SEPSIS BIOSURVEILLANCE What is sepsis Sepsis is a

SEPSIS BIO-SURVEILLANCE

What is sepsis? • Sepsis is a complication of severe infection characterized by a systemic inflammatory response. (Gauer, 2013) • Sepsis can be present on admission, or it can occur during hospitalization. • It may result from catheter-acquired infections, central line infections, ventilator-acquired pneumonia, or in any case where a harmful organism invades the body. • Every single patient is at-risk for sepsis.
 and Sepsis • SIRS is a group of signs")
Systemic Inflammatory Response Syndrome (SIRS) and Sepsis • SIRS is a group of signs and symptoms resulting from systemic activation of the immune response to infection or injury. • SIRS is considered to be two or more of the following: • Temperature > 100. 9 F (38. 3 C) or < 96. 8 F (36 C) • Heart Rate > 90 beats/minute • Respiratory Rate > 20 breaths/minute or Pa. CO 2 < 32 mm. Hg • WBC count > 12, 000 or < 4, 000 cells/mc. L • Normal WBC with > 10% Bands on differential • If SIRS goes untreated or undertreated, it may lead to sepsis. • Sepsis is two or more SIRS criteria with a suspected or documented infection. (Schell-Chaple & Lee, 2014)

Severe Sepsis and Septic Shock • Severe sepsis is sepsis plus signs of organ dysfunction or tissue hypoperfusion: • Hypotension (SB <90 mm. Hg or decrease of 40 mm. Hg from baseline; • • • MAP < 70 mm. Hg Blood lactate level > 2 mmol/L Altered mental status. Hypoxemia (Sp 02 < 90% or Pa. O 2/Fi. O 2 ratio < 250) Low urine output (<0/5 m. L/kg/hr) Coagulopathy (platelets < 100, 000/mc. L; INR > 1. 5) Bilirubin level > 2 mg/d. L (Schell-Chaple & Lee, 2014) • When the patient is hypotensive, or has a lactate > 4, they are considered to be in septic shock.

. Sepsis Statistics • Sepsis is the leading cause of death in ICUs, with an overall mortality of 1 in 4 patients. (Kurczewski, et al. , 2015) • Mortality rates for patients in septic shock range between 40% to 70%. (Gauer, 2013) • Sepsis affects more than 750, 000 persons annually, with a prevalence of 3 cases per 1, 000 persons. (Gauer, 2013) • Sepsis is one of the leading causes of hospital admission and death worldwide. (Gray, et al. , 2013) • Sepsis costs the health care system $17 billion every year. (Kurczweski, et al. , 2015)

. time goes by without appropriate intervention. • The chances of surviving sepsis dramatically decrease as

What can we do? • Early goal directed therapy remains the standard of care for patients identified as septic. • Anticipate and advocate for orders that include a blood lactate level, blood cultures, and diagnostic testing. • Septic patients should receive broad spectrum antibiotics within 1 hour of recognition. • For hypotension or a lactate > 4 mmol/L, administer 30 m. L/kg fluid bolus. (Schell-Chaple & Lee, 2014) • In order to improve survival, early recognition and management of sepsis is necessary. • Patients cannot be treated for sepsis until they are identified as septic!

What can we do? • Despite improving outcomes in healthcare, mortality related to sepsis remains high. (Gray, et al. , 2013) • Sepsis can be difficult to identify but easy to treat in its early stages. • Sepsis is then easy to identify but difficult to treat in its late stages. (Davis, 2015) • Early identification of sepsis is necessary for adequate treatment.

Respiratory Assessment • The earliest clinical sign of sepsis is often a rapid respiratory rate. (Nimmo, et al. , 2006) • Patients should be assessed carefully for even slight changes in oxygenation, as oxygenation changes are among the earliest signs of deterioration. • The respiratory rate rises as the body tries to compensate for decreased tissue oxygenation. • Pulse oximetry values decline. • The patient may need higher levels of administered oxygen to maintain adequate oxygen saturation. • Slight changes in the respiratory assessment should cause the nurse to suspect early SIRS/Sepsis. (Bernstein, et al. , 2013)

Electronic Sepsis Alerts • Using electronic sepsis alerts may minimize delays in recognizing sepsis. (Alsolamy, et al. , 2014) • One study found that 68% of patients with a positive electronic alert had a human delay in recognition and treatment. (Harrison, et al. , 2015 ) • Septic patients were compared prior to and after an electronic alert implementation. The post-alert group had a shorter time to sepsis intervention by a median of 3. 5 hours. (Kurczweski, et al. , 2015)

Electronic Sepsis Alerts • Using an electronic sepsis alert may help identify septic patients sooner. • Once identified, early goal directed therapy can be initiated. • The sooner patients are treated for sepsis, the greater their chances of survival. • Utilizing electronic sepsis alerts may help decrease mortality related to sepsis.

