THE EFFECTS OF PERIOPERATIVE MEDICATIONS BY NANCY OMALLEY

THE EFFECTS OF PERIOPERATIVE MEDICATIONS BY NANCY O’MALLEY, BSN MA RN CPAN CAPA

OBJECTIVES 1. 2. Discuss the effects of perioperative medications Identify conditions that affect perioperative medications
 PHYSICAL STATUS CLASSIFICATION n n Used to determine the")
AMERICAN SOCIETY OF ANESTHESIOLOGISTS (ASA) PHYSICAL STATUS CLASSIFICATION n n Used to determine the complexity of the patient’s medical condition after the H&P are completed. Affects the modes and methods of anesthesia to be used

ASA STATUS n ASA I n n ASA II n n Normal, healthy patient Patient with mild, systemic disease ASA III n Patient with severe systemic disease that limits activity but is not incompacitating

ASA STATUS n ASA IV n n ASA V n n Patient is not expected to survive 24 hours without the operation ASA VI n n Patient with severe systemic disease that is a constant threat to life Patient passed brain death criteria and is an organ donor E-Emergency patient with unknown history
 n GENERAL")
FOUR TYPES OF ANESTHESIA n LOCAL n REGIONAL n SEDATION/ANALGESIA (MAC) n GENERAL
 n Subcutaneous lidocaine injections n EMLA cream n")
LOCAL n Local anesthetic agents (‘caines) n Subcutaneous lidocaine injections n EMLA cream n Sprays (benzocaine) n Inhibits Na+ influx into nerve cells Observe for ‘caine toxicity n RX: Intralipids § Observe for methemaglobinemia RX: Methylene Blue

REGIONAL ANESTHESIA n Local anesthetic agents-’caines n n n Neuraxial: Epidural/spinal/caudal blocks Axillary block Bier block Stellate ganglion block Interscalene block Digital, ankle, wrist, femoral, and others Observe for toxicity

AXILLARY AND BIER BLOCKS n Axillary block n n n Observe for intravascular injection of ‘caine Fully monitor during injection Bier block n n Observe for tourniquet complications Observe for early release of tourniquet or inadequate metabolism of ‘caine

INTERSCALENE BLOCK

INTERSCALENE BLOCK n Normal symptoms n Mild chest heaviness-partial phrenic nerve block n Mild hoarseness, weak voice-laryngeal nerve blockade n Horner’s syndrome-ipsilateral myosis, ptosis, anhidrosis, nasal stuffiness, corneal hyperemia

INTERSCALENE BLOCK n Abnormal symptoms n Dyspnea-phrenic nerve paralysis vs pneumothorax n Total paralysis-cervical epidural/spinal injection n Seizures-vertebral artery injection n CNS excitation syndrome-venous injection n Hematoma n Nerve Injury

BENEFITS OF REGIONAL ANESTHESIA n Better perioperative outcomes compared to general anesthesia n n n Better analgesia Reduced risk for deep vein thrombosis Fewer myocardial events Fewer pulmonary complications Possibly reduced tumor recurrence rate Gupt, P. K& Hopkins, P. M. (2012). Regional anaesthesia for all? British Journal of Anaesthesia 109 (1): 7– 9.

EPIDURAL

dorsal horn dura needle pia mater arachnoid

GOALS OF EPIDURALS/SPINALS n Paralysis and anesthesia-local anesthetic agents block sympathetic, sensory and motor nerves as they emerge from the dura n Pain control-opioids occupy the opiate pain receptors in the dorsal horn of the spinal cord

ANESTHETIC AGENTS n Anesthetic agents-sympathetic, sensory, and motor block n n n Lidocaine-more neurotoxic sx than bupivacaine; shorter acting Bupivacaine (Marcaine)-longer acting Ropivicaine-less cardiotoxicity; less motor block Tetracaine-more motor than sensory effects; longest acting Levobupivacaine-less cardiotoxicity
-moderate spread")
ANALGESIC AGENTS n Opioids-block Mu pain receptors n Fentanyl-least spread n Hydromorphone (Dilaudid)-moderate spread n Duramorph/Astramorph (preservative-free morphine)-most spread n Epinephrine-slows absorption, prolongs effects n Also used during epidural catheter placement as a test for catheter tip location

ANESTHESIA ADJUNCTIVES n n Given via epidural or IV NMDA receptor antagonist-prevents central sensitization in dorsal horn neurons n n Ketamine Alpha-2 agonists-block sympathetic arm of the autonomic nervous system; enhance central neural blockade n n Clonidine Dexmedetomidine Chandrakantan, A. , & Glass, P. S. A. (2011). Multimodal therapies for postoperative nausea and vomiting, and pain. British Journal of Anaesthesia 107 (S 1): i 27–i 40.

