Integrated Management of Neonatal and Childhood Illness DR


























- Slides: 42
Integrated Management of Neonatal and Childhood Illness DR. ARVIND GARG
The Inequities of Child Health • Every year more than 10 million children die in developing countries before they reach their fifth birthday • 7 in 10 deaths are due to acute respiratory infections, diarrhoea, malaria, measles and malnutrition • 3 in 4 episodes of childhood illness are caused by one of these five conditions • The global burden of disease indicate that these conditions will continue to be major contributors to child deaths in the year 2020, unless significantly greater efforts are made to control them
Distribution of 10. 5 million deaths among children less than 5 years old in all developing countries, 1999 • 9 out of 10 deaths occur in 6 countries– Bangladesh – Bhutan – India – Indonesia – Myanmar – Nepal
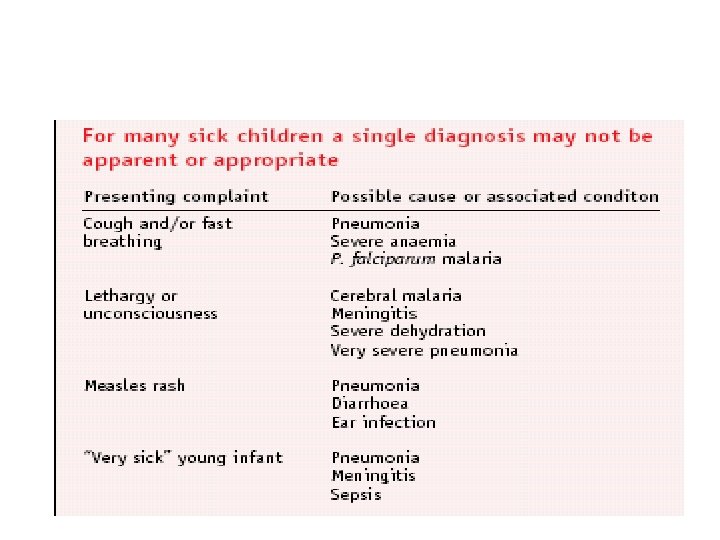
Rationale for an Integrated Evidence. Based Syndromic Approach to Case. Management • Overlapping signs and symptoms • Single diagnosis is not possible or appropriate • Improvements in child health are not necessarily dependent on the use of sophisticated and expensive technologies • Careful and systemic assessment of common symptoms and well-selected specific clinical signs provide sufficient information to guide rational and effective actions
Key elements
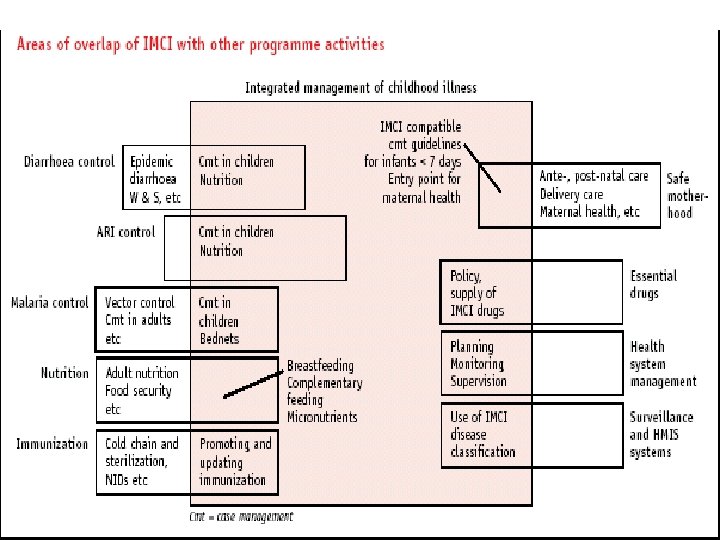
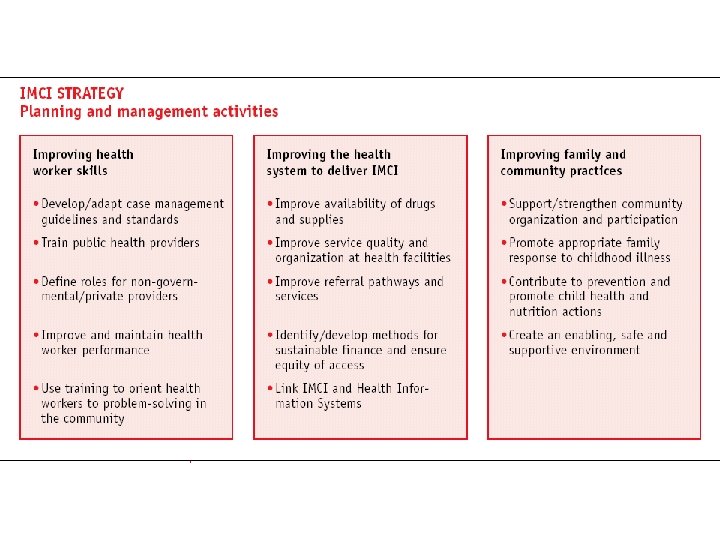
Components of Integrated approach • Improvement in case management skills of health staff through locally-adapted guidelines • Improvements in overall health system • Improvements in family and community health care practices
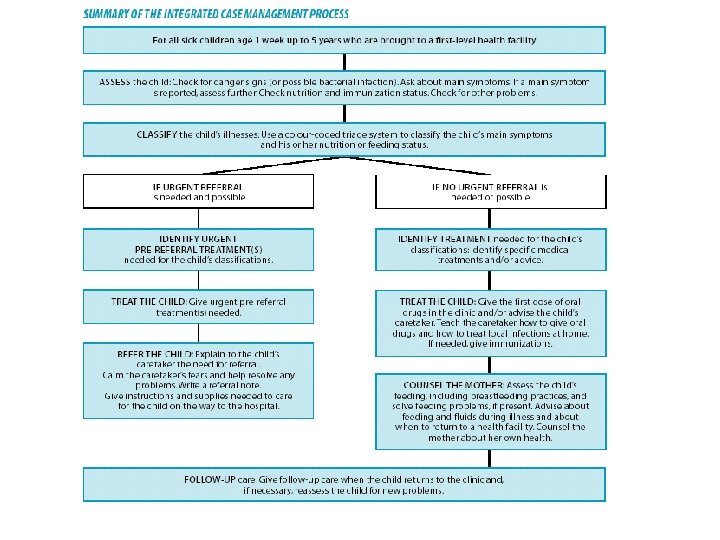
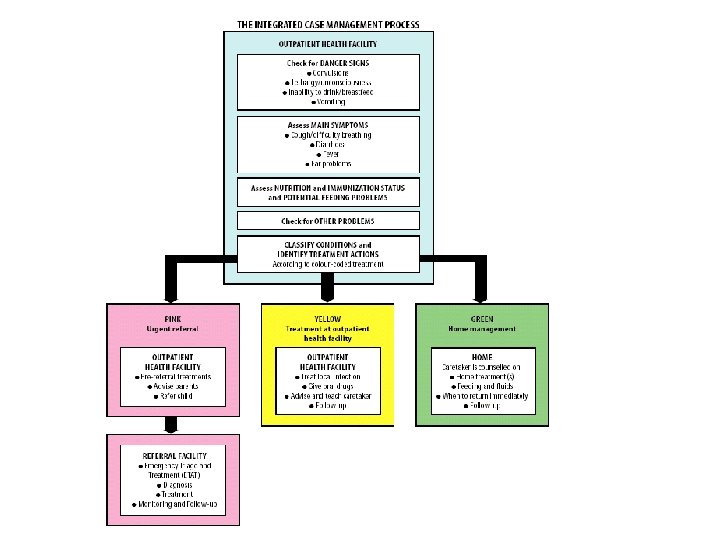
Assess and Classify
Identify treatment