Cerner Biosurveillance Tool • Mercy General Hospital will be implementing an electronic sepsis alert in August 2015 • Goals of the Cerner Biosurveillance tool: • Save lives! Decrease mortality rates related to sepsis. • Decrease ICU length of stay • Prevent ICU admissions • Decrease costs associated with sepsis and its complications.

How does it work? • The tool in Cerner will run automatically every 10 minutes on every Inpatient, Observation, and ED patient age 16 and over. • When a patient screens positive for SIRS or Sepsis, an alert will fire to the primary nurse for the patient. • This alert will provide the nurse with the specific criteria that caused the trigger. • This alert will notify the nurse regardless of which patient’s chart the nurse is logged into. • Nursing will receive alerts for SIRS and Sepsis. • Providers will receive limited Sepsis alerts.

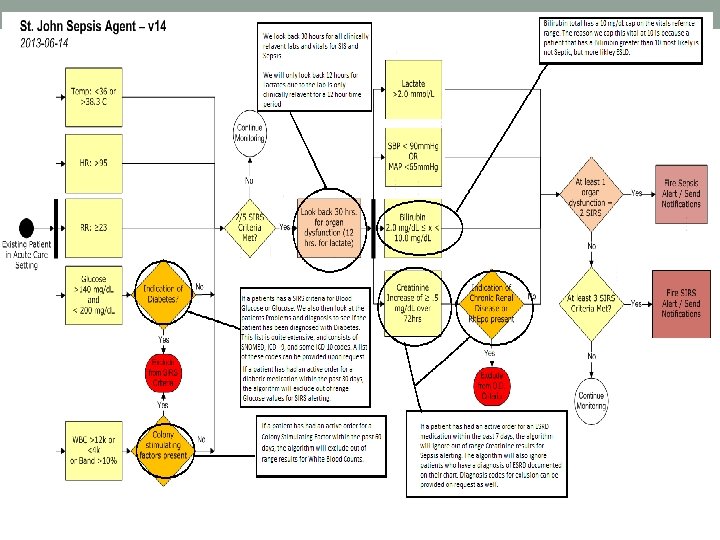
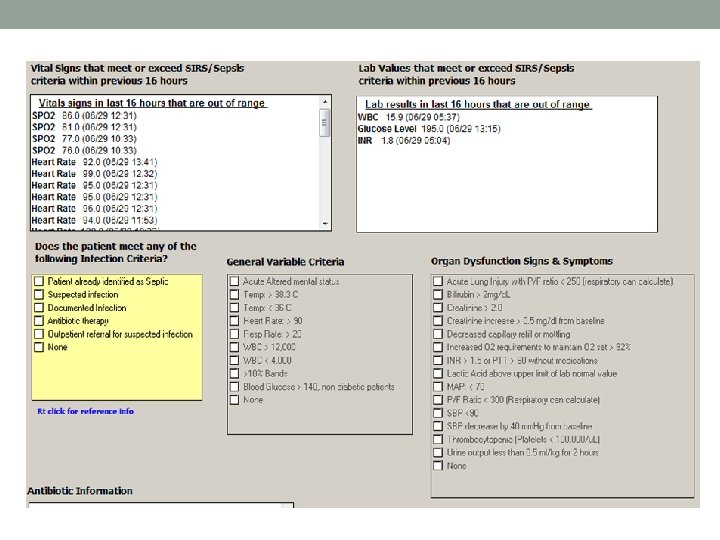
How does it work? • The SIRS alert will fire with 3 signs of SIRS: • Temp <36 or >38. 3 C • HR >95 • RR > 23 • Glucose > 140 mg/d. L and < 200 mg/d. L (without indication of diabetes) • WBC >12 k or <4 k or Band >10% • The Sepsis alert will fire with 2 SIRS criteria and 1 sign of organ dysfunction: • Lactate >2. 0 mmol/L • SBP <90 mm. Hg or MAP <65 mm. Hg • Bilirubin 2. 0 mg/d. L < x < 10. 0 mg/d. L • Creatinine increase of >. 5 mg/d. L over 72 hours
 will")
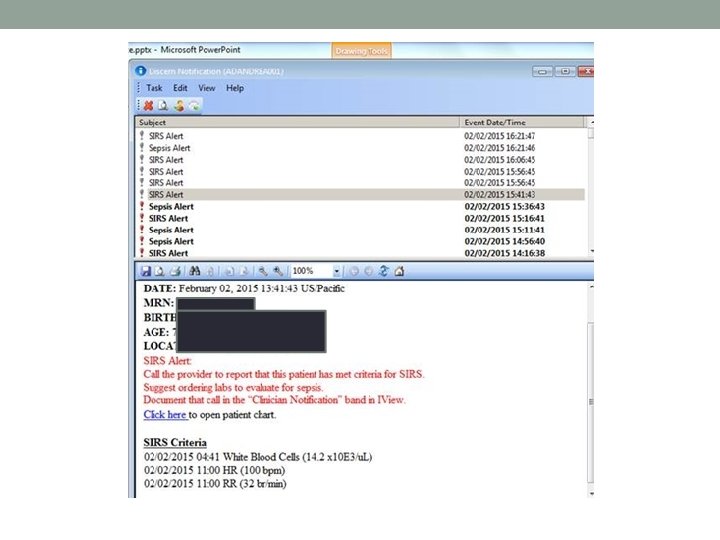
How does it work? • A Discern Alert (shown on the next slide) will fire to the primary nurse regardless of where they are currently in Cerner. If not in the patient’s chart, this alert will provide a hyperlink to open positive patient’s chart.

