Malabsorption syndrome Malabsorption is a clinical term that

Malabsorption syndrome

�Malabsorption is a clinical term that encompasses defects occurring during the digestion and absorption of food nutrients by and infections of the gastrointestinal tract. The digestion or absorption of a single nutrient component may be impaired, as in lactose intolerance due to lactase deficiency. When a diffuse disorder, such as celiac disease or Crohn's disease, affects the intestine, the absorption of almost all nutrients is impaired. �Although presenting symptoms, such as diarrhea and weight loss, may be common, the specific causes of malabsorption are usually established based on physiologic evaluations. The treatment often depends on the establishment of a definitive etiology for malabsorption.

Pathophysiology �To understand the mechanisms of malabsorption, understanding the normal physiologic process of digestion and absorption by the intestinal tract is necessary. �In general, the digestion and absorption of food materials can be divided into 3 major phases: luminal, mucosal, and postabsorptive. �The luminal phase is the phase in which dietary fats, proteins, and carbohydrates are hydrolyzed and solubilized by secreted digestive enzymes and bile.

�The mucosal phase relies on the integrity of the brush-border membrane of intestinal epithelial cells to transport digested products from the lumen into the cells. �In the postabsorptive phase, reassembled lipids and other key nutrients are transported via lymphatics and portal circulation from epithelial cells to other parts of the body. �Perturbation by disease processes in any of these phases frequently results in malabsorption.

Clinical Presentation History The osmotic load resulting from the inability of the intestine to absorb certain nutrient elements causes the presenting symptoms. On occasion, the products of digestion produced by bacterial flora also result in a secretory reaction by the intestine. Diarrhea is the most common symptomatic complaint. Diarrhea frequently is watery, reflecting the osmotic load received by the intestine. Bacterial action producing hydroxy fatty acids from undigested fat also can increase net fluid secretion from the intestine, further worsening the diarrhea. Steatorrhea is the result of fat malabsorption. The hallmark of steatorrhea is the passage of pale, bulky, and malodorous stools. Such stools often float on top of the toilet water and are difficult to flush. Also, patients find floating oil droplets in the toilet following defecation.


Weight loss and fatigue Weight loss is common and may be pronounced; however, patients may compensate by increasing their caloric consumption, masking weight loss from malabsorption. The chance of weight loss increases in diffuse diseases involving the intestine, such as celiac disease and Whipple disease. Flatulence and abdominal distention Bacterial fermentation of unabsorbed food substances releases gaseous products, such as hydrogen and methane, causing flatulence. Flatulence often causes uncomfortable abdominal distention and cramps.

Edema Hypoalbuminemia from chronic protein malabsorption or from loss of protein into the intestinal lumen causes peripheral edema. Extensive obstruction of the lymphatic system, as seen in intestinal lymphangiectasia, can cause protein loss. With severe protein depletion, ascites may develop. Anemia Depending on the cause, anemia resulting from malabsorption can be either microcytic (iron deficiency) or macrocytic (vitamin B-12 deficiency). Iron deficiency anemia often is a manifestation of celiac disease. Ileal involvement in Crohn disease or ileal resection cause megaloblastic anemia due to vitamin B-12 deficiency.

Bleeding disorders Bleeding usually is a consequence of vitamin K malabsorption and subsequent hypoprothrombinemia. Ecchymosis usually is the manifesting symptom, although, occasionally, melena and hematuria occur. Metabolic defects of bones Vitamin D deficiency can cause bone disorders, such as osteopenia or osteomalacia. Bone pain and pathologic fractures may be observed. Malabsorption of calcium can lead to secondary hyperparathyroidism.

Neurologic manifestations Electrolyte disturbances, such as hypocalcemia and hypomagnesemia, can lead to tetany, manifesting as the Trousseau sign and the Chvostek sign. Vitamin malabsorption cause generalized motor weakness (pantothenic acid, vitamin D) or peripheral neuropathy (thiamine), a sense of loss for vibration and position (cobalamin), night blindness (vitamin A), and seizures (biotin).

