Kneejerks in hospital medicine 2016 M Nogi updated
![Knee-jerks in hospital medicine 2016 [M. Nogi] updated April 2016](https://slidetodoc.com/presentation_image_h2/973a3846c79669fc2c7b99f46a3cd0a8/image-1.jpg "Knee-jerks in hospital medicine 2016 [M. Nogi] updated April 2016")


. Third universal definition of myocardial")

. Third")
. Third universal definition of myocardial")

. The Erlanger chest pain evaluation protocol: a")


. Journal of Cardiac Failure, 18(10), 792– 798.")
 ¡During the treatment of ADHF ¡ RA, RV, and")

. JAMA Internal Medicine, 173(12), 1058– 1064.")
 ¡mean age 60; mean LVEF")


. Safety of ultrasound-guided thoracentesis in patients with")

. The coagulopathy")




 ¡ “Favors combination")
 • AZM use")

 49% of HCAP patients came from nursing home. Kollef MH,")
 ¡ MRSA")
. Antimicrobial Agents and Chemotherapy, 57(3), 1163–")
 ¡ 91 patients with nasal and throat cultures negative")

. Critical Care")
 ¡ 24 eligible trials ¡ 1 on bacteremia, 0 in CLABSI,")
. Digestive Diseases and Sciences, 59(11), 2790– 2796")
 Inclusion: CPFX susceptible enterobactereciae from blood Cx CPFX iv")

. Contrast-induced acute kidney injury. Journal of the American College")


. Hypertensive crises: challenges and management. Chest,")
. Hypertensive crises: challenges")
. Intravenous hydralazine for")


 ? ¡TIBC is most frequently used along with a")
. Anemia of chronic disease. The New")
. Journal of General Internal Medicine, 20(6), 520– 524.")


. Management of severe hyperkalemia. Critical Care Medicine, 36(12), 3246– 3251.")
. Management of severe hyperkalemia. Critical Care Medicine, 36(12), 3246– 3251.")

. European Journal of Endocrinology / European Federation")