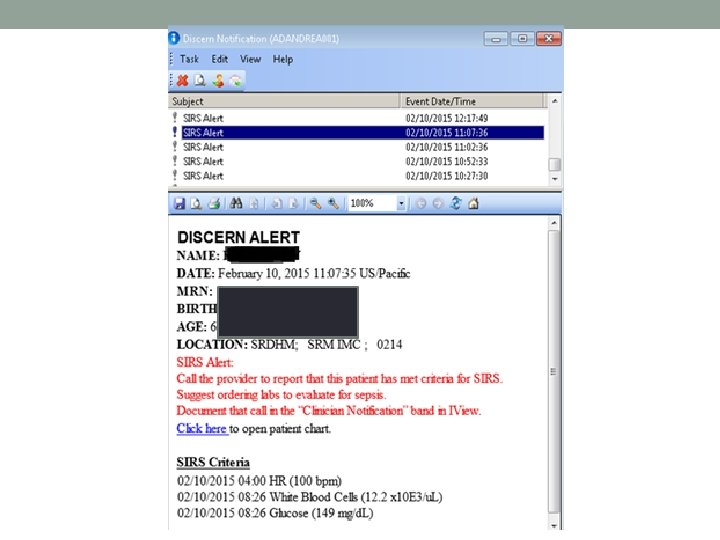
How does it work? • If the nurse is currently logged into the patient’s chart when the alert fires, they will receive the alert (shown on next slide) with an option for Clinician Notification.

Clinician Notification • Clicking “OK” does not provide a nurse response time, and will not stop the alert from firing. • Clicking “OK” on the alert will allow the nurse to review what triggered the alert. • Clicking on Clinician Notified will open the Clinician Notification Ad hoc form. • Documenting Clinician Notification from the alert box, Ad hoc, or the IView flowsheet will cease the alert for nurses.

Clinician Notification

New Flowsheet Tab

Sepsis Dashboard • The biosurveillance tool has a dashboard for leadership. • It allows you to compare facilities by metrics such as: • Length of Stay • Mortality Rate • Provider Response Time • Nurse Communication (Time from alert to provider notified) • Allows you to drill down by unit, as well as specific providers and nurses. • This allows for opportunities to educate specific providers and nurses on an individual basis.

Brief Snapshot of Live Data Tracking

Ability to select individual unit and users:

Nurse Response • The primary nurse who receives the SIRS/Sepsis alert is required to notify the patient’s provider as early as possible. This should be done no later than 120 minutes of the first alert. • Giving antibiotics within 1 hour of recognition is key in appropriate sepsis treatment, so the sooner the physician is notified, the more likely this treatment goal will be reached. • The alert will provide a Clinician Notify box which opens an Ad hoc form for the nurse to document what time the provider was notified.

