Sepsis and the systemic inflammatory response syndrome Definitions



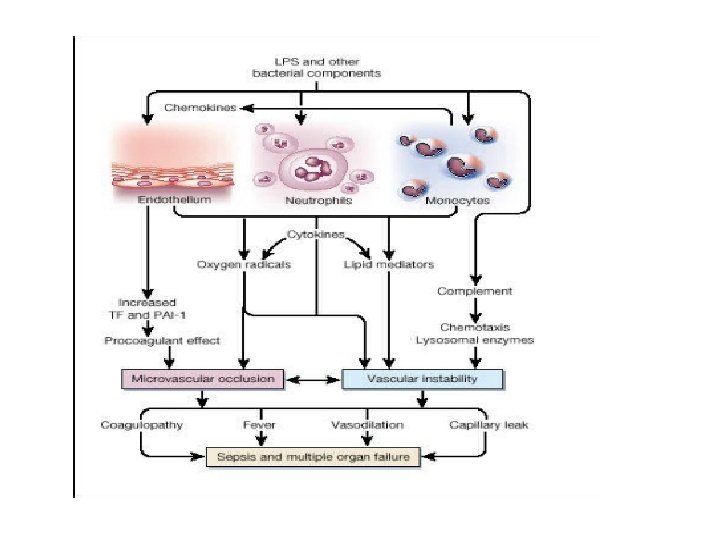
 SIRS refers to the consequences of a dysregulated host")













 • 1 st line therapy")








, abscesses should")





 as first")

 – Tissue hypoperfusion –")
















- Slides: 67
• Sepsis and the systemic inflammatory response syndrome: Definitions, epidemiology, and prognosis • “A little less conversation, a little more action please”
Infection • Infection is characterized by an inflammatory response to microorganisms, or the invasion of normally sterile host tissue by those organisms
Bacteremia • Bacteremia is defined as the presence of viable bacteria in the blood.
Systemic inflammatory response syndrome (SIRS) SIRS refers to the consequences of a dysregulated host inflammatory response. It is clinically recognized by the presence of two or more of the following • Temperature >38. 5ºC or <35ºC • Heart rate >90 beats/min • Respiratory rate >20 breaths/min or Pa. CO 2 <32 mm. Hg • WBC >12, 000 cells/mm 3, <4000 cells/mm 3, or >10 percent immature (band) forms SIRS can result from a variety of conditions, such as autoimmune disorders, pancreatitis, vasculitis, thromboembolism, burns, or surgery.
Definitions
x. Sepsis and Severe Sepsis – SIRS + suspected or confirmed infection (documented via cultures or visualized via physical exam/imaging) Severe Sepsis – Sepsis + at least one sign of organ hypo-perfusion or dysfunction Areas of mottled skin Disseminated intravascular coagulation Capillary refill > 3 secs AKI UOP < 0. 5 cc/kg /hr ARDS or acute lung injury (ALI) Lactate > 2 mmol /L Cardiac dysfunction on echo Altered mental status Plt < 100 000 Abnormal EEG Troponin Leak
x
Comparable Global Epidemiology • 95 cases per 100, 000 – 2 week surveillance – 206 French ICUs • 95 cases per 100, 000 – 3 month survey – 23 Australian/New Zealand ICUs • 51 cases per 100, 000 – England, Wales and Northern Ireland.