ANESTHETIC BLOCKADE OCCURS RESOLVES sympathetic motor sensory sympathetic sensory motor

EFFECTS OF SYMPATHETIC BLOCKADE § Peripheral vasodilation below block level: n n n Hypotension and loss of body heat Increased venous pooling/stasis Decreased heart rate-blockade of cardioaccelerator fibers of sympathetic system n Decreased cardiac output n Decreased coronary perfusion

MANAGEMENT OF SYMPATHETIC BLOCKADE Decrease effects of blockade by: n Adequate fluid therapy n TEDS or alternating pressure stockings n Mild elevation of the head of the bed unless ordered otherwise n Passive ROM to legs n If symptomatic-elevate legs, increase fluids, give vasopressors

DERMATOME LEVELS n n n C-8 T-2 T-4 T-10 L-1 S-1 little finger shoulders nipples umbilicus inner thigh lateral ankle Perineum comes back last!!

EPIDURAL ANESTHESIA n Apnea causes n “Total spinal”-rare, occurs during insertion or from migration of catheter through the dura n Inadequate cerebral perfusion-hypovolemia n Opioid affecting respiratory center-late sign; migrates via CSF or venous uptake

EPIDURAL ANESTHESIA n Post dural puncture headache n Causes: n “Wet tap” diagnostic lumbar puncture, or migration of epidural catheter n Signs: n n Throbbing pain when upright-better when flat Treatment: n Bed rest, hydration, analgesics, abdominal binders, caffeine, hydrocortisone, and ergotamine/triptane n Autologous blood patch

EPIDURAL ANESTHESIA n Resolution assessments n Stable VS and temperature n Leg temperature is normal n Ability to plantar reflex against resistance n Ability to lift buttocks off bed

GOT SLOW MOVERS?
 n MAC-monitored anesthesia care Moderate sedation under an anesthesia provider n Intraop")
SEDATION/ANALGESIA (MAC) n MAC-monitored anesthesia care Moderate sedation under an anesthesia provider n Intraop and postop monitoring per Moderate Sedation standards n

OVERVIEW of GENERAL ANESTHESIA n Preoperative meds n Intraoperative meds n Postoperative meds

PREOPERATIVE MEDS Sedatives n Anti-emetics n Antibiotics n Patient’s regular med regimen n

SEDATIVESBENZODIAZEPINES n n n n Potentiate opioids Are potentiated by opioids Cause apnea/respiratory depression Cause orthostatic hypotension Cause amnesia for up to 24 hours Raise the seizure threshold Are reversed by flumazenil Can have paradoxical reaction
 n Causes profound amnesia n Titrate slowly; wait 2 minutes")
SEDATIVES n Midazolam (Versed) n Causes profound amnesia n Titrate slowly; wait 2 minutes between doses n Lasts up to 24 hours n Paradoxical reactions-sexual fantasies n Diazepam (Valium) n Lasts longer n Burns IV n Incompatible with other meds n Lorazepam (Ativan) n Moderate duration n Minimal CV, sedation effects

PONV MAJOR Risk Factors n n n n n Female History of PONV History of motion sickness Non-smoker Use of opioids, volatile anesthetics, nitrous oxide postop If 0 factors-20% risk If 1 factors-40% risk If 2 factors-60% risk If 3+ factors-80% risk n PDNV may have different risk factors ASPAN’s Clinical Practice Guideline PONV-PDNV

