2016 2015 ATA guideline Haugen et al Thyroid
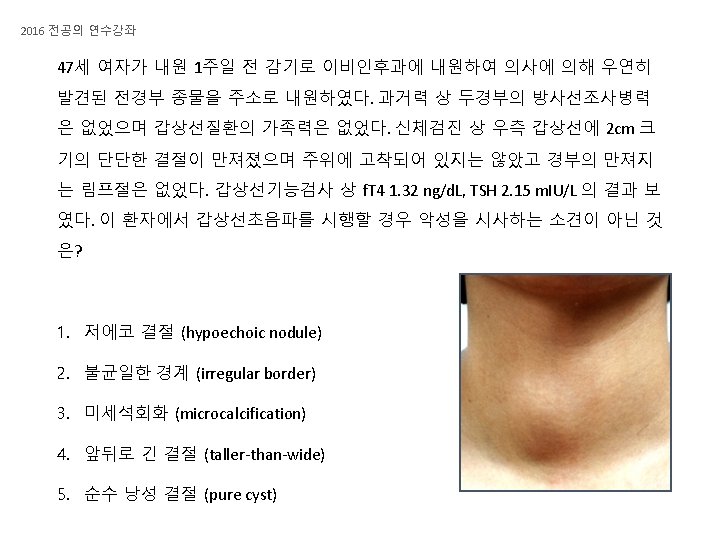



![2016 전공의 연수강좌 이 환자는 [그림 1]과 같은 초음파 소견을 보여 갑상선 결절에 대해](https://slidetodoc.com/presentation_image/56c2099ee0e6624032b2d6c2c30a010d/image-6.jpg "2016 전공의 연수강좌 이 환자는 [그림 1]과 같은 초음파 소견을 보여 갑상선 결절에 대해")
 2. 방사성요오드치료 (radioactive iodine")




 Serum Tg should be measured by an assay that is")
- Slides: 18
2016 전공의 연수강좌 갑상선 결절의 초음파 소견 2015 ATA guideline, Haugen et al. Thyroid 2016
2016 전공의 연수강좌 2015 ATA guideline, Haugen et al. Thyroid 2016
2016 전공의 연수강좌 2015 ATA guideline, Haugen et al. Thyroid 2016
2016 전공의 연수강좌 이 환자는 [그림 1]과 같은 초음파 소견을 보여 갑상선 결절에 대해 초음파 유도하 미세침흡인검사 (sono-guided FNA)를 시행하였으며 [그림 2]와 같은 소견으로 갑상선유두암 (papillary thyroid carcinoma)이 강력히 의심되어 갑상 선전절제술 및 중앙림프절곽청술을 시행하였고 수술병리 결과는 다음과 같 았다. [그림 1] [그림 2] Thyroid, total thyroidectomy: Papillary carcinoma - Tumor location: right lobe - Tumor multicentricity: absent - Size of tumor: 2. 2 x 2. 1 x 1. 7 cm - Encapsulation: complete - Capsular invasion: not applicable - Lymphatic invasion: present (extensive) - Blood vessel invasion: absent - Extrathyroid extension: microscopic - Surgical margins: negative - Lymph node metastasis: present metastasis in 6 out of 9 lymph nodes (0. 5 cm, central LN)
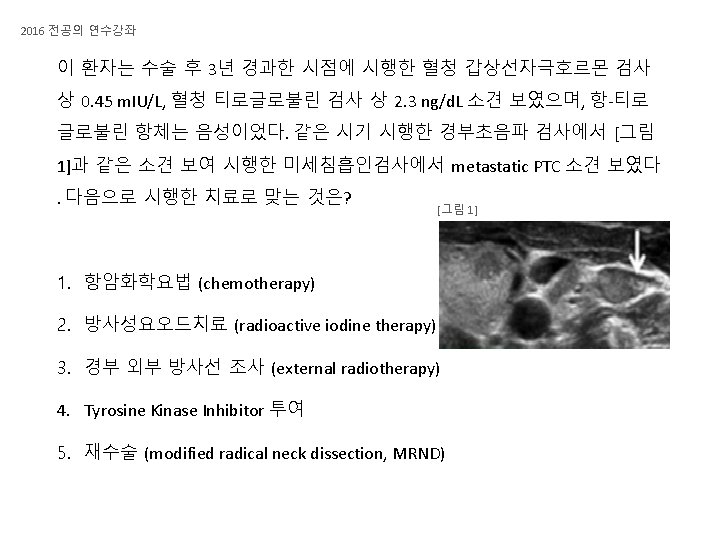
2016 전공의 연수강좌 다음으로 진행하여야 할 치료는? 1. 항암화학요법 (chemotherapy) 2. 방사성요오드치료 (radioactive iodine therapy) 3. 경부 외부 방사선 조사 (external radiotherapy) 4. Tyrosine Kinase Inhibitor 투여 5. 재수술 (modified radical neck dissection, MRND)
2016 전공의 연수강좌 2015 ATA guideline, Haugen et al. Thyroid 2016
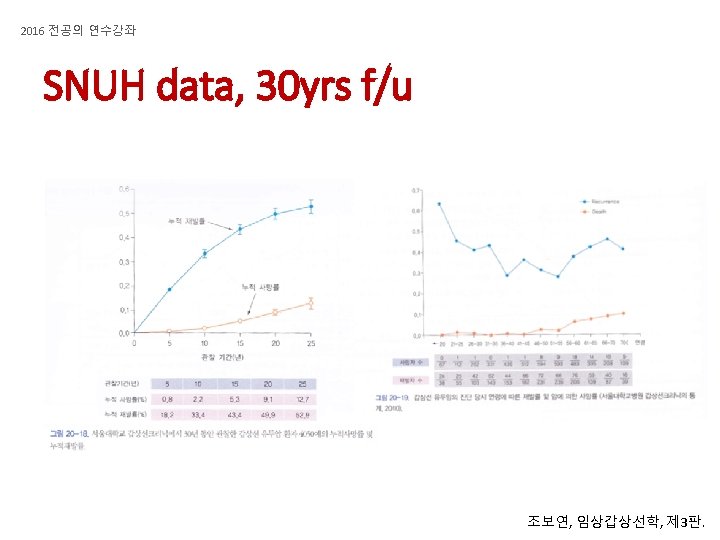
2016 전공의 연수강좌 Recurrence of DTC
2016 전공의 연수강좌 Recurrence, Death and Age
