Herpes zoster VZV was in latent state in
 after the")


 Chronic disease › Diabetes mellitus, coronary heart")


 1. 3 cases/1, 000 persons")


 face(V,")

 Pain which appears or persists after the cutaneous symptoms Pathogenesis › inflammatory")

 › Vesicular rash(pustule) : antiseptic wet dressing (hyaluronic")

 ›")


")

 + Skin eruption + virology")






 is")






- Slides: 39
Herpes zoster � VZV was in latent state in sensory ganglia (DRG) after the primary infection as chickenpox � Reactivation of the varicellar-zoster virus � Consequence of declining VZV-specific cellular immunity leading to herpes zoster ☞ neurocutaneous disease !
VZV : chickenpox & zoster Herpes simplex virus : type 1 & 2 � VZV & HSVs : subfamily alpha herpes virinae of the herpes virus group � Primary VZV infection (leading to to chickenpox nucleic acids of VZV)→ remain latent in sensory ganglia : lasts for several decades before VZV reactivation �
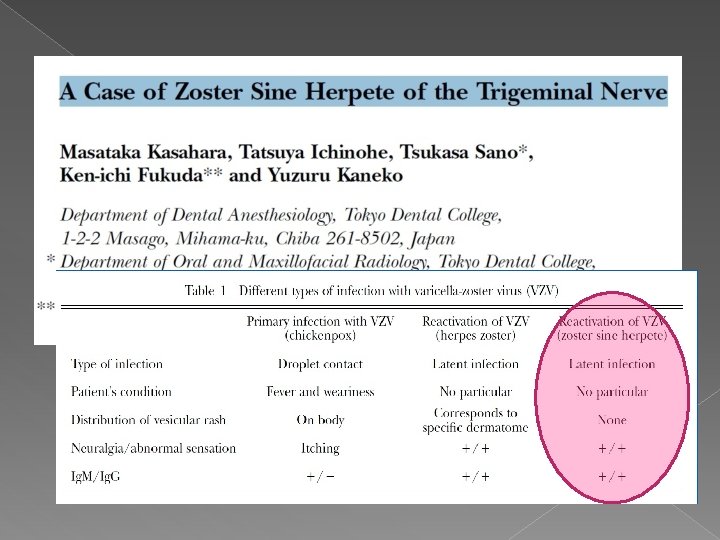
Reactivation & viral replication : necrosis & inflammation in the affected sensory ganglia → sensory nerves to the skin ☞ painful dermatomal rash(papulovesicular) & pustular skin lesions ☞ prodromal pain & paresthesia will appear After disappearance of both skin symptoms and acute pain, chronic zoster pain develps (>3 months) “Postherpetic Neuralgia(PHN)” zoster sine herpete : no visible cutaneous efflorescences despite acute & chronic zoster (very rare)
Risk factor Increasing age(>50 yrs, >>60 yrs) Chronic disease › Diabetes mellitus, coronary heart disease & depressions › Organ transplant recipients, tumor patients & HIV disease
Livengood JM. Curr Rev Pain 2000; 2: 7 -11 Psychosocial stress ↑ ☞ HZ & PHN ↑ Schmander et al. J Am Geriatr Soc. 1990; 38: 1188 -1194 Stressful life events and the status of spousal relationships between 101 individuals with HZ and 101 healthy controls ☞ negative lifeal. events results Immun. in participants with HZ Irwin et Brain Behav 2011’ 25: 759 -766 Depression may blunt the imune response and increase the risk and perhaps severity of HZ
Epidemiology VZV reactivation occurs in approximately 20% of seropositive individuals Normally, the VZV infection recurs only once in life Immunodeficient patients may develop zoster twice in the same dermatome : in very rare cases, even several times zoster may occur In contrast to HSV, The recurrence risk to develop zoster(shingles), increases with age(Meier and Strauss, 1992; Doerr and Rabenau, 1996)
3. 39 cases/1, 000 persons per year(in GB) 1. 3 cases/1, 000 persons per year(in USA) › 2~3 cases/1, 000 persons per year(40대말) › 5 cases/1, 000 persons per year(50대) › 6~7 cases/1, 000 persons per year(60 -70대) Leukemic children: 15%(Feldman et al. , 1973) BM transplant recipient: 30%(Locksley et al. , 1985) HIV: 20%(Veenstra et al. , 1995)
Cutaneous manifestation � Prodromal stage : 3 -5 days, General symptom : tiredness, weariness, mild fever & myalgia � skin rash, papule etc, not uniform � Burning pain, paresthesia, � Zoster sine herpete – dermatome dependent pain without rash � Zoster duplex is very rare: in very rare cases, several skin segments asymmetrically on both sides of the body(Vu et al. , 1999; Bloss et al. , 2001)
Within 12 -24 hours, grouped vesicle appear After 2 -4 days, vesicles become confluent On the 3 rd day, clouding the vesicles, dry out over 7 -12 days. In healthy patient, rash to crusts formation is 23 weeks Immunocompromised patient, lasting for months and repeated vesicular eruptions occur(Rustoven et al. , 1998)