THE BRAIN Pons 4 th Ventricle CTZ Medulla Vomiting center

THE EMETIC CENTER CTZ Receives Blood-born stimuli & has contact with CSF 4 th ventricle Lateral reticular formation Vomiting Center Receives stimuli from CTZ, vagus, cerebral cortex, labyrinthovestibular center, cerebellum, etc.
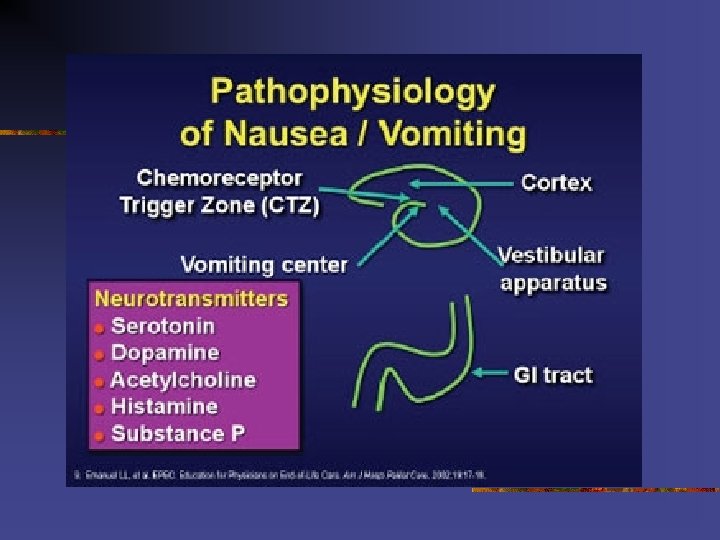

ANTI-EMETICS n Vomiting reflex coordinated by vomiting center n VC located in lateral reticular formation of the medulla oblongata in the mid-brainstem n Close to vagus nerve n Receives stimuli from GI, mediastinum, renal pelvis, peritoneum, genitalia, visual center, vestibular apparatus CTZ-located in floor of 4 th ventricle n No blood brain barrier; receives blood-borne chemical stimuli such as anesthetic agents n Does have contact with CSF n Chatterjee, S. , Rudra, A. , & Sengupta, S. (2011). Current concepts in the management of postoperative nausea and vomiting. Anesthesiology Research and Practice: 748031.

ANTI-EMETICS n Neurotransmitters receptors in the CTZ n n n Choline Dopamine Histamine Serotonin Opioid NK-1 (and in vomiting center)

ANTI-EMETICS n n Work in different ways May cause CNS symptoms such as: n n n Drowsiness Sedation Agitation/confusion Dizziness May cause extrapyramidal symptoms

repetitive movements “coming out of my skin”
, Atropine, Trimethobenzamide (Tigan) n Dopamine-(3")
ANTI-EMETICS n Neurotransmitters receptor antagonists n Choline-Scopolamine, Dimenhydrinate (Dramamine), Atropine, Trimethobenzamide (Tigan) n Dopamine-(3 types of drugs) Promethazine (Phenergan), Prochlorperazine (Compazine), Chlorpromazine (Thorazine); Metoclopramide (Reglan); Droperidol (Inapsine); Haloperidol (Haldol)
, Famotidine (Pepsid), Dimenhydrinate (Dramamine)-also has anticholinergic activity, Diphenhydramine (Benadryl), Hydroxyzine")
ANTI-EMETICS n Histamine-Ranitidine (Zantac), Famotidine (Pepsid), Dimenhydrinate (Dramamine)-also has anticholinergic activity, Diphenhydramine (Benadryl), Hydroxyzine (Vistaril, Atarax) n Serotonin-Ondansetron (Zofran), Dolasetron (Anzemet), Granisetron (Kytril), Metoclopramide, Palonosetron (long-acting)-PDNV n Opioid-Naloxone (Narcan), Nalmefene (Revex)
 NK-1 receptor antagonist n n Works on NK-1 receptors in")
ANTI-EMETICS n Aprepitant (Emend) NK-1 receptor antagonist n n Works on NK-1 receptors in both the CTZ and the Vomiting Center Study of 140 craniotomy patients at Duke U comparing aprepitant+dexamethosone vs ondansetron+dexamethosone n Incidence of vomiting 6% vs 21% over 48 hours n No difference in nausea (69% vs 60%) n Works on vomiting more than nausea Habid, A. S. , Keifer, J. C. Borel, C. O. , Shite, W. D. & Gan, T. J. (2011). A comparison of the combination of aprepitant and dexamethasone versus the combination of ondansetron and dexamethasone for the prevention of postoperative nausea and vomiting in patients undergoing craniotomy. Anesthesia and Analgesia, 112(4): 813 -8.
-decreases gastric secretions n Metoclopramide (Reglan)-empties stomach n Dexamethasone (Decadron)-?")
OTHER ANTI-EMETICS n Famotidine (Pepcid)-decreases gastric secretions n Metoclopramide (Reglan)-empties stomach n Dexamethasone (Decadron)-? how it works? n ? Prostaglandin inhibition in periphery n 5 -10 mg just prior to induction n Bicitra-gastric and urinary alkalizer n Propofol (Diprivan)-low doses

