventable disease Routes of Transmission: Antenatal (in utero): 1 st trimester 90% 2 nd trimester - 40% 3 rd trimester - 25% • CLINICAL FEATURES: • IUGR - prematurity • Cataracts • microcephaly • Hepatomegaly, splenomegaly • jaundice • patent ductus arteriosus • thrombocytopenia purpura • INVESTIGATIONS: • Serology: fetal rubella-specific Ig. M
Congenital Rubella: skin Lesions: Blueberry muffin rash but may be present in cytomegalovirus
Neonatal meningitis Clinical Picture: • The clinical presentation of neonatal meningitis often is indistinguishable from that of neonatal sepsis without meningitis. • The commonest C/P are temperature instability , irritability, and poor feeding or vomiting • Respiratory distress (tachypnea, retractions , grunting, apnea) • seizures
• Causitive micro-organism: GBS and Escherichia coli are the two most common organisms • investigation 1 - LP • Isolation of a bacterial pathogen from CSF by culture or visualization by Gram stain • Increased CSF white blood cell (WBC) count (typically >1000 WBC/micro. L, but may be lower, especially with gram-positive organisms), with a predominance of neutrophils
2 - blood culture 3 - Cranial US – Safe, convenient, available at the bedside – Ventricular size, development of hydrocephalus – Not identify infarct, abscess, subdural empyema 4 - CT – Abscess, subdural collections, hydrocephalus
Treatment • Gram negative – 3 rd generation cephalosporin(cefotaxime) – Carbapenem (meropenem) – + aminoglycoside • Klebsiella – Carbapenem (meropenem or imepenem)+ aminoglycoside • GBS – Ampicillin + gentamicin • S aureus – Ampicillin, nafcillin or vancomycin + aminoglycoside • Duration of therapy: 21 days(3 weeks)
Thank you