Treat the child
Counsel the mother
Give follow up care
Young Infants age upto 2 months • • Not used for well infant brought for immunization Injury Burn Care of new born at birth • Greet the mother • Ask the mother what the young infant’s problems are • Determine if this is an initial or follow up visit • Use the young infant recording form
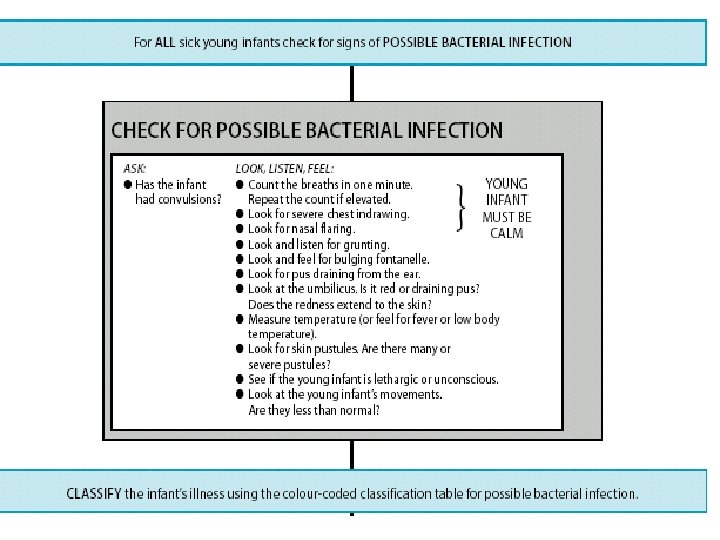
Checking for Possible serious bacterial infection/ jaundice
Jaundice/ Low body temperature • Yellow palms and soles or • Age <24 hours • Age 14 days or more • Severe Jaundice • Palms and soles not yellow • Jaundice • Temperature between 35. 5 -36. 4°C • Low body temperature
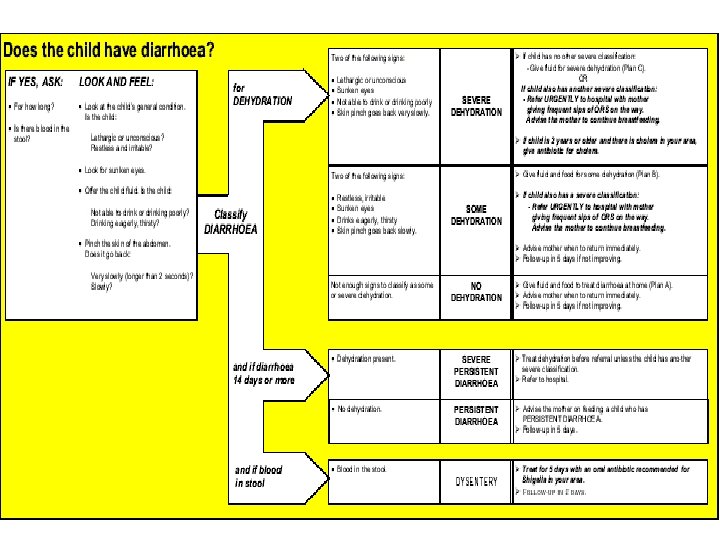
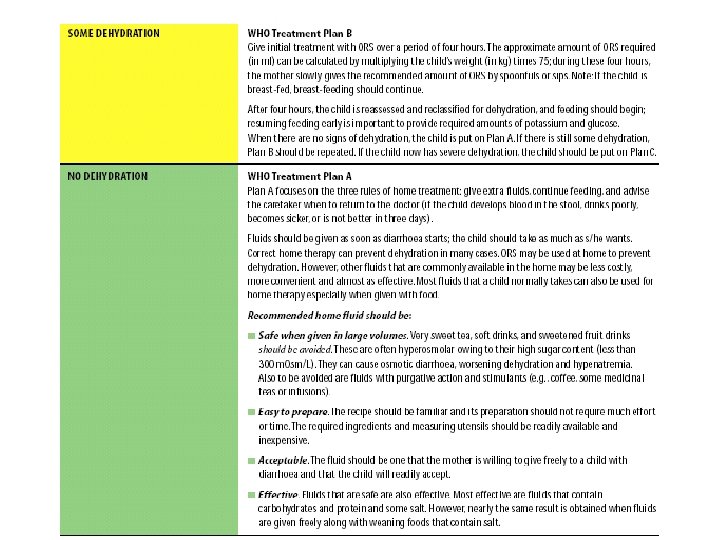
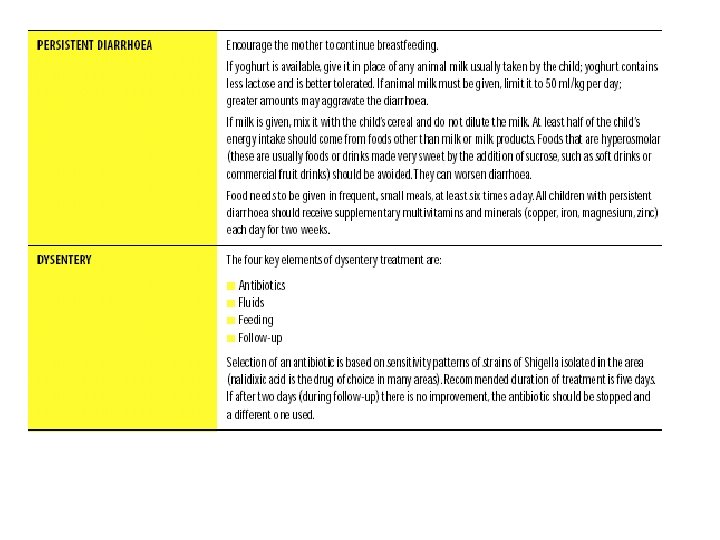
Diarrhoea
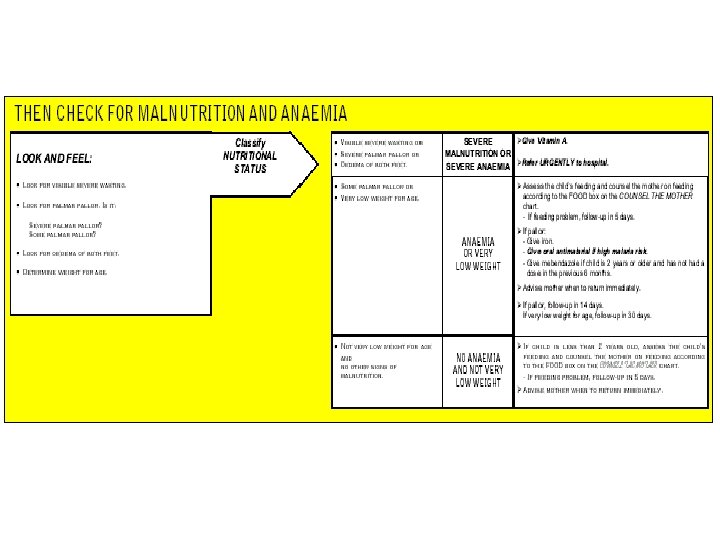
Feeding problem & Malnutrition • Not able to feed. Possible serious Bacterial Infection or severe malnutrition • Feeding Problem or Low weight • No Feeding Problem
