Introduction Vitamin A deficiency VAD is a major
 is a major nutritional concern in poor societies,")

































")






Which of the following is not a rich source of Vitamin A?")
 Daily Recommended Vitamin D requirement in Infants • A) 100 -200")
 VITAMIN A is not needed for which of the following functions?")
 Bitots spots are seen in the A) Skin B)")
 Vitamin A is Usually given to the infant during • 1)")
 Functions of Vitamin A • 2)")
Clinical features Of Vitamin A deficiency And Its Management")

- Slides: 51
Introduction • Vitamin A deficiency (VAD) is a major nutritional concern in poor societies, especially in lower income countries like INDIA. • Vitamin A is an essential nutrient needed in small amounts for the normal functioning of the visual system, and maintenance of cell function for growth, epithelial integrity, red blood cell production, immunity and reproduction.
VITAMIN A • Vitamin A is an essential Micronutrient because it cannot be biogenerated de novo by animals. It is obtained from plants in the form PROVITAMIN A CAROTENOIDS. The term Vitamin A refers to all Trans Retinol, the alcohol form of the vitamin.
• Storage form of vitamin A is known is RETINAL PALMITATE • The aldehyde form of Vitamin A is RETINAL & Functions in VISION. Physiologically most important form of Vit A metabolite is the acid derivetive, RETINOIC ACID
Sources
SOURCES OF VITAMIN A • The richest sources of Vitamin A include Oil extracted from Shark & Cod liver. • Carrots , Dark green leafy Vegetables, Squash, Oranges and Tomatoes are good Sources. • Infant formulas & many processed food are fortified with preformed
Sources of Vitamin A • Breast Milk fulfils the needs of Vitamin A entirely for the first 6 months of life , & continues to be a an important source upto 2 years.
Absorption & Metabolism • The body acquires Vitamin A either as preformed Vitamin A or as Provitamin A carotenoids. • Vitamin A & Provitamin A are Fat Soluble & their absorption depend adequate lipid & protein within the meal.
ABSORPTION & METABOLISM • Vitamin A is absorbed in the esterified form as a part of Chylomicrons. • Absorption is affected by impaired Chylomicron formation, or when fat absorption is altererd. Retinol is absorbed as the free alchol
Absorption & Metabolism by an active transport system containing a cellular retinol binding protein ( CRBP I I. ) The yellow Beta Carotene also requires Bile salts for absorption & is converted to Vitamin A in the intestinal tract. Once absorbed vitamin A is stored in liver as
Absorption & Metabolism • The liver releases Vitamin A to the circulation , bound to retinol binding protein (RBP) and to a pre albumin (Transthyretin)
Absorption & metabolism Chronic intestinal disoders or Lipid malabsorption syndromes can result in Vitamin A deficiency.
STORAGE • The liver has enormous capacity to store in the form of RETINOL PALMITATE. • under normal conditions a well-fed person has sufficient Vitamin A reserves to meet his need for 6 to 9 months or more.
Excretion of Vitamin A • Not readily excreted • Some lost in urine • Kidney disease and aging increase risk of toxicity because excretion is impaired
Recomended daily allowance • Recommended daily Allowance of Vitamin A is as follows INFANTS --- 300 -400 micrograms CHILDREN -- 400 -600 micrograms ADOLESCENTS – 750 micrograms.