Physical Examination : General physical examination �Patients may have orthostatic hypotension. �Patients may complain of fatigue. �Signs of weight loss, muscle wasting, or both may be present. �Patients may have signs of loss of subcutaneous fat. �Abdominal examination �The abdomen may be distended, and bowel sounds may be hyperactive. �Ascites may be present in severe hypoproteinemia.

Dermatologic manifestations Pale skin may reveal anemia. Ecchymoses due to vitamin K deficiency may be present. Dermatitis herpetiformis, erythema nodosum, and pyoderma gangrenosum may be present. Pellagra, alopecia, or seborrheic dermatitis may be present. Neurologic examination Motor weakness, peripheral neuropathy, or ataxia may be present. The Chvostek sign or the Trousseau sign may be evident due to hypocalcemia or hypomagnesemia. Cheilosis, glossitis, or aphthous ulcers of the mouth Peripheral edema

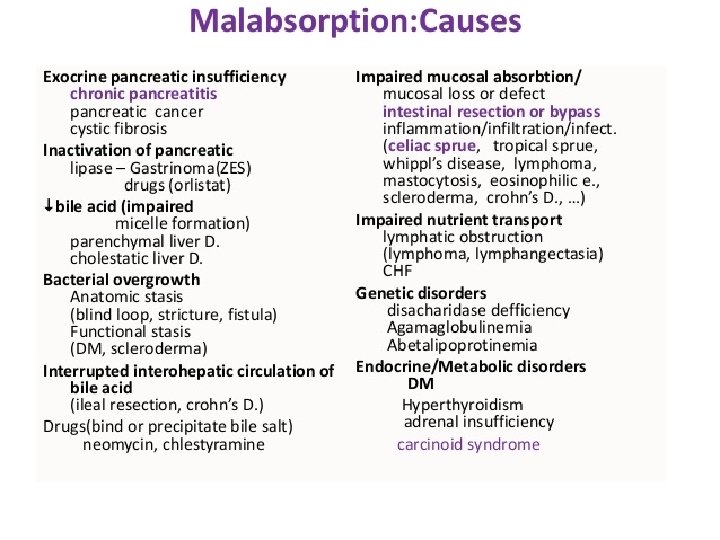
Causes The best way to classify the numerous causes of malabsorption is to consider the 3 phases of digestion and absorption. Luminal phase: Impaired nutrient hydrolysis -The most common cause for impaired nutrient hydrolysis is pancreatic insufficiency due to chronic pancreatitis, pancreatic resection, pancreatic cancer, or cystic fibrosis. The resultant deficiencies in lipase and proteases lead to lipid and protein malabsorption, respectively. -Inactivation of pancreatic enzymes by gastric hypersecretion, as seen in Zollinger-Ellison syndrome, is another cause. -Inadequate mixing of nutrients, bile, and pancreatic enzymes, as seen in rapid intestinal transit, gastrojejunostomy, total and partial gastrectomy, or intestinal resection after mesenteric emboli or thrombosis, also causes impaired hydrolysis. -Rarely, a failure to convert a proenzyme to active form, such as enterokinase and trypsinogen deficiencies, also can cause protein maldigestion and malabsorption.