- Slides: 65
Knee-jerks in hospital medicine 2016 [M. Nogi] updated April 2016
Today’s goal ¡Review literatures and evidence FOR or AGAINST our common practice behaviors. ¡Increase awareness of inappropriate tests in hospital medicine, and propose potential areas of QI studies. ¡Avoid the term “Because my ○○ taught me to order so”.
Chest pain = serial Troponin
Tehrani, D. M. , & Seto, A. H. (2013). Third universal definition of myocardial infarction: update, caveats, differential diagnoses. Cleveland Clinic Journal of Medicine, 80(12), 777– 786. doi: 10. 3949/ccjm. 80 a. 12158
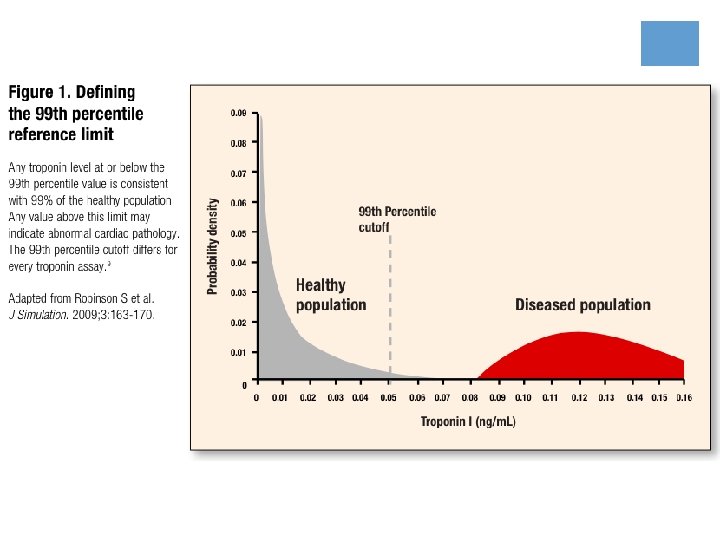
Why serial Troponin?
2 1 0 2 Tehrani, D. M. , & Seto, A. H. (2013). Third universal definition of myocardial infarction: update, caveats, differential diagnoses. Cleveland Clinic Journal of Medicine, 80(12), 777– 786. doi: 10. 3949/ccjm. 80 a. 12158
Tehrani, D. M. , & Seto, A. H. (2013). Third universal definition of myocardial infarction: update, caveats, differential diagnoses. Cleveland Clinic Journal of Medicine, 80(12), 777– 786. doi: 10. 3949/ccjm. 80 a. 12158
ESRD and Troponin ¡Reduced renal clearance is probably not the primary mechanism of persistently elevated troponin levels in patients with CKD, although this issue is controversial (5). ¡A change in troponin level greater than 20% within 9 hours (with 1 value exceeding the 99 th percentile) is recommended for AMI diagnosis among patients with ESRD and suspected ACS (6).
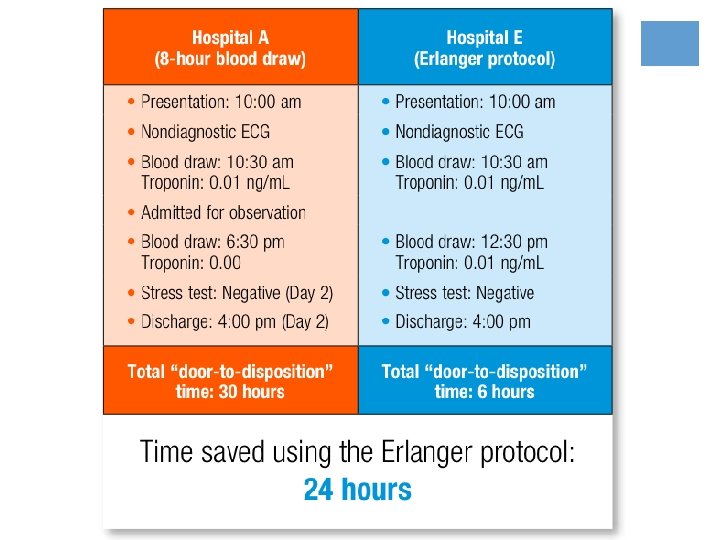
Fesmire, F. M. , et al. (2002). The Erlanger chest pain evaluation protocol: a one-year experience with serial 12 -lead ECG monitoring, two -hour delta serum marker measurements, and selective nuclear stress testing to identify and exclude acute coronary syndromes. Annals of Emergency Medicine, 40(6), 584– 594.
CHF exacerbation =order echo
Choosing Wisely 2011 - American Society of Echocardiography
Ramasubbu, K. , et al. (2012). Journal of Cardiac Failure, 18(10), 792– 798.
2014 Ramasubbu et al. (N=433) ¡During the treatment of ADHF ¡ RA, RV, and IVC sizes ↓ acutely. ¡ MR severity and mitral inflow parameters also improved significantly. ¡ the majority of acute changes in TTE parameters did not have an impact on clinical outcome ¡ There was no significant change in LV dimensions or LVEF despite a significant decrease in invasively measured left-sided filling parameters and increase in cardiac output. Ramasubbu, K. , . (2012). Echocardiographic changes during treatment of acute decompensated heart failure: insights from the ESCAPE trial. Journal of Cardiac Failure, 18(10), 792– 798.
2 major or 1 major and 2 minor criteria
Aliti, G. B. , et al. (2013). JAMA Internal Medicine, 173(12), 1058– 1064.