MEDICATIONS-Adverse Effects n Serotonin antagonists-Headache, diarrhea, constipation, arrhythmia n Neurokinin inhibitors-Dizziness, diarrhea, headaches, weakness n Steroids-Dizziness, mood changes, nervousness n Antihistamines-Confusion, drying of mucosal membranes, sedation, urinary retention n Butyrophenones-Prolonged QT interval (at doses ≥ 0. 1 mg/kg), hypotension, tachycardia, extrapyramidal symptoms Chandrakantan, A. , & Glass, P. S. A. (2011). Multimodal therapies for postoperative nausea and vomiting, and pain. British Journal of Anaesthesia 107 (S 1): i 27–i 40.

COMPLEMENTARY THERAPIES n Aromatherapy-scents to sniff n Isopropyl alcohol vapor inhalation was effective in reducing the use of rescue anti-emetics Hines, S. , Steels, E. , Chang, A. &Gibbons, K. (2012). Aromatherapy for treatment of postoperative nausea and vomiting. Journal of Peri. Anesthesia Nursing, 29(1), pp. 5 -11. § Quese. Ease was favorably received by most patients and represents an effective treatment option for postoperative nausea. Hodge, N. S. , Mc. Carthy, M. S. & Pierce, R. M. (2014). A prospective randomized study of the effectiveness of aromatherapy for relief of postoperative nausea and vomiting. Journal of Peri. Anesthesia Nursing, 29(1), pp. 5 -11.

COMPLEMENTARY THERAPIES n Controlled breathing and peppermint oil Though not statistically significant, controlled breathing was more efficacious than aromatherapy n CB can be initiated immediately n n Sites, D. S. , Johnson, N. T. , Miller, J. A. , Torbush, P. H. , Hardin, J. S. , Knowles, S. S. , Nance, J. , Fox, T. H. , & Tart, R. C. (2014). Controlled breathing with or without peppermint aromatherapy for postoperative nausea and/or vomiting symptom relief: A randomized controlled trial. Journal of Peri. Anesthesia Nursing, 29(1), pp. 12 -19.

COMPLEMENTARY THERAPIES n n Stimulation of the P 6 acupressure point Accupuncture n Compared with sham treatment P 6 acupoint stimulation significantly reduced: reduced nausea vomiting and the need for rescue antiemetics Lee, A. & Fan, L. T. Y. (2011). P 6 acupoint stimulation prevents postoperative nausea and vomiting with few side effects. Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No. :

PONV-PDNV n More causes: n n n n Pain ↓ blood sugar-LR in OR; NPO prolonged ↓ Na-fluid overload Hypotension/bradycardia/dysrhythmias Hypovolemia-vasodilation, ↓IV fluids, NPO, drains, insensible surgical losses, diarrhea, N/V preop Hypoxemia-↓O 2 and↑CO 2 ↑ICP, intraocular pressure Motion sickness-whipping through the halls

ANTI-EMETICS Multicauses=Multimodal therapies

OTHER PREOP MEDS Some meds potentiate or prolong n-m blockers n n n n Antibiotics (e. g. , Gentamicin, Streptomycin, Vancomycin Clindamycin, Polymixin A & B, tetracycline, and others) Furosemide (Lasix) Quinidine, procainamide Calcium channel and beta blockers Lithium, Magnesium Procaine, lidocaine Chlorpromazine Immunosuppressive agents Odom-Forren, J. (2013). Drain’s perianesthesia nursing: A critical approach (6 th ed). Missouri: Saunders-Elsevier.