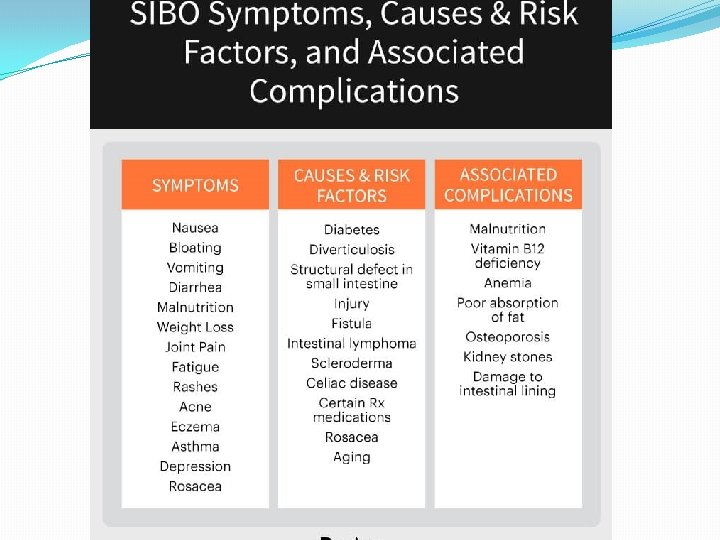
Impaired micelle formation �Impaired micelle formation causes a problem in fat solubilization and subsequent fat malabsorption. This impairment is due to different reasons, including: (1) decreased bile salt synthesis from severe parenchymal liver disease (eg, cirrhosis); (2) impaired bile secretion from biliary obstruction or cholestatic jaundice (eg, primary biliary cirrhosis, primary sclerosing cholangitis); (3) impaired enterohepatic bile circulation, as seen in small bowel resection or regional enteritis; or (4) bile salt deconjugation due to small bowel bacterial overgrowth (SIBO Syndrome). �Stasis of intestinal content caused by a motor abnormality (eg, scleroderma, diabetic neuropathy, intestinal obstruction), an anatomic abnormality (eg, small bowel diverticula, stricture, ischemia, blind loops), or small bowel contamination from enterocolonic fistulas can cause bacterial overgrowth.

Luminal availability and processing �Luminal bacterial overgrowth can cause a decrease in the availability of substrates, including carbohydrates, proteins, and vitamins (eg, vitamin B-12, folate). �Vitamin B-12 deficiency due to pernicious anemia is caused by a lack of intrinsic factor and by pancreatic enzyme deficiency.

Mucosal phase Impaired brush-border hydrolase activity: �Disaccharidase deficiency can lead to disaccharide malabsorption. �Lactase deficiency, either primary or secondary, is the most common form of disaccharidase deficiency. Genetic factors determine primary lactase deficiency; C/T-13910 AND G/A-22018 mutations have been implicated. Secondary lactase deficiency can be due to acute gastroenteritis (rotavirus and giardia infection), chronic alcoholism, celiac sprue, radiation enteritis, regional enteritis, or AIDS enteropathy. �Immunoglobulin A (Ig. A) deficiency (most common immunodeficiency) is due to decreased or absent serum and intestinal Ig. A, which clinically appears similar to celiac disease and is unresponsive to a gluten-free diet.

�Acrodermatitis enteropathica is an autosomal recessive disease with selective inability to absorb zinc, leading to villous atrophy and acral dermatitis. �Autoimmune enteropathy primarily diagnosed in children presenting with intractable secretory diarrhea and villous atrophy. Autoimmune enteropathy is due to antibodies directed against intestinal epithelial and goblet cells. Additional cell types affected by autoantibodies include islet and parietal cells. �Other carbohydrase deficiencies, such as sucraseisomaltase deficiency, may be the cause.