Localization � May occur in any dermatome m/c site : thoracic segment(50 -56%) face(V, VII & VIII)(20%) cervical, lumbar & sacral segment (less frequent) › thoracic & other spinal DRG involvement �intercostal nerve block, epidural block, selective nerve root block, rhizotomy › cranial nerve involvement �trigeminal nerve(V 1, V 2 & V 3) �Facial nerve : Bell’s palsy(HSV, E-B virus >VZV) - no interventional Tx. Only medication �Ramsay – Hunt syndrome (Herpes zoster oticus)
Ramsay-hunt syndrome Medical treatment as well as Bell’s palsy involvement of Geniculate ganglion of VII Peripheral facial nerve palsy + erythematous versicular rash on ear or mouth Other symptom : tinnitus, hearing loss, N/V, vertigo & nystagmus
Postherpetic neuralgia(PHN) Pain which appears or persists after the cutaneous symptoms Pathogenesis › inflammatory nerve lesions with destruction of peripheral nerve structures or neurons in the sensory ganglia as well as modified signal processes in the central nervous system(Kost and Strauss, 1996)
Diagnosis � P/Ex : asymetrical dermatomal rash and grouped vesicles & various pain(hyperalgesia, allodynia, dysesthesia etc) � Lab. Diagnosis(virological assay) › VZV serology & PCR �VZV-Ig. G : in recurrent HSV-infections due to cross reactivity of epitopes �VZV-Ig. M, high titered Ig. A anti-VZV antibodies : reactivated VZV infection regardless whether lesions are visible or not
Treatment � Symptomatic therapy (regarding zoster) › Vesicular rash(pustule) : antiseptic wet dressing (hyaluronic acid gel + antibiotic-ointment) › Antiviral ointment: controversy(Gross, 1997) › Po medication �Antiviral agents : effectively treat zoster rash & inhibit the viral replication �Analgesics(acetaminophen, tramadol, ultracet etc) �Oral corticosteroids (only or combination c antiviral agents) – to decrease neural inflammation but no long-term benefit and no effect on PHN �Antihistamines
Antiviral agents � Acyclovir (800 mg 5 times daily for 7 days, 10 mg/kg IV q 8 hrs for 7 -10 days) › Accelerates healing and reduces associated pain › Not helpful reducing PHN(Peterslund, 1982. Bean, 1982) › S/E : headache, nausea, diarrhea and renal toxicity, disorientation, delirium, seizures, slurred speech � Valacyclovir (1, 000 mg 3 times daily for 7 days, valtrex) › › › Prodrug of acyclovir, oral bioavailabitiy(65%) More effective resolving PHN No nephrotoxicity or neurotoxicity, but in renal insufficiency, modified dosage
� Famicyclovir (500 mg 3 times a day for 7 days, famcivir, famvir) › More bioavailability(77%) › Decrease duration of PHN among elderly patients(Tying, 1995) � Indications for systemic antiviral therapy › Urgent indication � Zoster of any localization >50 yrs � Zoster in the head/neck area at any age � Severe zoster on the trunk/ on the extremities � Immunocompromized zoster � Zoster in patients c severe atopy & eczema › Relative indication � On the trunk/ extremities zoster <50 yrs
Therapy of neuralgia : step-by-step scheme � � Step 1 : non- steroidal analgesics (e. g paracetamol 1. 5~5 g/day) Step 2 : additional low-potency opioid analgesics (e. g tramadol 200~400 mg/day, codeine 120 mg/day) � Step 3 : in additin to a peripheral analgesic, administration of a high-potency central opioid (e. g oral morphine 30~360 mg/day, buprenorphine 1. 5~1. 6 mg/day) ##. In severe neuralgic pain, step 1 or 2 in combination with an anti-convulsants (carbamazepine 400 -1200 mg/day) Anticonvulsants reduce the lancinating pain, but not effective for continuous pain. Gabapentin(900 -2400 mg/day) or pregabalin(150~600 mg/day) Antidepressants (TCA, nortryptilline) or SNRI (Venlafaxine, cymbalta, effexor, milnacipran etc) -local therapy : capsaicin(diaxen), local anesthetic patch(lidotop) etc. ##. Pregnant woman (third trimester) : should not take NSAIDs like ibuprofen(Advil, Motrin, Nuprin etc)