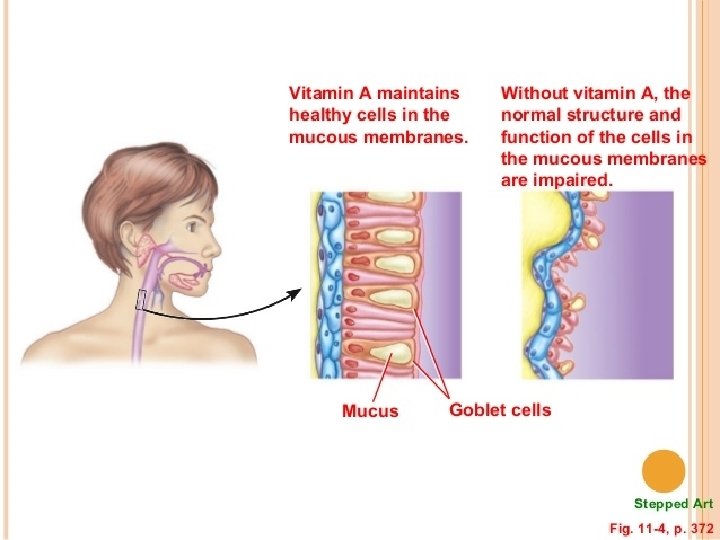
Functions of Vitamin A • Vitamin A has an essential role in vision, particularly Night Vision. • Vitamin A is necessary for regulation of many genes involved in cell division & differentiation. • Many Physiological processes involving Fetal growth & development , Reproduction,
Functions Of Vitamin A Gastrointestinal & respiratory function , and Immunity are dependent on vitamin A. Vitamin A is essential for integrity of Respiratory Epithelium & Skin. CARTENOIDS precursors of Vit A are important Anti Oxidant defences
Causes of Vitamin A Deficiency • SEVERE MALNUTRITION is an important cause of deficiency. • The requirement of vtamin A is increased in PRETERM BABIES & during INFECTIONS ( eg, Measles & Respiratory tract infections) making children prone to deficiency during these states
Causes of VITAMIN A deficiency • CHRONIC DIARRHEA , MALABSOPTIVE STATES and CHRONIC LIVER DISEASES cause significant Vitamin A deficiency.
Deficiency of Vitamin A
Deficiency of Vitamin A • In developing countries it is estimated that 500, 000 pre school children become blind every year owing to vitamin A deficiency, & many of them die because of increased vulnerability to infections particularly Measles.
Clinical features • The most characteristic & specific signs of Vitamin A deficiency are EYE LESIONS • Lesions due to Vitamin A deficiency develop insidiously & rarely occur before 2 yrs of age.
Clinical features • Early features : DEFECTIVE DARK ADAPTATION is the most characteristic early clinical feature, resulting in NIGHT BLINDNESS. PHOTOPHOBIA is a common symptom observed.
As vitamin A deficiency progresses the epithelial tissues of the eye becomes severely altered. In early vitamin A deficiency Cornea Keratinizes , becomes opaque , is susceptible to infections & forms dry scaly layers of cells , that is XEROPTHALMIA.
• In later stages, infection occurs , lymphocytes infiltrates & cornea will become wrinkled. It will degenerate irreversibly ( Known as KERATOMALACIA) , resulting in blindness. • Conjunctiva keratinises & develops plaques known as BITOTS SPOTS.
• The pigment epithelium is the structural element of the Retina. When the pigment epithelium keratinses & degenerates , Child will develop BLINDNESS.
EXTRA OCULAR features • Other clinical features of Vitamin a deficiency includes POOR OVERALL GROWTH, SUSEPTIBILITY TO INFECTIONS, due to squamous metaplasia of respiratory, urinary & vaginal tract epithelium. DIARRHOEA, ANEAMIA, APATHY
• Mental retardation, increased intracranial pressure, with wide separation of intra cranial sutures. • FOLLICULAR HYPERKERATOSIS here the skin becomes dry & scaly, especially over the outer aspect of the limbs , also known as TOAD SKIN or PHRYNODERMA.
Classification of xerophthalmia • • • XN Night blindness X 1 A Conjunctival Xerosis X 1 B Bitot’s spot X 2 Corneal Xerosis X 3 A Corneal ulceration/keratomalacia (< 1/3 corneal surface) • X 3 B Corneal ulceration/keratomalacia (≥ 1/3 corneal surface) • XS Corneal scar • XF Xerophthalmic fundus
Bitot’s Spot • These are foamy and whitish cheese-like tissue spots that develop around the eye ball, causing severe dryness in the eyes. • These spots do not affect eye sight in the day light.