Comparison With Other Major Diseases Mortality of Severe Sepsis Cases/100, 000 Incidence of Severe Sepsis AIDS* Colon Breast CHF† Severe Cancer§ Sepsis‡ †National AIDS* Breast AMI† Cancer§ Severe Sepsis‡ Center for Health Statistics, 2001. §American Cancer Society, 2001. *American Heart Association. 2000. ‡Angus DC et al. Crit Care Med. 2001; 29(7): 1303 -1310
Emergency Department Critical Care Volume Increases • 102 million National ED visits in 1999 • 17% (17. 5 million) “immediately life threatening” 1 • 57 California Emergency Departments (1990 -1999)2 • 50% (387, 616) Severe Sepsis Cases Initially Present ED P < 0. 001 for all groups 1. 2. 3. National Center for Health Statistics; 2001 Ann Emerg Med 2002; 39: 389 -96 Curr Opin Crit Care Dec. 2002
Population characteristics • The population at risk of developing sepsis is large. At any given moment, approximately 50 percent of ICU patients have a nosocomial infection Important risk factors include: • Bacteremia. • Advanced age (≥ 65 years). • Impaired immune system function. Comorbidities that cause hostdefense depression (neoplasms, renal or hepatic failure, AIDS) are common in septic patients. • Community acquired pneumonia (CAP). Among patients with CAP, severe sepsis and septic shock will either develop or be present at admission in approximately 48 and 5 percent of patients, respectively
The most common manifestations of severe organ dysfunction were • acute respiratory distress syndrome, • acute renal failure, • disseminated intravascular coagulation Survival was reduced in patients with these complications
CHARACTERISTICS THAT INFLUENCE OUTCOME Clinical characteristics that relate to the severity of sepsis include an abnormal host response to infection the site and type of infection the timing and type of antimicrobial therapy and the development of shock
Prognostic effects of organ dysfunction in severe sepsis
Prevalence of hospital mortality associated with severe sepsis
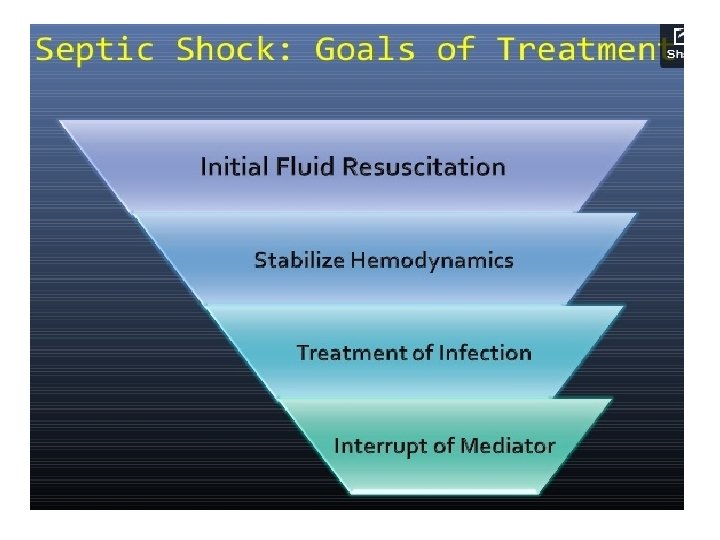
6 Hour Resuscitation Bundle • Early Identification • Early Antibiotics and Cultures • Early Goal Directed Therapy
6 - hour Severe Sepsis/Septic Shock Bundle • Early Detection: – Obtain serum lactate level. • Early Blood Cx/Antibiotics: – within 3 hours of presentation. • Early EGDT: • Hypotension: (SBP < 90, MAP < 65) or lactate > 4 mmol/L: initial fluid bolus 20 -40 ml of crystalloid (or colloid equivalent) per kg of body weight. • Vasopressors: – Hypotension not responding to fluid – Titrate to MAP > 65 mm. Hg. • Septic shock or lactate > 4 mmol/L: – CVP and Scv. O 2 measured. – CVP maintained >8 mm. Hg. – MAP maintain > 65 mm. Hg. • Scv. O 2<70%with CVP > 8 mm. Hg, MAP > 65 mm. Hg: – PRBCs if hematocrit < 30%. – Inotropes.
Fluid therapy • Central Line Access (Fluid hydration +/pressor) • 1 st line therapy – fluids, fluids! • Crystalloid equivalent to colloid • Initial 1 -2 Liters (20 mg /kg) crystalloid or 500 ml colloid • Careful in CHF patients !!
Fluid Challenge What is the difference between an infusion and a challenge? 250 to 500 ml colloid (or blood products) 500 to 1000 ml Hartmann’s [NOT 5% dextrose] As fast a possible (with pressure bag) You at the bedside
x. Surviving Sepsis targets of fluid resuscitation What are they? • • SBP > 90 MAP > 65 CVP 8 - 12 U/o > 0. 5 ml/kg/hr Lactate < 1 Scv. O 2 >70 HCt > 30
Markers of perfusion What are they? • Clinical signs – Warm skin, conscious level, u/o • Haemodynamic variables – CVP • Bloods – Serum Lactate – Scv. O 2 Tissue perfusion should be promptly restored using intravenous fluids, vasopressors, red blood cell transfusions, and inotropes However, critical hypoperfusion can also occur in the absence of hypotension, especially during early sepsis
if Pseudomonas is an unlikely pathogen, we favor combining vancomycin with one of the following: • Cephalosporin, 3 rd or 4 th generation (eg, ceftriaxone or cefotaxime), or • Beta-lactam/beta-lactamase inhibitor (eg, piperacillintazobactam, ticarcillin-clavulanate), or • Carbapenem (eg, imipenem or meropenem).