OTHER PREOP MEDS n Patient’s home or pre-surgical regimen n Pain/sedation meds n Cardiac n Diabetic meds n Eye medications-(ecothiophate) glaucoma meds n Herbals and other supplements

PAIN-ADJUNCTIVES Adjunctives: Given preop to decrease postop pain n Anticonvulsants-help control spinal nerve sensitization n Gabapentin (Neurotin) n 40 adult females-total mastectomy for cancer n Gabapentin 600 mg vs placebo n Post op pain scores at 30 minutes, 1 hour and 2 hours n Less morphine consumption n No significant adverse effects n Not beneficial for all surgeries Bharti, N. , et al. (2013). Effect of gabapentin pretreatment on propofol consumption, hemodynamic variables, and postoperative pain relief in breast cancer surgery. Acta Anaesthesiologica Taiwanica, 51(1): 10 -3.

CARDIAC PROTECTION n Beta Blockers n n Do not stop if using preoperatively Reduces morbidity/death from postop myocardial ischemia but may increase risk for stroke, severe hypotension, severe bradycardia Reduces stress/anesthesia responses Do not start if no indications White, C. M. , Talati, R. , Phung, O. J. , Baker, W. L. , Reinhart, K. , Sedrakyan, A. , Kluger, J. , & Coleman, C. I. (2010) Benefits and risks associated with beta-blocker prophylaxis in noncardiac surgery. American Journal of Health-System Pharmacists, 67(7): 523 -30.

INTRAOPERATIVE MEDICATIONS n n Induction Intubation Incision Wake up

INDUCTION AGENTS n n n Put brain to sleep Are hypnotic Are amnestic Produce no analgesia May cause histamine release n n Vasodilatation Hypotension
 n IV hypnotic n Contraindicated if soy or egg")
INDUCTION AGENTS n Propofol (Diprivan) n IV hypnotic n Contraindicated if soy or egg allergy n Fast onset/offset n Anti-emetic n Vein irritation n Thiopental (Pentothal) n Histamine release n Hypotension/bronchospasm n Depresses respiratory center n Stores in fat n Pain/necrosis with extravasation
 n Short acting (4 -7 minutes) n Muscle twitching,")
INDUCTION AGENTS n Methohexital (Brevital) n Short acting (4 -7 minutes) n Muscle twitching, tachycardia, transient hypotension, N&V, laryngospasm, apnea n Etomidate (Amidate) n Short acting (5 -10 minutes) n Used for rapid sequence induction/intubation n Low cardiovascular and respiratory risk profile n Lowers ICP & IOC n Induces adrenal insufficiency up to 48 hrs after a single dose-may increase mortality in critically ill & ASA III/IV
 n Potent bronchodilator; no loss of laryngeal reflexes; increased")
INDUCTION AGENTS n Ketamine (Ketalar) n Potent bronchodilator; no loss of laryngeal reflexes; increased secretions n Related to PCP=dissociative reactionmidazolam may reduce confusion, hallucinations n Nystagmus indicator

NEUROMUSCULAR BLOCKERS TWO CATEGORIES OF NM BLOCKERS: n Depolarizing n n Used for intubation Non-depolarizing n Prevents movement and reflex reactions during surgery
 n Causes muscle depolarization/fasciculations n Has fast onset/offset-used")
DEPOLARIZING NM BLOCKERS n Succinylcholine (Anectine) n Causes muscle depolarization/fasciculations n Has fast onset/offset-used for intubation (RSI) n Causes myalgias n Increases: Intraocular, intracranial, intragastric pressures n Contraindicated for children-undx myopathies may develop rhabdomyolysis and cardiac arrest n Serum K increases-avoid in burns, trauma, n-m disorders n Triggers MH n Metabolized-pseudocholinesterase (liver enzyme)