Treatment of Sick Young Infants Urgent pre-referral treatments • Convulsions • possible serious bacterial infection • &/or severe dehydration or some dehydration with low weight • &/or severe persistent diarrhoea/ dysentry with low weight • &/or not able to feedpossible serious bacterial infection or severe malnutrition • Severe dehydration • For all infants before referral: - prevent low blood sugar -warm young infant • Diazepam (0. 2 mg/kg) • Phenobarbitone (20 mg/kg)<2 weeks of age • First dose of antibiotic • gentamicin (5 mg/kg)+ampicillin (100 mg/kg), or ceftriaxone (100 mg/kg) or cefotaxime (50 mg/kg) • Plan C
Treatment in the outpatient clinic for sick young infants age up to 2 months • Local bacterial infection • Some deydration (without low weight) • No dehydration • Feeding problem or low weight • Oral antibiotic • Plan B • Plan. A • Give feeding advice
Counselling a mother or caretaker • • Ask and Listen Praise Advice Check Essential elements • • Teach how to give oral drugs Teach how to treat local infection Teach how to manage breast or nipple problem Teach correct positioning and attachment for breastfeeding Counsel on other feeding problems Advise when to return Counsel the mother about her own health
Advise when to return • Return immediately if - breastfeeding or drinking poorly - becomes sicker - develops a fever or feels cold to touch - fast breathing - difficult breathing - yellow palms and soles (if jaundice present) -diarrhoea with blood in stools • Return for follow up not later than- local bacterial infection, jaundice, diarrhoea, any feeding problem, thrush- 2 days -low weight for age-14 days -
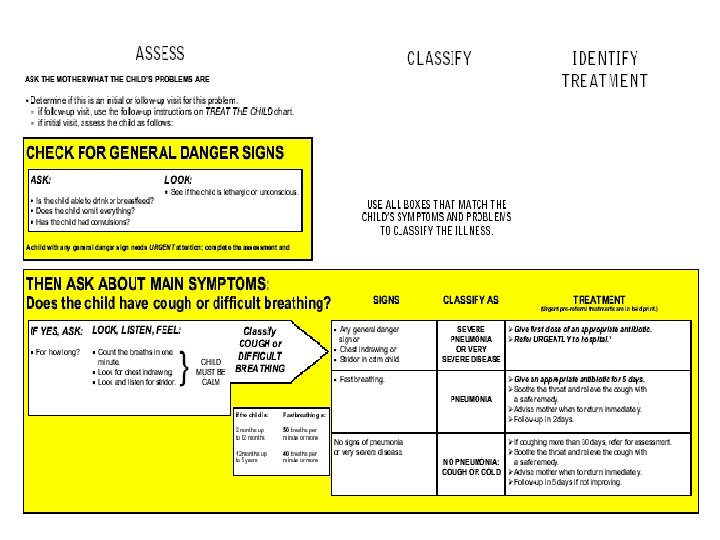
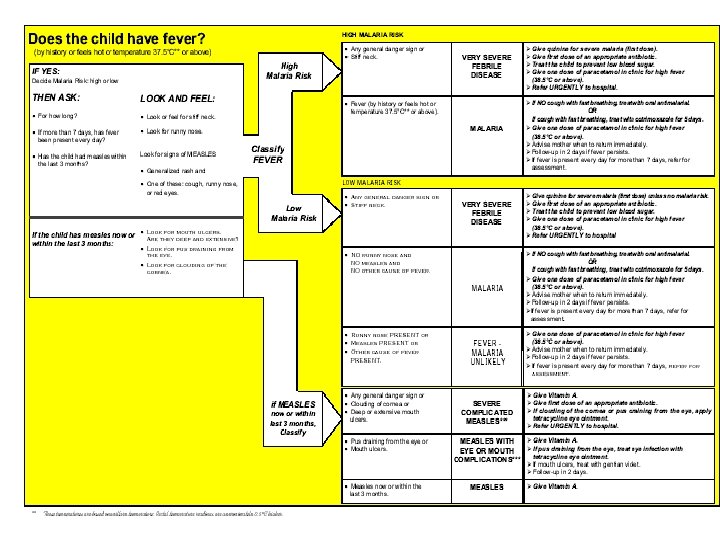
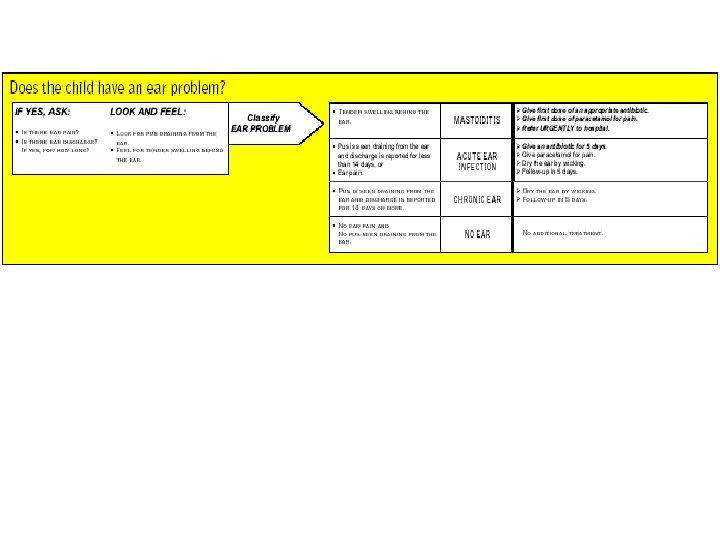
