IN THE NAME OF GOD ANATOMY OF THE




 innervates the lateral rectus muscle cranial nerve IV (trochlear)")

































- Slides: 43
IN THE NAME OF GOD
ANATOMY OF THE EXTRAOCULAR MUSCLES MOHAMMAD REZA AKHLAGHI
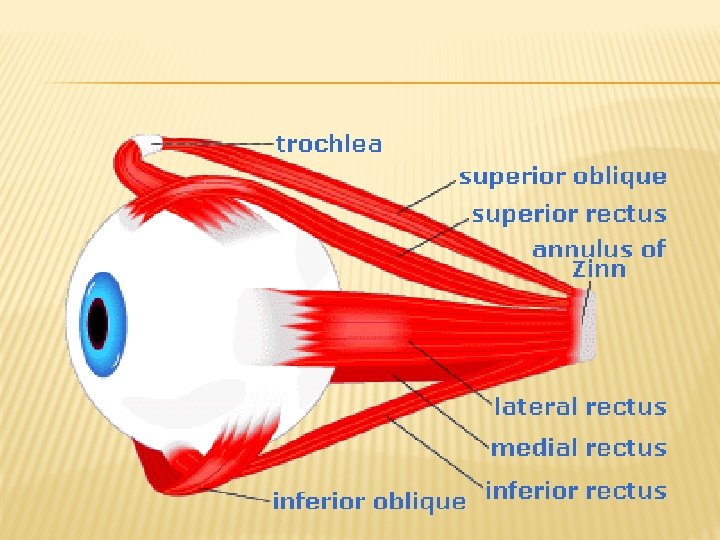
EXTRAOCULAR MUSCLES There are 7 extraocular muscles: � 4 rectus muscles, � 2 oblique muscles � levator palpebrae superioris muscle.
EXTRAOCULAR MUSCLES
INNERVATION Cranial nerve VI (abducens) innervates the lateral rectus muscle cranial nerve IV (trochlear) innervates the superior oblique muscle cranial nerve III has an upper and a lower division: innervates the levator palpebrae, superior rectus, medial rectus, inferior rectus, and inferior oblique muscles.
EYE POSITION & MUSCLE ACTIONS primary position The primary action is the major effect of a muscle, when the muscle contracts while the eye is in primary position. The secondary and tertiary actions: of a muscle are the additional effects on the position of the eye in primary position
RANGE OF ACTION � The globe usually can be moved about 50° in each direction from primary position. � Under normal viewing circumstances, the eyes move only about 15°-20° from primary position before head movement
ANNULUS OF ZINN A cone-shaped structure, behind the eyeball, composed of five extraocular muscles (medial rectus, lateral rectus, superior rectus, inferior rectus, and superior oblique), within which runs the optic nerve (cranial nerve II), the ophthalmic artery, and the ophthalmic vein
EXTRAOCULAR MUSCLES
MEDIAL RECTUS � Origin: annulus of zinn � Insertion: medially, in hori meri, 5. 5 mm from limbus � Length: 40 mm L, 10 mm W, 4 mm T � Direction: 90 o � Innervation: lower CN III � Blood supply: Inf. Mus. Branch Of Oph. A. � Action: addu
MEDIAL RECTUS
LATERAL RECTUS � Origin: annulus of zinn � Insertion: laterally, in horizontal meridian, 6. 9 mm from limbus � Length: 40 mm L, 9 mm W, 8 mm T � Direction: 90 o � Innervation: CN VI � Blood supply: Inf. Mus. Branch Of Oph. A. � Action: abd
LATERAL RECTUS
INFERIOR RECTUS Origin: annulus of zinn Insertion: inferiorly, in ver. Mer. 6. 5 mm from limbus Length: 40 mm L, 10 mm W, 5. 5 mm T Direction: 23 o Innervation: lower CN III Action: Dep. Ext, Add,
INFERIOR RECTUS
SUPERIOR RECTUS Origin: annulus of zinn Insertion: superiorly, in ver. Mer. 7. 7 mm from limbus Length: 40 mm L, 10 mm W, 5. 5 mm T Direction: 23 o Innervation: upper CN III Action: Dep. Ext, Add,
SUPERIOR RECTUS
SUPERIOR OBLIQUE Origin: superior of annulus of zinn (func. At trochlea Insertion: post. to equator in suprotemp. Length: 32 mm L, 6 mm W, 25 mm T Direction: 51 o Innervation: CN IV Action: Int, Dep, Abd,
SUPERIOR OBLIQUE
INFERIOR OBLIQUE Origin: behind of lacrimal fossa Insertion: post. to equator in macular area. Length: 37 mm L, 10 mm W, 1 mm T Direction: 51 o Innervation: lower CN III Action: Ext, Elev, Abd,