Alternatively, if Pseudomonas is a possible pathogen, we combine vancomycin with two of the following • Antipseudomonal cephalosporin (eg, ceftazidime, cefepime), or • Antipseudomonal carbapenem (eg, imipenem, meropenem), or • Antipseudomonal beta-lactam/beta-lactamase inhibitor (eg, piperacillin-tazobactam, ticarcillin-clavulanate), or • Fluoroquinolone with good anti-pseudomonal activity (eg, ciprofloxacin), or • Aminoglycoside (eg, gentamicin, amikacin), or • Monobactam (eg, aztreonam)
• For patients whose Scv. O 2 remains <70 percent after intravenous fluid and vasopressor therapy, it is reasonable to administer additional therapies, including blood transfusions or inotropic therapy.
• Prompt identification and treatment of the site of infection are essential. Sputum and urine should be collected for gram stain and culture. Intra-abdominal fluid collections should be percutaneously sampled. Blood should be taken from two distinct venipuncture sites and from indwelling vascular access devices and cultured aerobically and anaerobically.
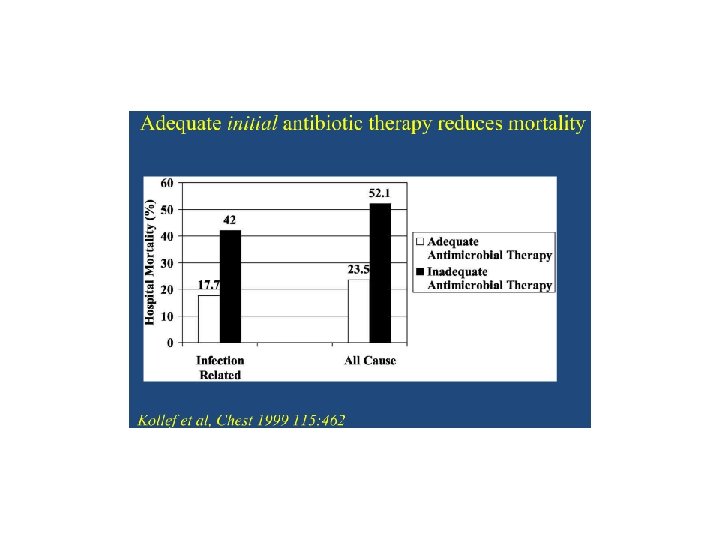
• Antibiotics should be administered immediately after appropriate cultures have been obtained. We recommend empiric broad spectrum antibiotics when a definite source of infection can not be identified (Grade 1 B).
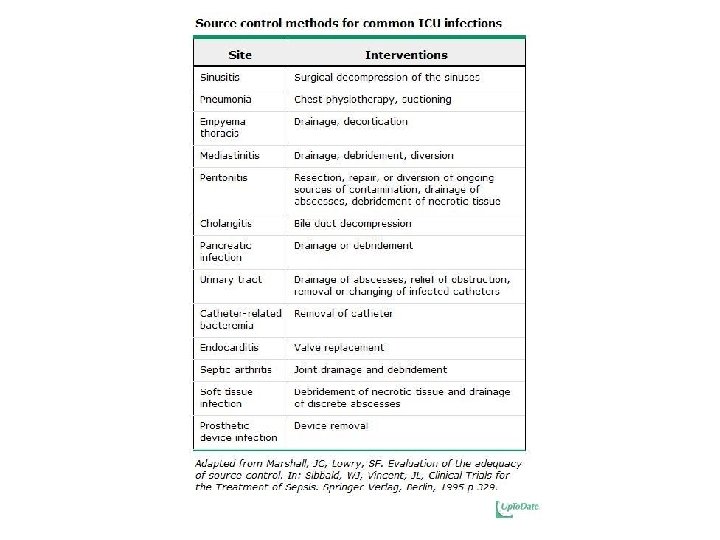
• Potentially infected vascular access devices should be removed (if possible), abscesses should be drained, and extensive soft tissue infections should be debrided or amputated
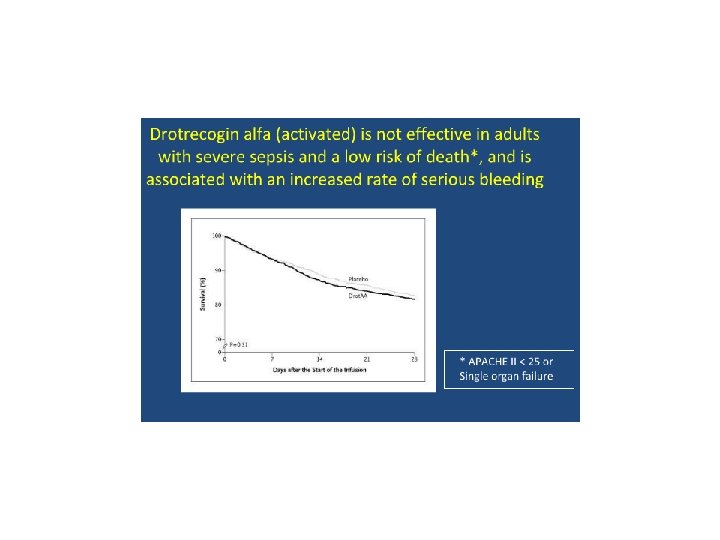
• In patients with septic shock or severe sepsis with a high risk of death, defined as an APACHE II score >25, multiple organ dysfunction, or sepsis-induced acute respiratory distress syndrome, we suggest that recombinant human activated protein C be administered if contraindications do not exist (Grade 2 B). Effort should be made to initiate the infusion within 24 hours from the first-sepsis induced organ dysfunction.
• Glucocorticoid therapy, nutritional support, and glucose control are additional issues that are important in the management of patients with severe sepsis or septic shock. Each is discussed in detail in separate topic reviews.
Rhode Island Hospital EGDT Data Time from Entering ED to Receiving Antibiotics Time from Entering ED to Catheter Insertion Reduced by 42% Reduced by 60% Time from Entering ED to Transfer to MICU Reduced by 51%