Conjunctival Xerosis • Conjunctiva becomes dry and non wettable. • Instead of looking smooth shiny it appears muddy &wrinkled.
Keratomalacia • One of the major cause for blindness in India. • Cornea becomes soft and may burst • The process is rapid • If the eye collapses vision is lost.
Follicular hyperkeratosis
DIAGNOSIS • In the presence of clinical manifestations , diagnosis is not difficult. • SERUM RETINOL LEVEL usually below 20 mg/dl in Vitamin A deficiency. • CONJUNCTIVAL IMPRESSION CYTOLOGY is a noninvasive
TREATMENT • PREVENTION of Vitamin A deficiency can be achieved by making available the recommended daily allowances to all children. • AS per the NATIONAL PROGRAM for prevention BLINDNESSS , the children in age group of 6 to 11 months should
Should receive 100, 000 I. U of Vitamin A Orally (preferably during Measles immunization) & other children between 1 & 5 years should receive 200, 000 I. U vitamin A every 6 months, in target areas. • Use of Vit A & beta carotene rich food should be encouraged.
• Infants 6 to 12 months recive a half dose & infants less than 6 months one quarter the dose, following the same schedule. • Children with pneumonia, wasting malnutrition , recurrent diarrhoea, & severe infections should also recieve full treatment course of vitamin A
• Fortification of commonly eaten foods with vitamin A can be an effective prophylactic measure. • Treatment of XEROPTHALMIA – 200, 000 IU vitamin A should be given orally on presentation, the following day& whenever possible, 0 ne to four weeks later.
Recommended Xerophthalmia treatment schedule 6 -12 months 100, 000 IU • Immediately IU • Next day 100, 000 IU l. U • 2– 4 weeks later 100, 000 IU IU > 1 yr 200, 000 • Severe Protein-Energy Malnutrition (PEM) drpankajyadav 05@gmail. com
Hypervitaminosis A Toxcity may appear with massive doses or with large doses taken over a large time period. Clinical features : child may have Nausea, Vomiting, Drowsiness, pappilledema, & symptoms suggestive of raised intracranial tension (PSEUDOTUMOR CEREBRI). drpankajyadav 05@gmail. com
• Chronic cases may show marked Anorexia, failure to thrive, Alopecia, seborrheic dermatitis, Hepatomegaly, & tender bone swelling may develop. • RADILOGICALLY May show Hyperosteosis of the shafts of long bones.
• Beta carotene ingestion is seemingly without toxicity , with chronic high consumption stains the skin yellow –orange which is benign & reversible.
MCQ • 1)Which of the following is not a rich source of Vitamin A? • A) Shark liver oil • B) Green leafy Vegetables • C) Sun flower oil • D) Oranges & Tomatoes
• 2) Daily Recommended Vitamin D requirement in Infants • A) 100 -200 micrograms • B) 300 -400 micrograms • C) 50 micrograms
• 3) VITAMIN A is not needed for which of the following functions? A) Night vision B) Immunity C) Functioning of Thyroid Gland D) Reproduction
• • • 4) Bitots spots are seen in the A) Skin B) Conjunctiva C) Cornea D) Fundus
• 5) Vitamin A is Usually given to the infant during • 1) Pulse polio immunisation. • 2) Measles immunisation • 3) BCG Immunisation
• Write Short Notes on • 1) Functions of Vitamin A • 2) Ocular Manifestations Of Vitamin A deficiency. • 3) Hypervitaminosis A • 4) Treatment of Xeropthalmia
• Major Question • 1)Clinical features Of Vitamin A deficiency And Its Management • 2) WHO Classification for Xeropthalmia. Explain Treatment of Xeropthalmia.
Thanking You