Evaluation of the Thoracic Spine ATTR 322 Krzyzanowicz



















 ◦ Sternum projects forward and downward like")

; T 7= inferior")
")
 ◦ Flexion- bend down")
 � Manual ◦ ◦ muscle test: Pectoralis major/minor Serratus anterior Rectus")






; could be stress fracture over time")
 �")


 ◦ Muscular membrane; separates thoracic and abdominal cavity; creates")







, primary function")












 ◦")


 ◦ Thoracic-try to rule out life")

- Slides: 66
Evaluation of the Thoracic Spine ATTR 322 Krzyzanowicz- Spring ‘ 13
Objectives � Understand bony and soft tissue anatomy of the thoracic spine � Understand movement relationships of the thoracic spine � Describe common injuries to the thoracic spine, abdomen, heart and lungs � Demonstrate the proper evaluation of the thoracic spine to include ◦ Palpation, special tests ◦ Differentiate between life-threatening emergencies and non-life threatening emergencies � Utilize EBP principles' in evaluation techniques
Orthopedic Evaluation of the Thoracic Spine
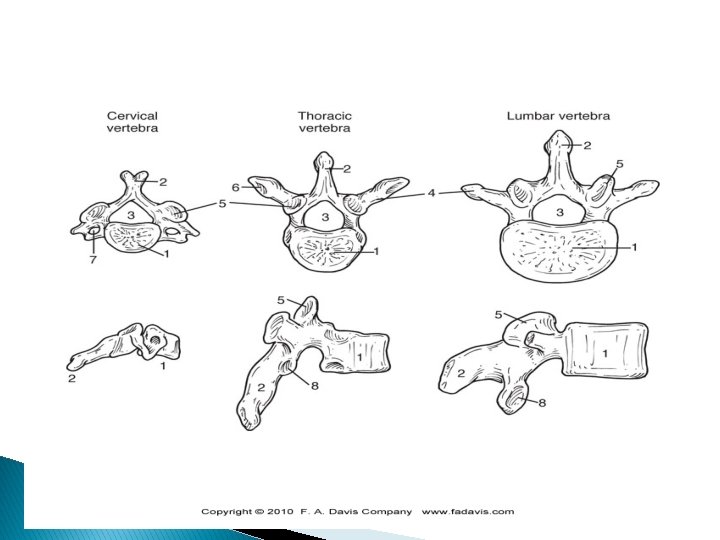
Thoracic Spine � Spinal column is divided into 4 segments, cervical and thoracic are the two for this class � Thoracic spine (T 1 -T 12) ◦ Provides great protection of spinal cord but limited ROM �Protects heart and lungs �Injury to anterior thoracic spine can range from mundane to fatal �Progressive symptoms leading to death �Need to know signs and symptoms!
Clinical Anatomy � Sternum ◦ Manubrium ◦ Body ◦ Xiphoid process � True ribs ◦ Upper 7, articulate with sternum (costal cartilage) � False ribs ◦ Ribs 8 -10; conjoined costal cartilage � Floating ribs ◦ 11 -12, do not have an articulation
Joints of the Thoracic Spine � Costovertebral joints ◦ Located between the ribs and vertebral bodies � 24 of these joints �Ribs 1, 10, 11 and 12 articulate with a single vertebra �Ribs 2 -9 articulate with the two adjacent vertebrae and intervening intervertebral disc � Costotransverse joints ◦ Found between the ribs and transverse processes of the vertebra for ribs 1 -10
Joints of the Thoracic Spine � Costochondral joints ◦ Between ribs and costal cartilage ◦ Joints 2 -6 are synovial, 1 st is not ◦ Where a rib articulates with an adjacent rib or costal cartilage (ribs 5 -9) a synovial joint exists ◦ What does this all mean?