Complications Acute cx. 2 dnary infection Zoster hemorrhagicus Zoster gangrenous Zoster generalisatus Chronic cx. Persisting zoster Scars Pigmentation(hypo/de) Granulomatous skin Pseudolymphoma psoriasis Nervous systems Eye Inner organs Encephalitis Meningitis Granulomatous arteritis Segmental pareses Facial palsy in zoster oticus Conjunvtivitis Episcleritis Uveitis Keratitis iridocyclitis Pneumonia Esophagitis Myocarditis Enterocolitis Pancreatitis PHN G-B syndrome Myelitis Motor neuropathy Abdomnial hernia Bladder dysfunction Keratitis Chorioretinitis Retrobulbar neuritis Vasculitis Optic n. atrophy arthritis
Resistance of VZV to antivirals Can become resistant to nucleoside analgues(Acyclovir, VCV, FCV etc) › d/t mutations in the thymidin kinase(TK) gene or mutations in the TK gene Treatment of choice › IV foscarnet, 3 times 40 mg or 2*50 mg/kg/Bwt/day(Breton et al. , 1998) › Alternative Tx. : IV cidofovir(safrin et al. , 1997)
Old age! PHN? Dementia? How manage? Total 84명 42명: PHN group(21명: systemic Tx. 21명: topical Tx) 42명: healthy volunteer 4 cognitive test – reaction time, semantic memory, decision making & visual memory
PHN Vs Radiculopathy DDx? History taking(onset, distribution, pain type) + Skin eruption + virology test ☞Antiviral or other medication or image w/u or intervention
50세 이상 Acute zoster 환자중 64명선정 Group 1 SGB block c 8 ml saline Group 2 SGB block c 0. 125% bupiva 6 ml+ 8 mg dexa total 8 ml 두군 모두 pregabalin 150 mg bid, acetaminophen prn. 일주일간 두번 SGB 시행 후, VAS initial visit, after 2, 3 and 6 mo. Check -> pain duration : group 2에서 통계상 의미 있을 정도로 짧아졌다. PHN incidence : 3, 6개월후에 발병률도 group 2에서 의미 있을 정도로 적어졌다 전체 pregabalin및 acetaminophen사용량도 group 2에서 현저히 감소
Peripheral nerve field stimulation Usage : intractable PHN, occipital neuralgia, shoulder pain , postherniorrhaphy site neuralgia & chronic LBP etc. USA FDA approved : equipment is yes, approach is not yet Newley modality for intractable neuropathic pain
A lack of nation-wide surveys on the current status of PHN tx. Retrospective chart review, 2011. Jan~Dec. in 11 teaching Hosp. 1, 414 patients review ↓ 1. Most common affected site : thoracic area - trigeminal area(15. 6%, V 1>V 2>V 3), lumbar (13. 8%), cervical(13. 1%), other (3%) 2. PHN Tx. Modality(mostly used) : anticonvulsants + interlaminar epidural block 3. Parenteral or topical : anticonvulsants(83. 8% ), NSAIDs, TCA, Tramadol(each other about 55%), Topical lidocaine(19. 1%), opioid(18. 4%), SSRI/SNRI(7. 7%), steroid(4. 4%), capsaicin cream(2. 1%) 4. Epidural block interval : 5 or more-weeks > 1자 5. Peripehral & cranial n. block interval : 0. 5~2 weeks 6. Before PHN treatment, observation period : median 1 month 7. Other Treatment : p. RF, heat RF, IV ketamin, IV multi-vitamin 8. Incidence of suspected zoster sine herpete : only 0. 1~0. 2%%
• Antiviral agents : dose-related adverse drug reaction? Neurotoxicity with delirium, tremor, confusion, hallucinations , coma • Typically occur within days of drug initiation and generally resolve with drug discontinuation • In older patient with chronic kidney disease ☞ to prevent systemic accumulation from reduced elimination ☞ not associated with an increased risk of adverse drug events.