NORMAL MUSCLE Depolarization/Repolarization Ach=Acetylcholine =Acetycholinesterase Ach MOTOR Ach NEURON Ach Ach Myoneural junction Motor End plate MUSCLE CELL Nicotinic cholinergic receptors
cholinesterase")
DEPOLARIZING N-M BLOCKER Ach=Acetylcholinesterase Sx=Succinylcholine Ach Sx Ach MOTOR NEURON Sx Ach = Pseudo(plasma)cholinesterase Sx MUSCLE CELL

PSEUDOCHOLINESTERASE DEFICIENCY n n n n Atypical/deficient occurs in 1: 2800 people n Genetic n Malnutrition/liver disorders Paralyzed for several hours or more Requires ventilatory support! Feels pain! Hears everything! Be frightened! Will need education! May develop post traumatic distress symptoms!

INTRAOP INTUBATION INCISION

ANESTHESIA MAINTENANCE AGENTS n Inhalation gases n Are respiratory depressants n Affect CV & renal systems n Cause uterine relaxation n May cause shivering n Cause vasodilation n Increase cerebral blood flow n May be used prior to intubation for kids- “breathing down”

STAGES OF ANESTHESIA n Stage I-Analgesia=sleepiness n Stage II-Delirium=involuntary activity, nystagmus, breath holding, BP n Stage III-Surgical Anesthesia=Slow regular breathing, areflexia, pupils dilated and fixed n n 4 planes Stage IV-Medullary Paralysis=Death Awaken in reverse order

INHALED AGENTS n Nitrous oxide n n n Light anesthesia-amnesia, fast onset-offset “Carrier gas” Increases PONV Administered with O 2 Diffusion hypoxemia Sevoflurane (Ultane) n Fast onset and ultra fast offset n Smooth onset and emergence n Minimal airway irritation-mask inductions n Does not sensitize the heart to catecholamines n Strong vasodilator n Does not depress liver or kidney functions
 n Very fast induction and recovery n Elimination mostly")
INHALED AGENTS n Desflurane (Suprane) n Very fast induction and recovery n Elimination mostly via lungs n Pungent n Increased delirium n Strong vasodilator n May induce breath-holding n Isoflurane (Forane) n Smooth onset n Fast offset n Elimination mostly via lungs n Potentiates n-m blockers
 n Opioids n Sedatives n")
TIVA n Combination of IV agents n Propofol (Diprivan) n Opioids n Sedatives n Neuromuscular blockers n Oxygen/Nitrous Oxide

Incision Time

NON-DEPOLARIZING N-M BLOCKERS n Block muscle from being depolarized n Are profound muscle relaxants n Are curare related n Have variable lengths of action n Are metabolized slowly via liver, kidneys, or other processes n Are reversed by anticholinesterases

Non-Depolarizing N-M Blocker Ach=Acetylcholinesterase NDP=Non-depolarizing agent Ach P ND NDP N D P Ach MOTOR NEURON Ach Ach ND PP ND P MUSCLE CELL

N-M BLOCKERS n Selected based on: n n n Length of action CV /ICP and other side effects (histamine release, ICP, IOP) Metabolism-renal, hepatic, biliary, Hofmann elimination, pseudocholinesterase
-gold standard; histamine n Vecuronium (Norcuron)-corticosteroids may prolong paralysis;")
NON-DEPOLARIZING NM BLOCKERS n D-Tubocurarine (Curare)-gold standard; histamine n Vecuronium (Norcuron)-corticosteroids may prolong paralysis; no histamine-good for COPD/CV patients n Atracurium (Tracrium)-histaminic effects (flushing, bronchospasm, hypotension); p. H 3. 5=phlebitis; Hofmann elimination
-no histamine; Hofmann elimination primarily n Mivacurium (Mivacron)-short acting;")
NON-DEPOLARIZING NM BLOCKERS n Cisatracurium (Nimbex)-no histamine; Hofmann elimination primarily n Mivacurium (Mivacron)-short acting; plasma cholinesterase metabolism n Rocuronium (Zemuron)-fast onset (60 sec); no histamine/CV effect minimal n Pancuronium (Pavulon)- 5 times more potent than curare; little histamine; renal elimination