Facet Joints � Apophyseal of facet joints ◦ T 2 -T 11 facets face down, forward and slightly medial �This enables slight rotation in the thoracic spine � Thoracic spine ◦ 60 degree angle ◦ Superior facets face posterior ◦ Inferior facets face anterior
Superior Facet
Rib Motion During Breathing � If a rib or group of ribs stops moving relative to other ribs during inhalation ◦ Classified as a depressed rib or an inhalation restriction � If �Top rib is key to mobilize a rib or group of ribs stops moving relative to other ribs during exhalation ◦ Classified as an elevated rib or an exhalation restriction �Bottom rib is key to mobilize
Rib Motion During Breathing � Ribs 1 -7 � Ribs 8 -10 � Ribs 10 -12 ◦ Pump handle motion ◦ Bucket handle ◦ Caliper
Rib pump handle and bucket handle motion
History of present condition � Location of pain ◦ Ribs, thoracic spine? P! with extension? Feel like it has to pop? �Referred pain- Kehr’s sign � MOI ◦ Direct blow (usually for thoracic spine) or facet � Onset ◦ Gradual (internal bleeding) vs. sudden � Complaints ◦ Syncope, palpitations, chest pain, respiratory issues?
History of present condition � Patients age? ◦ Scoliosis/anatomical diseases � Pain with coughing, sneezing or straining? ◦ Valsava’s maneuver � What makes it better/worse? � Posture bother you? � Referred pain?
Types of Pain Descriptors Possible Causes of Pain Sharp Musculoskeletal trauma Pinching Facet dysfunction Stretching Muscular hypertonicity Deep aching Myofascial P!, kidney (renal) Stabbing Costovertebral or visceral P! associated w/diet Visceral (gallbladder? ) Deep, boring Bone Crushing Pulmonary P!
Inspection � Musculoskeletal ◦ ◦ ◦ assessment Spinal/pelvic alignment/leg length Thoracic curve- kyphotic? Atrophy- lats, rhomboids, traps? Foot posture- pronation or supination Knee posture- valgus, varus, recurvatum Hip posture- anteversion (pigeon toed), retroversion (duck footed)
Kyphosis � Rounded thoracic spine ◦ Round back- usually soft tissue ◦ Hump back- usually structural ◦ Flat back- decreased pelvic angle, thoracic spine remains mobile ◦ Dowager’s hump- postmenopausal osteoporosis
Scoliosis � Deformity in which there are one or more lateral curves of the lumbar or thoracic spine or combination of spinal areas ◦ Nonstructural- poor posture, nerve root irritation, inflammation in the spin area, leg length discrepancy or hip contracture can cause this ◦ Structural- genetic, idiopathic or caused by congenital problems �Structural change in the bone
Scoliosis
Chest Deformities � Pigeon chest (pectus carinatum) ◦ Sternum projects forward and downward like the heel of a boot �Congenital, impair breathing � Funnel chest (pectus excavatum) ◦ Congenital deformity that results from the sternum’s being pushed posteriorly by an overgrowth of the ribs; may cause kyphosis � Barrel chest ◦ Sternum projects forward and upward
Chest Deformities
Orthopedic Palpation � Bony ◦ Spinous processes (T 1 -T 12); T 7= inferior angle of scapula ◦ Transverse processes (T 1 -T 12) ◦ Ribs ◦ Costovetebral junctions (spine) ◦ Costochondral junctions (anterior) ◦ Sternum-body, manubrium and xiphoid process
Orthopedic Palpation � Soft tissue ◦ Supraspinatus ligament ◦ Paraspinal muscles (spinalis, longissimus, iliocostalis) ◦ Trapezius ◦ Latissimus dorsi ◦ Rhomboids ◦ Pectoralis major/minor ◦ Serratus anterior ◦ Rectus abdominus ◦ External/internal obliques
Orthopedic ROM � Measure (using tape measurer or eyeball it) ◦ Flexion- bend down touch your toes (middle finger to floor) ◦ Extension- extend back (measure scapulae to floor) ◦ Lateral flexion- middle finger to floor ◦ Rotation- goniometer in center of skull, rotate with them
Muscle Testing (Strength) � Manual ◦ ◦ muscle test: Pectoralis major/minor Serratus anterior Rectus abdominus External obliques � What about spinal muscles?
Neurological � Sensory exam from T 1 to T 12 ◦ T 1 - medial forearm ◦ T 2 -T 12 coincide with the rib �T 2 -T 5 are only anteriorly �T 6 -T 12 are anterior and posterior � Can they feel you with sharp and dull? ◦ Is the feeling diminished? ◦ If so, what does that mean?