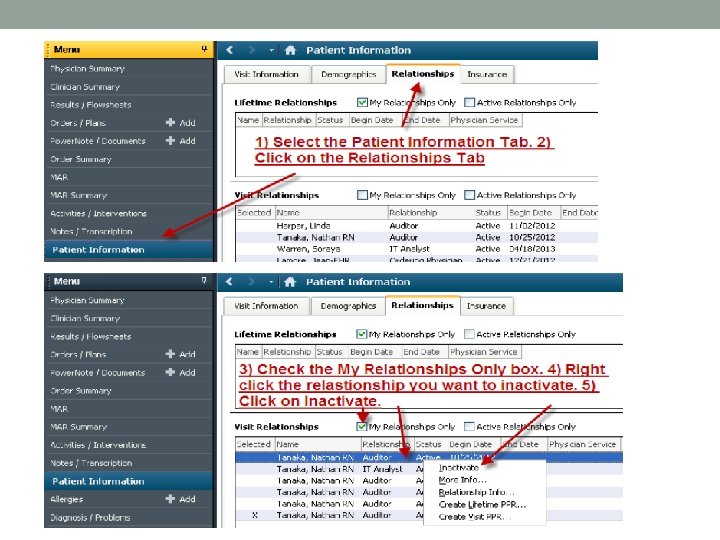
Inactivate Relationship • Mercy San Juan implemented this alert and found that primary nurses who were no longer caring for the patient were receiving the alert for the patient. • In order to prevent this from happening at MGH, after the nurse is finished caring for a patient, they must inactivate their relationship. • This is done under the Patient Information tab in Cerner.

Physical Assessment • This alert is being implemented in addition to nurses’ ongoing physical assessments. This alert in no way replaces the nurses’ responsibility to provide adequate and thorough assessment of their patients. • Please do not depend on this tool to assess signs of SIRS and sepsis for you. It is intended to help identify these signs earlier in the event you are in another patient’s chart and have not had time to review recent laboratory results. • Anticipate further sepsis education to help you in identifying and treating sepsis in its earliest stages.

Alert Fatigue • Repeated exposure to electronic alerts leads to declining user responsiveness over time. (Embi & Leonard, 2011) • Be aware of alert fatigue and always take the SIRS and Sepsis alerts seriously. • The tool has been tested and currently shows high specificity and sensitivity, so false positives should be minimal. • Being mindful of BMDI vital signs prior to signing them off will help reduce false positive alerts.

Additional Information • Nurses are expected to continue their current process, as seen on the next slide. • Shift screenings and sepsis screenings should continue to be done on every patient. • Nurses should only call RRT for signs of organ dysfunction. A positive SIRS alert does not necessitate a call to RRT.

Sources • Alsolamy, S. , Al Salamah, M. , Al Thagafi, M. , Al-Dorzi, H. M. , Marini, A. M. , • • • Aljerian, N. , & …. Arabi, Y. M. (2014). Diagnostic accuracy of a screening electronic alert tool for severe sepsis and septic shock in the emergency department. BMC Medical Informatics & Decision Making, 14(1), 1 -13. doi: 10. 1186/s 12911 -014 -0105 -7 Bernstein, M. , & Lynn, S. (2013). Helping patients survive sepsis. American Nurse Today. (8)1. Davis, C. (2015). Sepsis. What is the prognosis? Medicine. Net. Retrieved on June 6, 2015, from http: //www. medicinenet. com/sepsis/page 7. htm Embi, P. J. , & Leonard, A. C. (2012). Evaluating alert fatigue over time to EHRbased clinical trial alerts: findings from a randomized controlled study. Journal Of The American Medical Informatics Association: JAMIA, 19(e 1), e 145 -e 148. Gauer, R. L. (2013). Early recognition and management of sepsis in adults: the first six hours. American Family Physician, 88(1), 44 -53 Gray, A. , Ward, K. , Lees, F. , Dewar, C. , Dickie, S. , & Mc. Guffie, C. (2013) The epidemiology of adults with severe sepsis and septic shock in Scottish emergency departments. Emergency Medicine Journal, 30(5), 397 -401. doi: 10. 1136/emermed-2012 -201361

Sources • Harrison, A. M. , Thongprayoon, C. , Kashyap, R. , Chute, C. G. , Gajic, O. , • • Pickering, B. W. , & Herasevich, V. (2015). Developing the surveillance algorithm for detection of failure to recognize and treat severe sepsis. Mayo Clinic Proceedings, 90(2), 166 -175. doi: 10. 1016/j. mayocp. 2014. 11. 014 Kumar, A. , et al. (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Critical Care Medicine, 34(6), 1589 -96. Kurczewski, L. , Sweet, M. , Mc. Knight, R. , & Halbritter, K. (2015). Reduction in time to first action as a result of electronic alerts for early sepsis recognition. Critical Care Nursing Quarterly, 38(2), 182 -187. doi: 10. 1097/CNQ. 000000060 Nimmo, G. , Nelson, G. , & Cairns, C. (2006). Identifying sepsis early. University of Edinburgh. 6 Schell-Chaple, H. , & Lee, M. (2014). Reducing sepsis deaths: a systems approach to early detection and management. American Nurse Today, 9(7), 26 -31.