24 - hour Severe Sepsis and Septic Shock Bundle • • Glucose control: – maintained on average <150 mg/d. L (8. 3 mmol/L) Drotrecogin alfa (activated): – administered in accordance with hospital guidelines Steroids: – for septic shock requiring continued use of vasopressors for equal to or greater than 6 hours. Lung protective strategy: – Maintain plateau pressures < 30 cm H 2 O for mechanically ventilated patients
IV Abx within 3 hrs in the ED, within 1 hr in the ICU Broad Spectrum, combination therapy for neutropenic and patients with pseudomonas risk factors Vancomycin PLUS Zosyn Consider need for Source Control ! Drainage of abscess or cholangitis, removal of infected catheters, debridement or amputation of osteomyelitis
Pressors • See separate lecture on vasopressors – Start with Levophed (norepinephrine) as first line therapy +/- Vasopressin – Consider Dopamine peripherally on floor • ** This is available in crash cart ** If not responding to fluids, don’t want for pharmacy to send levophed.
Corticosteroids • Use in Septic Shock, if NO response to vasopressors and fluids – HYDROCORTISONE 200 mg -300 mg / day Divided doses (Q 6 hrs) • Initial Dose 100 mg IV x 1
Lactate What does it mean? • Increased production (anaerobic glycolysis) – Tissue hypoperfusion – Tissue dysoxia • Reduced metabolism – Hepatic – Renal • <1 is normal, 1 -2 is a concern, >2 is bad, >4 is very bad
Scv. O 2 What does it mean? • Balance between oxygen delivery and consumption (VO 2) • Fick principle • Scv. O 2 = Sa. O 2 - VO 2 CO • Target > 70%
Further Management What else can be done? • • Low tidal volume ventilation Steroids in septic shock Activated Protein C Glycaemic control Stress ulcer prophylaxis Thromboprophylaxis Sedation scoring / holds etc.
System-based Approaches to sepsis Rivers, E. , Nguyen, B. , Havstad, S. , Ressler, J. , Muzzin, A. , Knoblich, B. , Peterson, E. , et al. (2001). Early goal-directed therapy in the treatment of severe sepsis and septic shock. New England Journal of Medicine, 345(19), 1368– 1377.
x. System-based Approaches to sepsis Early-Goal Directed Therapy INCLUSION = SEPSIS AND [BP < 90 after fluid OR Lactate > 4] Control Intervention EGDT CVP 8 -12 Fluids CVP 8 -12 MAP > 65 Vasopressors MAP > 65 Transfusions Dobutamine Scv. O 2 > 70% 49% mortality 33% mortality Rivers, E. , Nguyen, B. , Havstad, S. , Ressler, J. , Muzzin, A. , Knoblich, B. , Peterson, E. , et al. (2001). Early goal-directed therapy in the treatment of severe sepsis and septic shock. New England Journal of Medicine, 345(19), 1368– 1377.