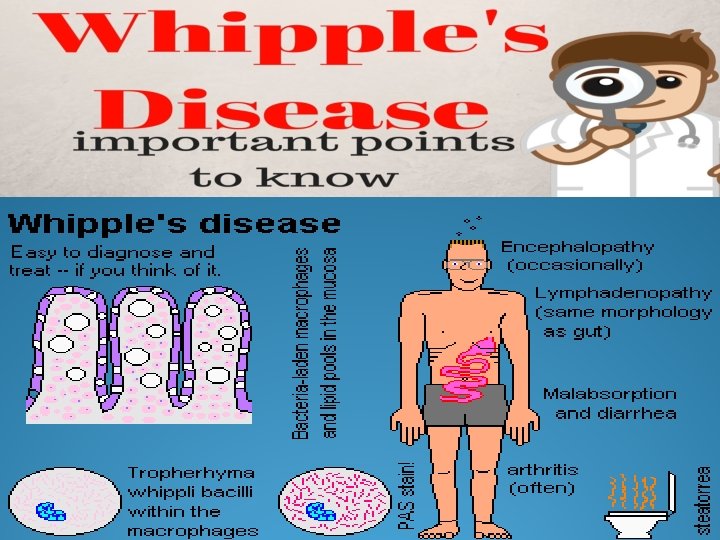
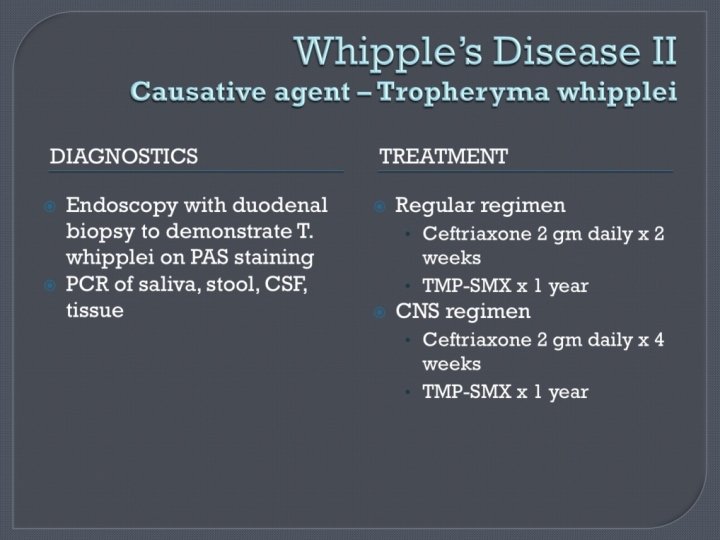
�Impaired nutrient absorption -Nutrient malabsorption is due to inherited or acquired defects. -Inherited defects include glucose-galactose malabsorption, abetalipoproteinemia, cystinuria, and Hartnup disease. -Acquired disorders are far more common and are caused by the following: (1) decreased absorptive surface area, as seen in intestinal resection of intestinal bypass; (2) damaged absorbing surface, as seen in celiac sprue, tropical sprue, Crohn's disease, AIDS enteropathy, chemotherapy, or radiation therapy; (3) infiltrating disease of the intestinal wall, such as lymphoma and amyloidosis; and (4) infections, including bacterial overgrowth, giardiasis, Whipple's disease, cryptosporidiosis, and microsporidiosis.


Laboratory Studies Hematologic tests �A CBC count may reveal microcytic anemia due to iron deficiency or macrocytic anemia due to vitamin B -12 or folate malabsorption. �Serum iron, vitamin B-12, and folate concentrations may help establish a diagnosis. �Prothrombin time may be prolonged because of malabsorption of vitamin K, a fat-soluble vitamin.

Electrolytes and chemistries �Malabsorption can involve electrolyte imbalances, such as hypokalemia, hypocalcemia, hypomagnesemia, and metabolic acidosis. �Protein malabsorption may cause hypoproteinemia and hypoalbuminemia. �Fat malabsorption can lead to low serum levels of triglycerides, cholesterol, and alpha- and betacarotene. �Westergren sedimentation rate is elevated in Crohn disease and Whipple disease.

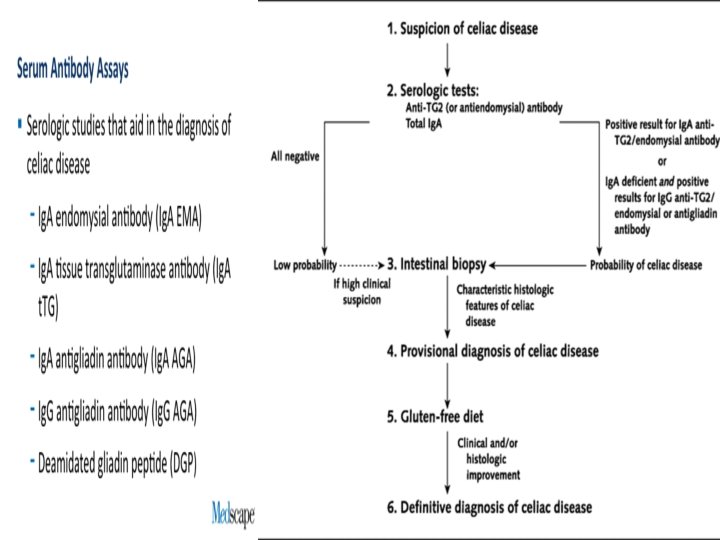
Serology �No serologic tests are specific for malabsorption. �Serum antigliadin and antiendomysial antibodies can be used to help diagnose celiac sprue. �Serum Ig. A can be used to rule out Ig. A deficiency. �Determination of fecal elastase and chymotrypsin (2 proteases produced by the pancreas) can be used to try to distinguish between pancreatic causes and intestinal causes of malabsorption.