Changes to the Severe Sepsis Bundle beginning October 1 st • Inclusions: Inpatients age 18 and older and ICD-10 -CM Principle or Other Diagnosis Code of severe sepsis or septic shock • Exclusions: Directive for Comfort Care within 3 hrs of severe sepsis LOS > 120 days Directive for Comfort Care within 3 hrs of septic shock Transfer from another acute care facility Administrative contraindication to care Patients with severe sepsis who expire within 3 hours of presentation Patients with septic shock who expire within 6 hours of presentation

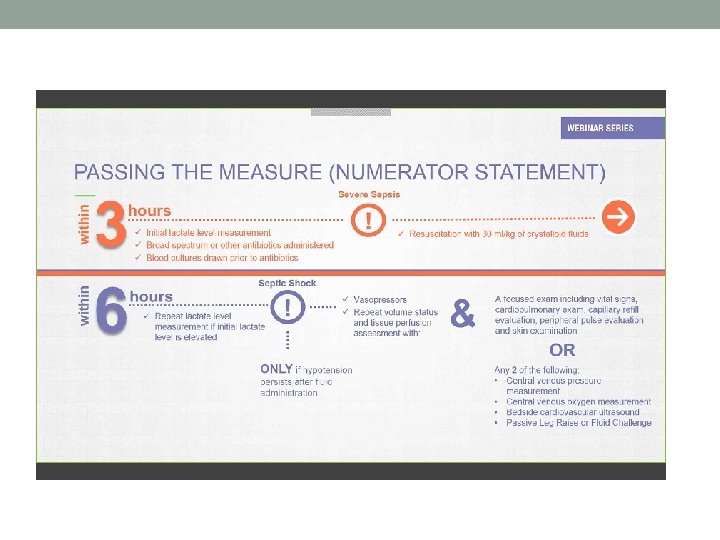
Changes to the definition of Time Zero • Time zero will always be when the chart annotation suggests signs and symptoms are all present. • Time Zero may be from nursing charting, lab flow sheets, physician documentation, anything with a time stamp • Time Zero will be triage time if all signs and symptoms are present at triage Two Clocks • Severe Sepsis: Three Hour and Six Hour Counters • Septic Shock: Three Hour and Six Hour Counters • Clinical Example follows: o A patient developed severe sepsis at 12 pm but did not become hypotensive until 5 pm. o The severe sepsis bundle time would start at 12 pm and the shock bundle time would start at 5 pm. Severe Sepsis Bundle (without shock) Severe Sepsis Three Hour Bundle • Initial lactate level measurement • Blood Cultures prior to antibiotics • Antibiotic administration Severe Sepsis Six Hour Bundle • Repeat lactate if initial lactate is greater than

Septic Shock Bundle Septic Shock Three Hour Clock • Fluid resuscitation with 30 ml/kg of crystalloid fluids (Normal Saline or Lactated Ringers). Resuscitation must be completed within three hours. Septic Shock Six Hour Clock • Vasopressor administration • Document Reassessment of volume status and tissue perfusion with Either: Ø Repeat focused exam (after initial fluid resuscitation). All elements must be documented by a Licensed Independent Practitioner: o Complete set of vital signs: (temperature, pulse, RR and BP) to be taken at one point in time; must be documented by the physician. o Cardio-pulmonary exam: must incorporate both heart and lung assessment and assessed within the same timeframe. o Capillary Refill: must be within same timeframe, provider must complete assessment and document findings. Cannot be pulled into the note (Cerner) from nursing documentation o Peripheral pulse exam: provider must complete assessment and document findings. Cannot be pulled into the note (Cerner) from nursing documentation. Can include radial, dorsalis pedis and posterior tib. o Skin exam: provider must complete assessment and document findings. Cannot be pulled into the note (Cerner) from nursing documentation. Color must be documented otherwise it will not be counted Or two of the following: • Measure CVP • Measure SCv. O 2 • Bedside cardiovascular ultrasound • Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge
- Slides: 39