INFERIOR OBLIQUE
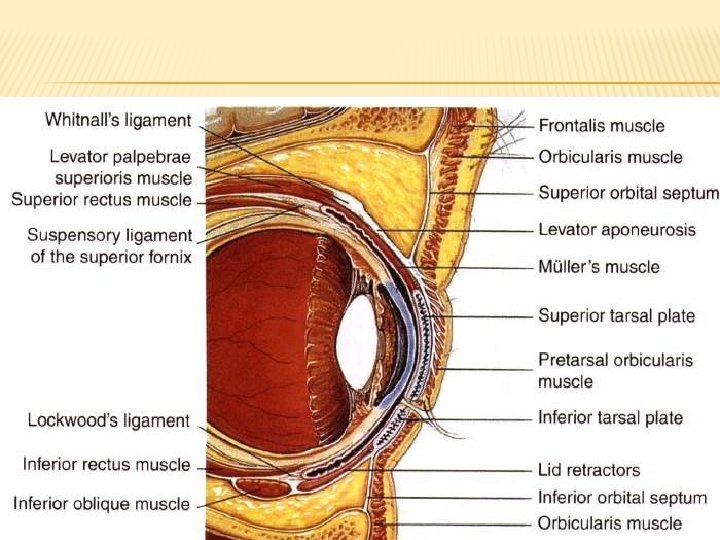
LEVATOR PALPEBRAE SUPERIORIS Origin: above of annulus of zinn Insertion: above and anterior surface of tarsus. Innervation: upper CN III Action: eyelid elevation
ADDUCTOR MUSCLES
ABDUCTORS
ELEVATORS
DEPRESORS
INTERNAL ROTATORS
EXTERNAL ROTATORS
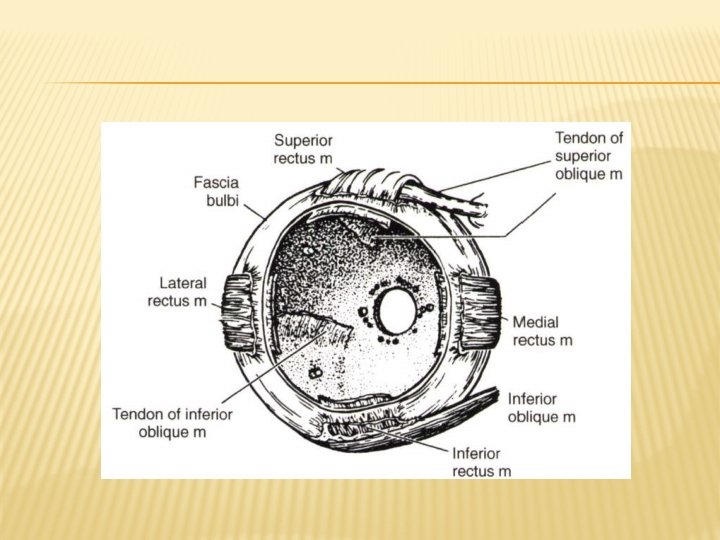
INSERTION RELATIONSHIPS OF THE RECTUS MUSCLES Spiral of Tillaux
MUSCLE CONE The muscle cone lies posterior to the equator. It consists of the extraocular muscles, the extraocular muscle sheaths, and the intermuscular membrane. The muscle cone extends posteriorly to the annulus of Zinn at the orbital apex
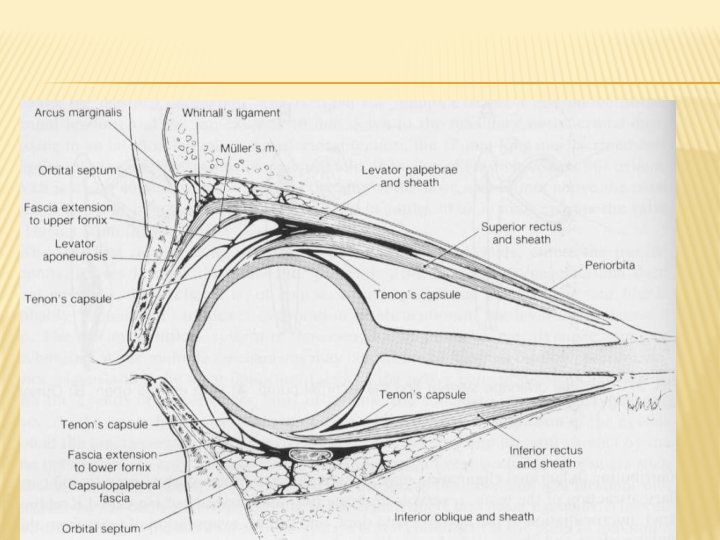
TENON'S CAPSULE Is the bulk of the orbital fascial system Forms the envelope within which the eyeball moves Fuses posteriorly with the optic nerve sheath and anteriorly with the intermuscular septum Posterior portion is thin and flexible Posterior to the equator, it is thick and tough, suspending the globe to the periorbital tissues
INTERMUSCULAR SEPTUM �a membrane that spans between rectus muscles and fuses with the conjunctiva 3 mm posterior to the limbus. � Posterior to the globe, it separates the intraconal fat pads from the extraconal fat pads. � Numerous extensions from all the extraocular muscle sheaths attach to the orbit and help support the globe.
ANATOMICAL CONSIDERATIONS DURING SURGERY Damaging of nerves during anterior surgery An instrument thrust more than 26 mm posterior to the rectus muscle's insertion may cause injury to the nerve. The nerve supplying the inferior oblique muscle enters the lateral portion of the muscle, where it crosses the inferior rectus muscle; the nerve can be damaged by surgery in this area. Cranial nerve IV would not be affected by a retrobulbar block.
CONT. The intermuscular septum connections, especially between rectus muscles and oblique muscles, can help locate a lost muscle during surgery. Extensive intermuscular septum dissections are not necessary for rectus recession surgery. During resection surgery, the intermuscular septum connections should be severed
The blood supply to the extraocular muscles provides almost all of the temporal half of the anterior segment circulation and the majority of the nasal half of the anterior segment circulation. Therefore, simultaneous surgery on 3 rectus muscles may induce anterior segment ischemia, particularly in older patients.
The inferior rectus muscle is distinctly bound to the lower eyelid by the fascial extension from its sheath
The sclera is thinnest just posterior to the 4 rectus muscle insertions. This area is the site for most muscle surgery, especially for recession procedures. Therefore, scleral perforation is always a risk during eye muscle surgery.