2016 전공의 연수강좌 Thyroid, total thyroidectomy: Papillary carcinoma - Tumor location: right lobe - Tumor multicentricity: absent - Size of tumor: 2. 2 x 2. 1 x 1. 7 cm - Encapsulation: complete - Capsular invasion: not applicable - Lymphatic invasion: present (extensive) - Blood vessel invasion: absent - Extrathyroid extension: microscopic - Surgical margins: negative - Lymph node metastasis: present metastasis in 7 out of 9 lymph nodes (0. 5 cm, central LN) 2015 ATA guideline, Haugen et al. Thyroid 2016
RECOMMENDATION 62 • (A) Serum Tg should be measured by an assay that is calibrated against the CRM 457 standard. Thyroglobulin antibodies should be quantitatively assessed with every measurement of serum Tg. Ideally, serum Tg and anti-Tg antibodies should be assessed longitudinally in the same laboratory and using the same assay for a given patient. (Strong recommendation, High-quality evidence) • (B) During initial follow-up, serum Tg on thyroxine therapy should be measured every 6– 12 months. More frequent Tg measurements may be appropriate for ATA high-risk patients. (Strong recommendation, Moderate-quality evidence) • (D) Serum TSH should be measured at least every 12 months in all patients on thyroid hormone therapy. (Strong recommendation, Low-quality evidence) RECOMMENDATION 63 • (A) In ATA low-risk and intermediate-risk patients who have had remnant ablation or adjuvant therapy and negative cervical US, serum Tg should be measured at 6– 18 months on thyroxine therapy with a sensitive Tg assay (<0. 2 ng/m. L) or after TSH stimulation to verify absence of disease (excellent response). (Strong recommendation, Moderate-quality evidence) RECOMMENDATION 65 • (A) Following surgery, cervical US to evaluate thyroid bed and central and lateral cervical nodal compartments should be performed at 6– 12 months and then periodically, depending on the patient’s risk for recurrent disease and Tg status. (Strong recommendation, Moderate-quality evidence) 2015 ATA guideline, Haugen et al. Thyroid 2016