2013 Aliti et al. (N=75 / Brazil / RCT) ¡mean age 60; mean LVEF 26%. ¡ randomly assigned to strict diet (800 mg of sodium and 800 m. L of fluid per day) vs liberal diets (3 to 5 g of sodium and 2. 5 L of fluid per day). ¡Aggressive fluid and sodium restriction has no effect on weight loss or clinical stability at 3 days and is associated with a significant increase in perceived thirst. sm 1. Only 9% of the screened patients ended up in the study. 2. The randomization may have occurred up to 36 hours into the admission 3. The total sodium and fluid ingestion was not provided, nor was the mean total dose of diuretics. tici i r C Aliti, G. B. , Rabelo, E. R. , Clausell, N. , Rohde, L. E. , Biolo, A. , & Beck-da-Silva, L. (2013). Aggressive fluid and sodium restriction in acute decompensated heart failure: a randomized clinical trial. JAMA Internal Medicine, 173(12), 1058– 1064.
INR>1. 5 = give FFP before thoracentesis
2013 Mayo Clinic, Rochester 1009 US-guided thoracentesis, PT-INR>1. 6 +/- PLT<50 Group 1: no transfusion Group 2: with transfusion Hibbert, R. M. , et al. (2013). Safety of ultrasound-guided thoracentesis in patients with abnormal preprocedural coagulation parameters. Chest, 144(2), 456– 463
Hibbert, R. M. , et al. (2013). Safety of ultrasound-guided thoracentesis in patients with abnormal preprocedural coagulation parameters. Chest, 144(2), 456– 463.
INR>1. 5 with cirrhosis = hold Lovenox
More bleeding More clotting Tripodi, A. , & Mannucci, P. M. (2011). The coagulopathy of chronic liver disease. The New England Journal of Medicine, 365(2), 147– 156.
Prothrombin test & extrinsic pathway The reagants do not contain sufficient amounts of thrombomodulin. PT-time test and related tests are not effective in assessing the risk of hemorrhage in patients with acquired coagulopathies in which there is a concomitant decrease of procoagulants and anticoagulants.
The prevalence of DVT in patients with liver cirrhosis was 4. 7% Lesmana, C. R. A. , (2010). Deep vein thrombosis in patients with advanced liver cirrhosis: a rare condition? Hepatology International, 4(1), 433– 438
Community acquired pneumonia =Azithromycin
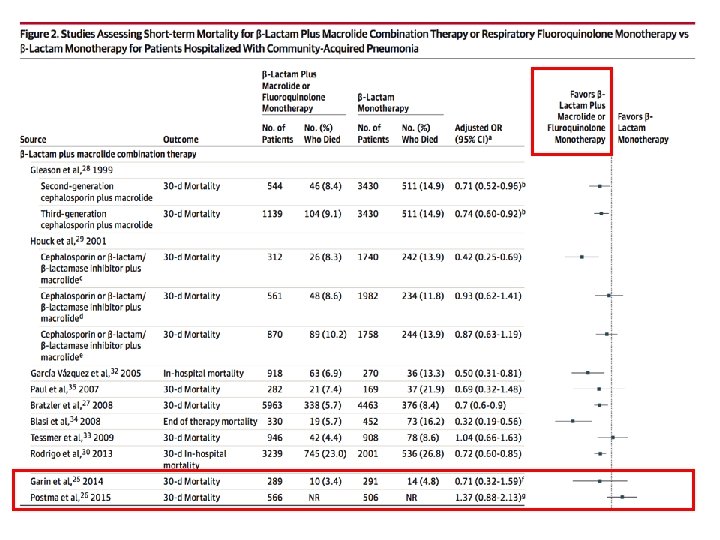
2007 IDSA guidelines ¡Empirical antibiotic therapy should cover both typical and atypical bacterial pathogens ¡ 1 st line : ¡ Respiratory fluoroquinolone monotherapy (moxifloxacin, gemifloxacin, or levofloxacin) ¡ β-Lactam (cefotaxime, ceftriaxone, or ampicillin) and macrolide (azithromycin, clarithromycin, or erythromycin) combination therapy ¡ 2 nd line: ¡ β-Lactam (cefotaxime, ceftriaxone, or ampicillin) and doxycycline combination therapy