A Multidisciplinary Community Hospital Program for Early and Rapid Resuscitation of Shock in Nontrauma Patients Sebat, F. , Johnson, D. , Musthafa, A. A. , Watnik, M. , Moore, S. , Henry, K. , & Saari, M. (2005). A multidisciplinary community hospital program for early and rapid resuscitation of shock in nontrauma patients. Chest, 127(5), 1729– 1743.
A Multidisciplinary Community Hospital Program for Early and Rapid Resuscitation of Shock in Nontrauma Patients Sebat, F. , Johnson, D. , Musthafa, A. A. , Watnik, M. , Moore, S. , Henry, K. , & Saari, M. (2005). A multidisciplinary community hospital program for early and rapid resuscitation of shock in nontrauma patients. Chest, 127(5), 1729– 1743.
Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis BEFORE Do whatever it is that you normally do. We will be watching. AFTER All physicians, nurses, and patient care technicians in the emergency department and intensive care units received formal order set clinical education. Additionally, all hospital floor clinical nurse specialists and advance practice nurses, along with the house staff physicians in these areas, were inserviced on the order sets. . These educational endeavors included training in sepsis pathophysiology, monitoring of central venous pressures, assessment of central venous blood oxygen saturation, and the pharmacotherapy of sepsis 1. EDUCATION 2. ORDER SET with recommendations and goals for sepsis treatment. Thiel, S. W. , Asghar, M. F. , Micek, S. T. , Reichley, R. M. , Doherty, J. A. , & Kollef, M. H. (2009). Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis*. Critical Care Medicine, 37(3), 819– 824. doi: 10. 1097/CCM. 0 b 013 e 318196206 b
Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis After Before Thiel, S. W. , Asghar, M. F. , Micek, S. T. , Reichley, R. M. , Doherty, J. A. , & Kollef, M. H. (2009). Hospital-wide impact of a standardized order set for the management of bacteremic severe sepsis*. Critical Care Medicine, 37(3), 819– 824. doi: 10. 1097/CCM. 0 b 013 e 318196206 b
Acute Phase Identify Sepsis as early as possible Broad Spectrum antibiotics ASAP and Identify source(s) of infection Identify severity: Vitals, mental status, UOP, LACTATE, other labs. Volume and physiologic resuscitation ASAP with GOALS. Tweak your system so these things happen FAST
Sepsis Identification Train all providers Vital sign/Laboratory alerting systems ? Biomarkers
Defining the severity of sepsis Importance of looking for organ failure is self evident. Identification of “shock” dramatically alters the treatment and mortality. Blood Pressure, Response to Fluid, LACTATE
Lactate Evidence is clear that Lactate levels are predictive of death and MODS Clearance of lactate is associated with improved survival Algorithms of care based on lactate clearance appear to work as well or better than other approaches. Jones AE, Shapiro NI, Trzeciak S, et al. Lactate Clearance vs Central Venous Oxygen Saturation as Goals of Early Sepsis Therapy: A Randomized Clinical Trial. JAMA: The Journal of the American Medical Association 2010; 303(8): 739– 46. Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, openlabel, randomized controlled trial. American Journal of Respiratory and Critical Care Medicine 2010; 182(6): 752– 61.
Goals in resuscitation Initial fluid resuscitation: CVP 8 -12, MAP > 65, UOP 0. 5 m. L/kg/hr, Sc. VO 2 70% and Lactate Clearance. Give enough volume to maximize stroke volume. Start with 20 cc/kg in most patients. Goal? Give vasopressors to raise the MAP enough to maintain adequate end-organ perfusion. Assessment of Cardiac Function UOP and Lactate Clearance are nice global indicators of success.
Chronic Phase Monitor for and prevent recurrence of sepsis VAP, CLABSI, UTI. Infection Control Practices. Lung Protective Ventilator Strategies Protocolized Sedation, Daily Awakenings Nutritional Support Early Mobilization Success with these measures is most likely with a multi-disciplinary approach.
Evidence-Based Sepsis Guidelines
Evidence-Based Sepsis Guidelines