Special Tests for Orthopedic Evaluation � Kernig/Brudzinski Signs ◦ Could mean many things � Rib compression tests (ant/post and med/lat) ◦ r/o fx � Scoliosis flexion test � Slump test � Beevor’s sign � Quadrant test � Thoracic Outlet Tests ◦ Allen’s, Adson’s
Facet Joint Problems � Common in uppermost and lowermost thoracic segments ◦ Usually unilateral pain ◦ Feels a pinching sensation with extension �Feels like it has to pop �Feels like it is “stuck” ◦ MOI- poor mechanics (posture, muscle spasm/shortening) � Treatment ◦ Passive intervertebral movements ◦ Adjustment
Thoracic Sprain/Strain � MOI ◦ Heavy lifting or exertion � Signs ◦ ◦ and Symptoms P! localized to muscle or joint involved Rarely referred to another area Spasm in the muscle Tough to differentiate between sprain of ligament or strain of muscle (due to musculature) � Treatment ◦ Rest, gentle stretching, stim to break spasm �Heat or ice?
Costovertebral Dysfunction � MOI ◦ Usually in an awkward position and have a force (cough, sneeze, wrestling) � S&S ◦ Stabbing, focal P! over CV joint ◦ P! with deep inspiration, coughing, sneezing ◦ May radiate into anterior chest wall and to the side of the injury ◦ P! with thoracic movement � Tx ◦ Rest, ice
Costochondral Dysfunction � MOI ◦ Usually in an awkward position and have a force (cough, sneeze, wrestling) � S&S ◦ ◦ Heard/felt a pop Stabbing, focal P! over CC joint P! with deep inspiration, coughing, sneezing P! with thoracic movement � Tx ◦ Rest, ice
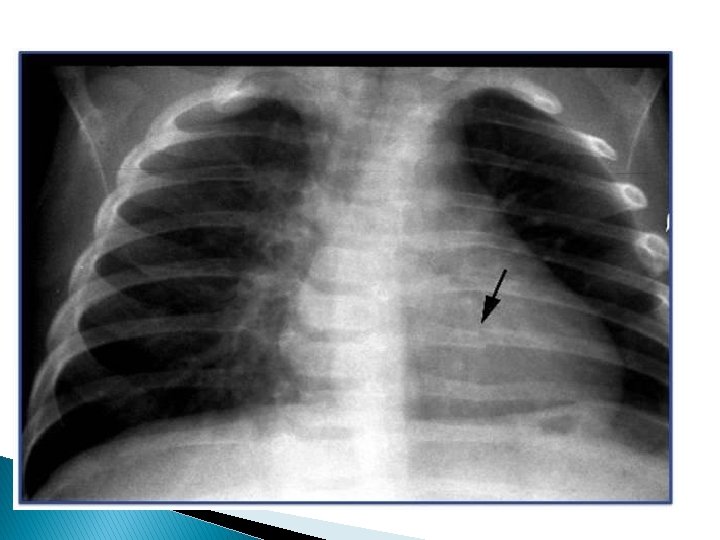
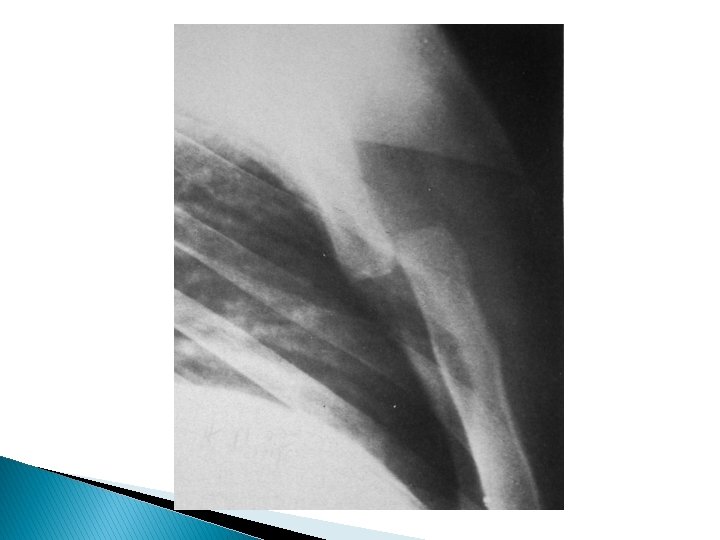
Rib Fracture � MOI ◦ Direct trauma (typically); could be stress fracture over time � S&S ◦ Sudden P!, difficulty breathing, pt. tender over the rib (deformity possible), crepitus, delayed ecchymosis, crepitus ◦ Rib compression test (a-p/ lat-med) � Tx ◦ Refer for x-ray ◦ r/o injury to lungs ◦ Watch and wait
Sternum Fracture � Can include any part of the sternum (manubrium, xiphoid process) � MOI ◦ Direct trauma, compression � S&S ◦ Sudden P!, difficulty breathing, sharp chest P!, rapid swelling, deformity, crepitus � Tx ◦ Refer for immediate x-ray