JAMA Feb 2016 ¡ 2014 Garlin et al. (Swiss study, N=580) ¡ “Favors combination therapy” ¡ Primary outcome – 7 -day mortality ¡ Strict protocol ¡ 2015 Postma et al. (Deutch study, N=2283) ¡ “Monotherapy was non-inferior” ¡ Loose protocol ¡ High rate (27 -39%) of deviation from randomization ¡ Overestimating the effect of monotherapy? !
AZM: azithromycin Azithromycin harmful? ! • 2014 Mortensen et al. (JAMA) • AZM use was associated with a statistically significant ↓ mortality at 10, 30, and 90 days. • However, prior studies in elderly populations have shown ↑mortality from any cause associated with current use of AZM, within 1 to 5 days of therapy. • 2014 Rao et al (Ann Fam Med) • AZM use was associated with higher risk of death, but no significant association was observed during days 6 to 10 of therapy. • The mechanism of increased risk is thought to be a proarrhythmic effect of the medication, which would be expected to occur during the first 5 days of therapy when drug levels are at their highest.
Pneumonia with recent admission = Cefepime+vanco mycin
2005 Kollef study (N=4543) 49% of HCAP patients came from nursing home. Kollef MH, Shorr A, Tabak YP, et al. Epidemiology and outcomes of health-care–associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005; 128(6): 3854 -3862.
Recent prospective studies ¡ 2011 Chalmers et al. 1 (N=1348 / UK) ¡ MRSA : 2. 2% of HCAP vs 0. 6% of CAP (P = 0. 4), ¡ Pseudomonas aeruginosa : 2. 2% of HCAP vs 0. 3% of CAP (P = 0. 2). ¡ prevalence of S pneumoniae was high in both groups (HCAP, 49. 4%; CAP, 59. 8%; P =. 1). ¡ 2011, Garcia-Vidal et al. 2 (N=2245 / Spain / prospective) ¡ incidence of MDR pathogens was low in HCAP patients (N=557). ¡ MRSA was isolated in just 2 cases ¡ P aeruginosa was scarce in both the HCAP and the CAP groups. 1. Epidemiology, antibiotic therapy, and clinical outcomes in health care-associated pneumonia: a UK cohort study. Clin Infect Dis. 2011; 53(2): 107 -113 2. Garcia-Vidal C, Viasus D, Roset A, et al. Low incidence of multidrug-resistant organisms in patients with healthcare associated pneumonia requiring hospitalization. Clin Microbiol Infect. 2011; 17(11): 1659 -1665
Boyce, J. M. , , et al. (2013). Antimicrobial Agents and Chemotherapy, 57(3), 1163– 1168.
2013 Boyce et al. (N=91) ¡ 91 patients with nasal and throat cultures negative for MRSA in the absence of adequate respiratory cultures had empirical vancomycin therapy discontinued. ¡In the absence of adequate lower-respiratory-tract cultures, it is reasonable to discontinue empirical vancomycin HCAP therapy in patients with negative MRSA nasal and throat cultures and a CPIS of <6.
Bacteremia = IV antibiotics for 10 days
Havey, T. C. , Fowler, R. A. , & Daneman, N. (2011). Critical Care (London, England), 15(6), R 267–R 267.