Zoster vaccine � US FDA : recommend use of the vaccine for the aged over 60 (2006)(ZOSTAVAX ) � In Korea, commercial release in 2012 � Live attenuated vaccine R
Efficacy and clinical effectiveness › The vaccine strain of the zoster vaccine(ZOSTAVAX) is the same strain used for Varicella vaccine(VARIVAX) › In the Zostavax, vaccine strains are contained 14 times of Varixax › A Shingles prevention study on ZOSTAVAX (1998~2001 38, 546 persons, over 60 yrs) Herpes zoster incidence 51. 3% decreased, PHN incidence 66. 5% decreased & side effects are decreased preventive effect of HZ & PHN : gradually decreasing during the first year of vaccination, but maintained stably for at least three years Increased reaction (RCF and IFN-r ELISPOT) : maintained for 3 -6 years after vaccination
Recommendation of korean society of infectious disease � In 2012, KSID recommendation › Adults over 60 without contraindication › but the recommendation for adults at 50 ages through 59 was deferred. ( could not be verified ) › In chronic disease and immunocompromised, the risk of incidence of HZ increases but vaccination is not recommended under the specific age because the recommendation criteria were set by age
Licensure of VZV in the USA was a lengthy process largely because of concerns about warning immunity leading to possible (1) vaccine failure in older age groups when varicella can be more severe and/or (2) a subsequent enhanced risk for HZ. � Tseng et al(2012), in cohort study, � › HZ history patient를 2년간 재발 관찰, 재발율은 vaccination과는 무관하게 낮다. ☞ vaccination이 최근 HZ 병력 가진 사람에서는 반드시 필요하다고 할 수 없다.
Adverse reaction on vaccination � Major reaction rate : 1. 4% › Asthma attack and poly-myalgia rheumatic sx. � m/c reaction : reddness, pain, swelling, pruritis hematoma, headache › Slight & spontaneously recover When varicella-like eruption on vaccination, sensitive to VZV and virus can be spread ☞ do not contact. �
Future of Vaccination New inactivated vaccine › Very helpful in immunocompromised person
Varicella during pregnancy l l In the prevaccine era, the frequency of chickenpox during preg in the USA : 5(1 -20)cases/10, 000 pregnancy Varicella pregnant : 10~20% more high risk of developing VZV pneumonia than non pregnant Varicellar pneumonia is fatal. Mortality rate : over 40% l l Every suspected chicken pox pregnant women should be started immediately on oral acyclovir (esp, famciclovir or valacyclovir) within 72~96 hrs. In 1 st trimester primary VZV infection, not seem to increase the risk of spontaneous abortion In 1 st half trimester(13~20 wks), risk of the rare congenital varicella -> intrauterine fetal VZV infection ☞ varicellar embriopathy : limb atrophy, skin scar, CNS problem VZIG or acyclovir to its mother In 3 rd trimester, fetal infection can occur but the outcome is usually good with no associated birth defects -> increased risk for HZ during early infancy(infantile zoster)
� What are the complications of HZ in pregnancy? › PHN develops in about 20% of pregnant HZ › May Persist on 4 months after the initial rash › Less common in this case d/t pregnant women age under 40 years ago � What is the prognosis for HZ in pregnancy? › Most cases heal without a risk of serious complications or long-term problems � Can HZ in pregnancy be prevented? › Zostavax : reduces in the incidence about 50% �Cannat be taken by pregnant women �Should wait at least 3 months before attempting pregnancy