REVERSAL AGENTS for Non-Depolarizing N-M Blockers Ach=Acetylcholinesterase NDP=Non-depolarizing agent Anticholinesterase P NDPNDP = ND N D P Ach MOTOR NEURON Ach Ach ND N P MUSCLE CELL
 n n Onset 6 -8 minutes Lasts")
REVERSAL AGENTS ANTICHOLINESTERASE MEDS n Neostigmine (Prostigmin) n n Onset 6 -8 minutes Lasts 60 minutes May be used with glycopyrrolate Edrophonium (Tensilon) n n n Onset 2 -4 minutes Lasts 60 minutes May be used with atropine

ANTICHOLINESTERASE MEDS n n n Reverse neuromuscular blockade by destroying acetylcholinesterase Cause n Bradycardia n Hypotension n Salivation n Bronchoconstriction Must be used with anticholinergic drugs
 n Slower onset and change in HR")
ANTICHOLINERGICS Prevent anticholinesterase-induced bradycardia n Glycopyrrulate (Robinul) n Slower onset and change in HR n Does not cross BB barrier n Atropine n Faster onset and change in HR n Lasts 40 minutes
 inactivates")
WHAT’S NEW? ? n Selective relaxant binding agents n n n Sugammadex (Bridion) inactivates Rocuronium & Vercuronium As of 12/15/15 it is available; has been used in other countries Adverse events: Anaphylaxis n Severe bradycardia soon after injection (use Atropine) n Nausea/vomiting, low blood pressure, pain, headache n May reduce contraceptive effectiveness-advise patient! n

OPIOIDS n Block stress responses during surgery n Bind with receptors in the brain and spinal cord n Produce respiratory and CV depression n Must maintain blood level n Reversed by naloxone (Narcan)
 n")
OPIOIDS n Morphine n n n Gold standard High histamine release Fentanyl (Sublimaze) n n n 100 X more potent Shorter acting No histamine release
-more potent n Sufentanil (Sufenta)-short duration n Remifentanil")
OPIOIDS n Fentanyl Cousins n Alfentanil (Alfenta)-more potent n Sufentanil (Sufenta)-short duration n Remifentanil (Ultiva)-ultra short

OTHER INTRAOP MEDS n n Vasoactive meds Cardiac meds Antibiotics Insulin Anything the patient needs

WAKE UP TIME

POSTOPERATIVE MEDS-PACU n n n Oxygen Opioids Anti-emetics Sedatives Antibiotics Vasoactive medications
 n Shorter duration than morphine n Causes rashes n Meperidine")
OPIOIDS n Hydromorphone (Dilaudid) n Shorter duration than morphine n Causes rashes n Meperidine (Demerol) n Removed from many formularies n Produces metabolites that can cause seizures and CNS excitation n Used for shivering n Stimulates vomiting
 n Inhibit prostaglandin synthesis by blocking COX I and COX")
NSAIDS n Ketoralac (Toradol) n Inhibit prostaglandin synthesis by blocking COX I and COX II enzymes n Prostaglandins activate nerve fibers that transmit pain n Anti-inflammatory n Inhibit platelet function-COX 1 inhibition n Reduces amounts of opioids n Problems: increased bleeding, GI problems, kidney damage (COX I effects)

MORE MEDS! n n IV Ibuprofen-Caldolor® IV acetaminophen-Ofirmev
 n n Titrate to effect May cause non-cardiogenic")
OPIOID REVERSAL AGENT n Naloxone (Narcan) n n Titrate to effect May cause non-cardiogenic pulmonary edema if administered rapidly Lasts 1 -4 hours Watch for resedation for 2 hours
 n n n Titrate to effect Lasts 30")
BENZODIAZEPINE REVERSAL AGENT n Romazicon (Flumazenil) n n n Titrate to effect Lasts 30 -60 minutes Watch for resedation

CONDITIONS THAT AFFECT MEDICATIONS n Medication properties n Solubility-stored in fat n Methods of metabolism and excretion n Onset time n Peak effect time n Duration n Ability to cross BB barrier

CONDITIONS THAT AFFECT MEDICATIONS n Medical condition of the patient n Renal/liver problems n CV status n Respiratory status n Obesity/fat content n Age n Thermia regulation ability

THE GOAL! To see our patients LIVE!!
- Slides: 95