2011 Meta-analysis (N=155) ¡ 24 eligible trials ¡ 1 on bacteremia, 0 in CLABSI, 3 in intra-abdominal infection, 6 in pyelonephritis, 13 in pneumonia and 1 in SSTI. ¡ Outcome data were available for 155 bacteremic patients: neonatal bacteremia (n = 66); intra-abdominal infection (40); pyelonephritis (9); and pneumonia (40). ¡ Among bacteremic patients receiving shorter (5 -7 days) vs longer (7 -21 days) antibiotic therapy ¡ no significant difference was detected for rates of clinical cure (RR 0. 88, 95% CI: 0. 77 -1. 01), microbiologic cure (RR 1. 05, 95% CI 0. 91 -1. 21), and survival (RR 0. 97, 95% CI 0. 761. 23) ¡ A high rate of failure was seen among the small number of patients receiving short-duration treatment for S. aureus bacteremia. Havey, T. C. , Fowler, R. A. , & Daneman, N. (2011). Duration of antibiotic therapy for bacteremia: a systematic review and meta-analysis. Critical Care (London, England), 15(6), R 267–R 267.
Park, T. Y. , (2014). Digestive Diseases and Sciences, 59(11), 2790– 2796
2014 Park et al. (N=59) Inclusion: CPFX susceptible enterobactereciae from blood Cx CPFX iv 6 d oral 8 d CPFX iv 10 -14 d No difference! Park, T. Y. , . (2014). Early oral antibiotic switch compared with conventional intravenous antibiotic therapy for acute cholangitis with bacteremia. Digestive Diseases and Sciences, 59(11), 2790– 2796.
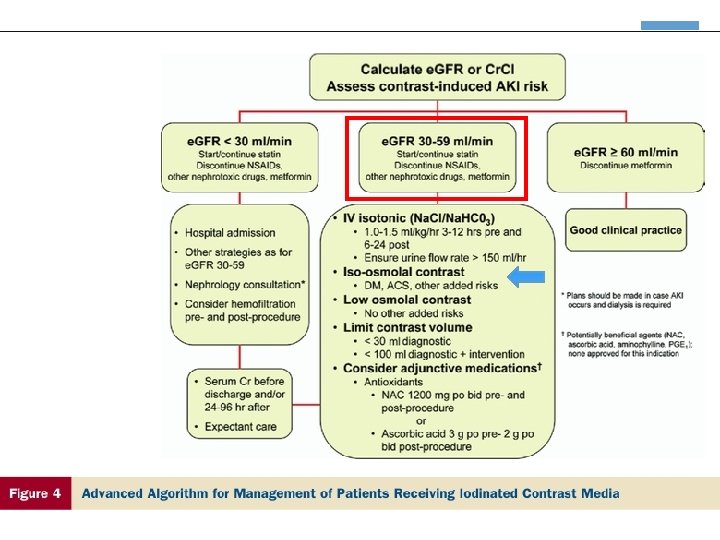
Elevated Cre = Avoid contrast
Mc. Cullough, P. A. (2008). Contrast-induced acute kidney injury. Journal of the American College of Cardiology, 51(15), 1419– 1428. doi: 10. 1016/j. jacc. 2007. 12. 035
CIN requiring dialysis? ¡Most cases of CIN reflect mild transient impairment of renal function ¡ The need for dialysis after contrastinduced AKI is less than 1% ¡ it was considerably higher in some older studies with high-osmolal contrast media (HOCM) Mc. Cullough, P. A. (2008). Contrast-induced acute kidney injury. Journal of the American College of Cardiology, 51(15), 1419– 1428.
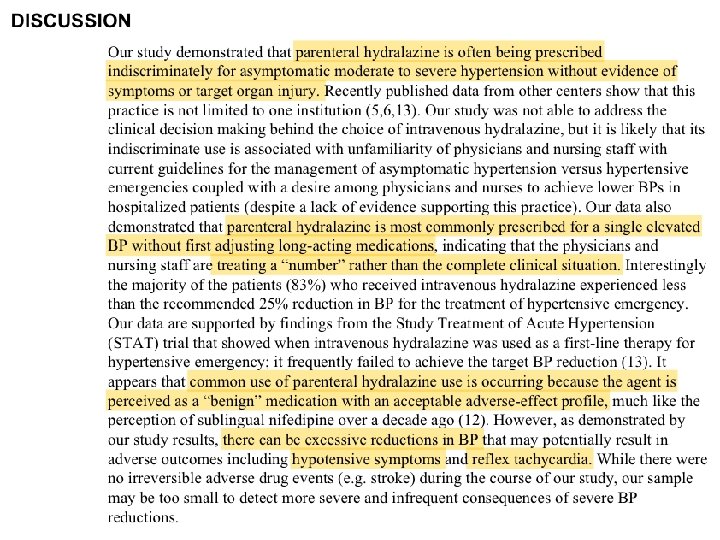
High BP = iv Hydralazine
MARIK, P. E. , & Varon, J. (2007). Hypertensive crises: challenges and management. Chest, 131(6), 1949– 1962. doi: 10. 1378/chest. 06 -2490
Why not Hydralazine? MARIK, P. E. , & Varon, J. (2007). Hypertensive crises: challenges and management. Chest, 131(6), 1949– 1962
Campbell, P. , Baker, W. L. , Bendel, S. D. (2011). Intravenous hydralazine for blood pressure management in the hospitalized patient: its use is often unjustified. Journal of the American Society of Hypertension, 5(6), 473– 477. doi: 10. 1016/j. jash. 2011. 07. 002
Drop in BP is larger with high baseline BP, But very unpredictable Campbell, P. , Baker, W. L. , Bendel, S. D. , & White, W. B. (2011). Intravenous hydralazine for blood pressure management in the hospitalized patient: its use is often unjustified. Journal of the American Society of Hypertension, 5(6), 473– 477