Solar Plexus Syndrome � “Wind � MOI knocked out” ◦ Direct trauma to solar plexus � S&S ◦ P!, can’t breathe, hysteria � Tx ◦ Calm patient down ◦ Deep breathes in through nose, out through mouth
General Medical Evaluation of the Abdomen
Clinical Anatomy � Diaphragm (inspiration) ◦ Muscular membrane; separates thoracic and abdominal cavity; creates a vacuum pulling air into lungs �Phrenic nerve � Intercostal muscles ◦ Intrinsic skeletal muscles air in inspiration; as do the scalene muscles- elevate 1 st and 2 nd rib �Sternocleidomastoid, trapezius, serratus anterior, pec major/minor and lat. dorsi all help with inspiration
Clinical Anatomy � Abdominal muscles aid in expiration ◦ Rectus abdominus, internal and external oblique and transverse abdominus �All flex and rotate lumbar and thoracic spine but also help expel air from lungs �Pressure gradient across diaphragm
Respiratory Tract � Trachea ◦ Connecting the larynx to the bronchioles then into each lung � Lungs ◦ Right lung has 3 lobes; left lung has 2 �Parietal pleura lines the thoracic wall �Visceral pleura surrounds the lungs; forms a pleural cavity between the two ◦ Exchange of gases occurs at the alveoli
Respiratory Tract
Cardiovascular Anatomy � Heart and major vessels lie within the mediastinum, b/t the lungs ◦ Heart divided into 4 chambers (table 15 -1 p. 567) ◦ Valves of the heart
Cardiovascular Anatomy � Heart anatomy ◦ Right atrium receives deoxygenated blood via superior and inferior vena cava �Passes through tricuspid valve ◦ Left atrium �Newly oxygenated blood via the pulmonary veins; passed through mitral valve
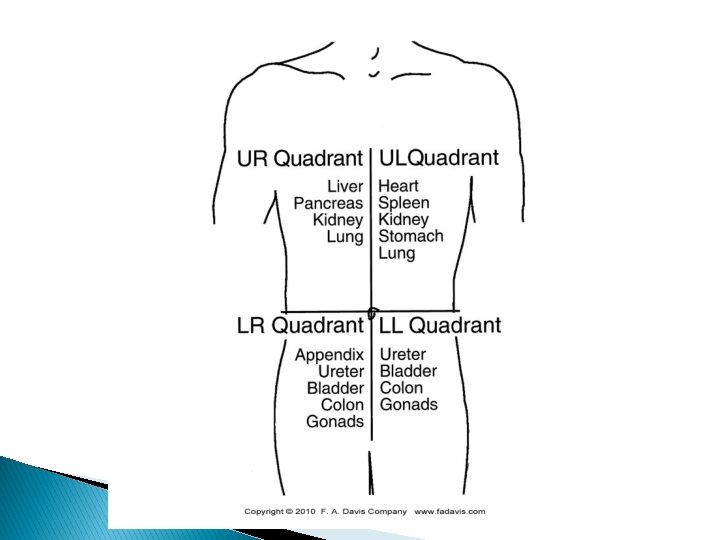
Digestive Tract � Esophagus ◦ Solids/liquids enter digestive tract through esophagus and enter the stomach � Liver ◦ Largest organ in the body, Upper Right quadrant; introduces bile (from gallbladder) to digest fats �What if your gallbladder is removed? Fats=what? ◦ Also stores glucose and filters toxins out of blood and produces mediators for blood clotting
Liver and Gallbladder
Lymphatic Organ � Spleen ◦ Upper left quadrant (9 -11 th ribs), primary function is to destroy blood cells during times of infection ◦ Mononucleosis �Engorged with blood, protrudes through ribs �Could cause spleen to be removed in ruptured �If spleen is removed, liver and bone marrow take over it’s functions