Imaging Studies Small bowel barium studies �An abnormal small bowel pattern obtained from barium studies of the upper gastrointestinal tract may reveal the nature of malabsorption. �The mucosa pattern associated with celiac disease often becomes obliterated or coarsened. �Flocculation of the barium occurs in the gut lumen. �Small bowel dilatation and diverticulosis are frequently identified in scleroderma. �Regional enteritis of the small intestine can lead to stricture, ulceration, and fistula formation. �Other anatomic abnormalities, such as surgical changes or enterocolonic fistula, also can be detected on x-ray films.

�CT scan of the abdomen: Performing this study may help detect evidence of chronic pancreatitis, such as pancreatic calcification or atrophy. Enlarged lymph nodes are seen in Whipple disease and lymphoma. �Endoscopic retrograde cholangiopancreatogram (ERCP): This study helps document malabsorption due to pancreatic or biliary-related disorders. �Plain abdominal x-ray film: Pancreatic calcifications are indicative of chronic pancreatitis

Other Tests of fat malabsorption �This usually is the first test because many disease processes result in fat malabsorption. �For a quantitative measurement of fat absorption, a 72 -hour fecal fat collection is often performed and is considered the criterion standard. �Qualitative tests include the acid steatocrit test and Sudan III stain of stool, but these tests are less reliable. �Raman et al suggest that a novel clinical test that uses levels of serum retinyl palmitate to identify severe cases of fat malabsorption may be useful relative to the 72 -hour fecal fat test. � Instruct patients to consume a normal amount (80 -100 g/d) of fat before and during the collection. Based on this intake, fecal fat excretion in healthy individuals should be less than 7 g/d.

D-xylose test �If the 72 -hour fecal fat collection results demonstrate fat malabsorption, the D-xylose test is used to document the integrity of the intestinal mucosa. �Facilitated diffusion in the proximal intestine primarily absorbs D-xylose. �Approximately half of the absorbed D-xylose is excreted in urine, unmetabolized. If the absorption of D-xylose is impaired due to either a luminal factor (eg, bacterial overgrowth) or a reduced or damaged mucosal surface area (eg, surgical resection, celiac disease), urinary excretion is lower than normal. �Cases of pancreatic insufficiency usually result in normal urinary excretion because the absorption of D-xylose is still intact.

Tests of carbohydrate absorption �A simple sensitive test for carbohydrate malabsorption is the hydrogen breath test, in which patients are given an oral solution of lactose. � In cases of lactase deficiency, colonic flora digest the unabsorbed lactose, resulting in an elevated hydrogen content in the expired air. �Bacterial overgrowth or rapid transit also can cause an early rise in breath hydrogen, necessitating the use of glucose instead of lactose to make a diagnosis. However, 18% of patients are hydrogen nonexcretors, causing a false-negative test result.

Test of bile salt absorption �The bile salt breath test can determine the integrity of bile salt metabolism. �The patient is given oral conjugated bile salt, such as glycine cholic acid with the glycine radiolabeled in the carbon position. �The bile salt is deconjugated and subsequently metabolized by bacteria, leading to a radioactively labeled elevated breath carbon dioxide level if interrupted enterohepatic circulation, such as bacterial overgrowth, ileal resection, or disease, is present.

Schilling test �Malabsorption of vitamin B-12 may occur as a consequence of deficiency of intrinsic factor (eg, pernicious anemia, gastric resection), pancreatic insufficiency, bacterial overgrowth, ileal resection, or disease. �The 3 -stage Schilling test results often can help differentiate these conditions.