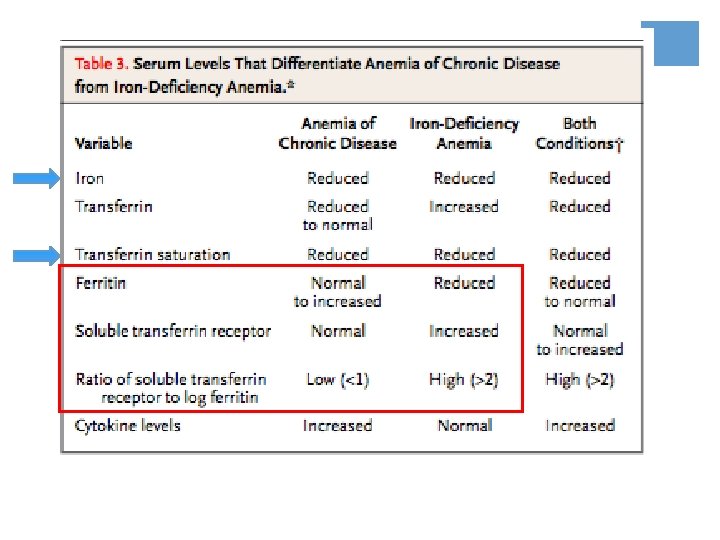
Anemia = Iron panel
Why Total iron-binding capacity (TIBC) ? ¡TIBC is most frequently used along with a serum iron test to evaluate people suspected of having either iron deficiency or iron overload. ¡ In iron deficiency ¡ ↓iron & ↑TIBC =↓transferrin saturation ¡ In iron overload states, such as hemochromatosis, ¡ ↑iron & ↓TIBC =↑transferrin saturation
Weiss, G. , & Goodnough, L. T. (2005). Anemia of chronic disease. The New England Journal of Medicine, 352(10), 1011– 1023. doi: 10. 1056/NEJMra 041809
Thavendiranathan, P. , et al (2005). Journal of General Internal Medicine, 20(6), 520– 524.
2005 Thavendiranathan, et al ¡On average, every 100 m. L of phlebotomy was associated with a decrease in Hgb 0. 7 g/d. L and Hct 1. 9%, respectively. 1 g/L = 0. 1 g/d. L
Hyperkalemia = 1 amp of Bicarb push
Weisberg, L. S. (2008). Management of severe hyperkalemia. Critical Care Medicine, 36(12), 3246– 3251.
Weisberg, L. S. (2008). Management of severe hyperkalemia. Critical Care Medicine, 36(12), 3246– 3251.
Hyponatremia = check TSH
Spasovski, G. , et al. (2014, March). European Journal of Endocrinology / European Federation of Endocrine Societies
Hypothyroid & Hypo. Na ¡Hypo. Na due to hypothyroidism is very rare other than in myxoedema coma, when there is also a decrease in cardiac output and GFR ¡ 2006, Warner et al. ¡ ↓serum Na 0. 14 m. Eq/l for every ↑ 10 m. U/l of TSH ¡ In theory, if the Na 125 was purely caused by hypothyroidism, TSH will be around 714 Warner MH, Holding S & Kilpatrick ES. The effect of newly diagnosed hypothyroidism on serum sodium concentrations: a retrospective study. Clinical Endocrinology 2006 64 598– 599
Take home message 1. Trending Troponin is useful only with symptoms suggesting ACS. Does NOT have to be q 8 hx 3 2. You do NOT have to order an echo for acute CHF exacerbation (if we have one prior) 3. Thoracentesis can be safely done even if INR>1. 5 4. Cirrhosis patients with high INR will still need DVT prophylaxis 5. Giving azithromycin for CAP is okay, but understand the proarryhthmic risk. 6. HCAP and MDR pathogen is still controversial. Nursing home and comorbidities matters more.
Take home message 7. It’s OK to switch to oral antibiotics if clinically stable bacteremia from other sources. Except for S. aureus! 8. Contrast CT scan still be done in patients with GFR 30 -60 9. IV Hydralazine is NOT an appropriate PRN med to control inpatient elevated BP 10. You should check ferritin +/- transferrin saturation for anemia work-up. 11. Pushing Bicarb is NOT effective for hyperkalemia 12. Checking TSH for hyponatremia is NOT so helpful