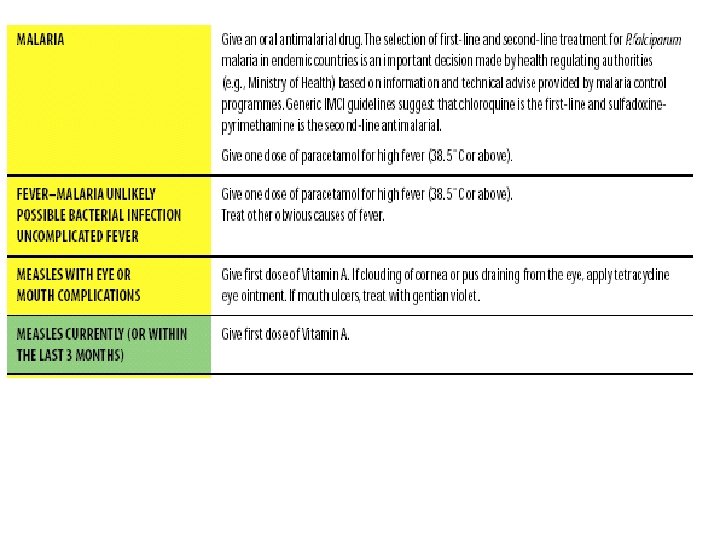
Outpatient management of children age 2 months up to 5 years
Urgent pre-referral treatment for children age 2 months up to 5 years
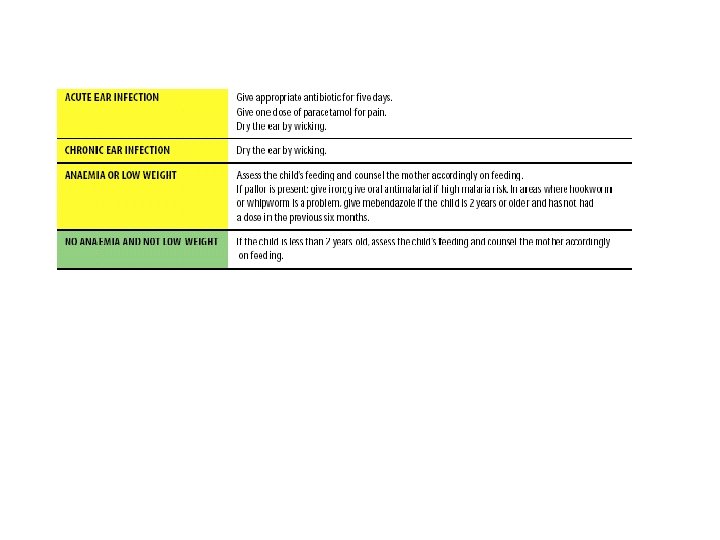
Treatment in outpatient facility
Advise to return immediately
For Follow up
Comments • promotes accurate identification of childhood illnesses in outpatient settings • ensures appropriate combined treatment of all major illnesses • strengthens the counselling of caretakers and the provision of preventive services • speeds up the referral of severely ill children • improve the quality of care of sick children at the referral level • In the home setting, it promotes appropriate careseeking behaviours, improved nutrition and preventive care, and the correct implementation of prescribed care. • cost-effective • Improves equity • has the potential to make a major contribution to health system