13 C-D-xylose breath test �Hope et al suggest that small intestinal malabsorption in chronic alcoholism may be determined by a 13 C-D-xylose breath test. � The investigators evaluated the 13 C-D-xylose breath test in 14 alcoholics, compared the breath test results with those of untreated celiac patients and healthy controls, and correlated the breath test findings to morphologic findings of the duodenal mucosa. [14] Hope et al found significantly reduced absorption of 13 C-D-xylose in the alcoholic individuals relative to the healthy controls, whereas the time curve of 13 C-D-xylose absorption in the alcoholics was similar in appearance to that of the untreated celiac patients. In addition, despite few light microscopic changes in the alcoholics, morphologic pathology, primarily a reduced surface area of microvilli, was observed under electron microscopy in the majority of the patients.

Procedures 1 -Upper endoscopy with small bowel mucosal biopsy: � Establishing a definitive diagnosis of malabsorption of the mucosal phase often can be achieved by histologic examination of biopsied mucosal specimens obtained during routine upper endoscopy. � Examples of conditions that can be diagnosed this way include celiac sprue, giardiasis, Crohn disease, Whipple disease, amyloidosis, abetalipoproteinemia, and lymphoma. � Magnification narrow band imaging with upper endoscopy for the evaluation of duodenal villi may be predictive for the presence of villous atrophy or normal villi, which could be be helpful for targeted biopsies. In a prospective study, 16 of 100 patients who underwent upper endoscopy with magnification narrow band imaging for suspected malabsorption had histologically confirmed villous atrophy. Two endoscopists independently demonstrated this technique had a greater than 80% sensitivity (87. 5% vs 81. 3%) and a more than 92% specificity (95. 2% vs 92. 9%) for detecting villous atrophy; the interobserver agreement was very good (kappa = 0. 87).

2 -Histologic Findings �Depending on the cause, the histologic features of malabsorption vary. �A frequently encountered histologic finding is villous atrophy, which is seen in celiac disease, tropical sprue, viral gastroenteritis, bacterial overgrowth, inflammatory bowel disease, immunodeficiency syndromes, lymphoma, and radiation enteritis.

Medical Care Two basic principles underlie the management of patients with malabsorption, as follows: (1) the correction of nutritional deficiencies, and (2) when possible, the treatment of causative diseases. Nutritional support � Supplementing various minerals, such as calcium, magnesium, iron, and vitamins, which may be deficient in malabsorption, is important. � Caloric and protein replacement also is essential. � Medium-chain triglycerides can be used as fat substitutes because they do not require micelle formation for absorption and their route of transport is portal rather than lymphatic. � In severe intestinal disease, such as massive resection and extensive regional enteritis, parenteral nutrition may become necessary.

Treatment of causative diseases �A gluten-free diet helps treat celiac disease. �Similarly, a lactose-free diet helps correct lactose intolerance; supplementing the first bite of milkcontaining food products with Lactaid also helps. �Protease and lipase supplements are therapy for pancreatic insufficiency. �Antibiotics are therapy for bacterial overgrowth. �Corticosteroids, anti-inflammatory agents, such as mesalamine, and otherapies are used to treat regional enteritis.

what Is Gluten Intolerance? First you must separate gluten intolerance into three distinct categories: Celiac Disease, Non-Celiac Gluten Sensitivity and a Wheat Allergy. (Technically, a wheat allergy is not an intolerance to gluten. )
 trigger your immune")
Celiac Disease occurs when the proteins in gluten (glutenin and gliadin) trigger your immune system to overreact with strong and unusual anitbodies. Over time, the reaction caused by these antibodies wears down the villi that line the walls of the intestine (this process is called villous atrophy). Celiac disease also triggers inflammation of the intestinal wall. The combination of absorption-killing villous atrophy and inflammation sets off a domino-effect of increasingly serious health problems. Celiac disease is also associated with leaky gut syndrome (or intestinal hyperpermeability). Undigested proteins and toxins move through the intestinal wall and into the bloodstream. This may be the cause of conditions like Duhring’s dermatitis herpetiformis (Duhring’s disease), a nasty gluten intolerance rash.

�Scalloping in the duodenum in celiac disease

- Slides: 46