Urinary Tract � Kidneys ◦ Responsible for filtering toxins from blood, regulate body’s electrolyte levels ◦ Lie on each side of vertebral column (T 12 -L 3) �Right kidney slightly lower than left kidney �Unprotected by ribs increases chance of direct blow trauma
Reproductive Tract � Males ◦ Testes- produce sperm and testosterone �Commonly injured in athletics �Common place for cancer in the high school/college aged athlete � Females ◦ More commonly we see menstrual cycle dysfunction in the athlete �Female athlete triad
History � Past history important here ◦ Should be on physical; ask about paired organs, asthma � Family medical hx ◦ Cardiac abnormalities (hypertrophic cardiomyopathy) � Medication/drug use � General medical health ◦ Conditions such as asthma, Crohn’s disease, hypertension, etc
Inspection � Observe posture ◦ Leaning to one side? Flexing? – cramp or can’t breathe? � Sweating ◦ Typical of cardiac arrest � Throat ◦ Midline of cervical spine? If no- possible pneumothorax � Muscle tone ◦ Paraspinal muscles � Skin features ◦ Abrasions, contusions, bruising
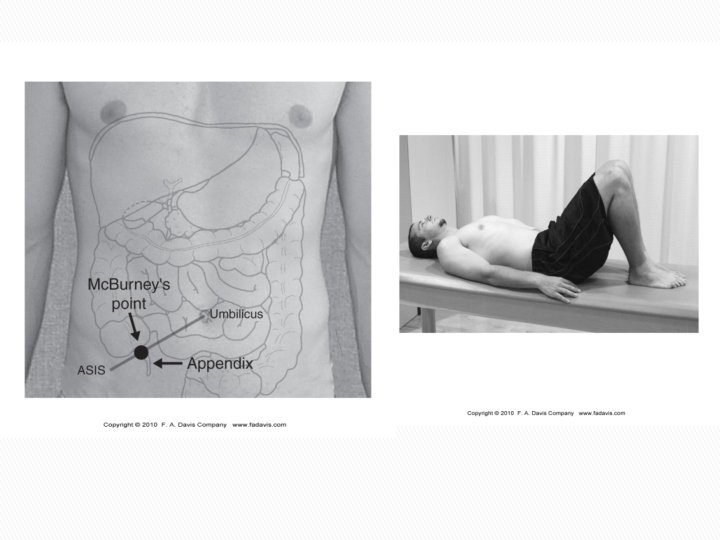
Non-Orthopedic Palpation � Organs ◦ Spleen �Palpate under left rib cage- have pt raise arms overhead ◦ Kidneys �“punch” thoracolumbar region on each side ◦ Mc. Burney’s Point �Located between ASIS and navel (appendicitis)
Palpation of Abdomen � Hook lying position ◦ Rigidity �Secondary to muscle guarding or blood accumulating in abdomen; internal injury likely ◦ Rebound tenderness �Pain increases after you remove your hands from the organ (common in appendcitis) ◦ Tissue density �Tapping or percussing over organs (hollow vs. nonhollow organs)
Cardiovascular Review � Heart Rate � Blood Pressure ◦ 60 -80 bpm; athletes will vary ◦ 120/80; athletes will probably be lower � Cardiac Auscultation ◦ Heart sound, will practice this ◦ Refer to table 15 -5 (p. 579) for examples of heart sounds
Respiratory Review � Respirations per minute ◦ Typical adult 12 -14 � Breath ◦ ◦ sounds Auscultate over lobes of lungs (will practice) Rapid, shallow breaths= internal injury/shock Deep, quick breaths= asthma, pulmonary obstruction Noisy, raspy breaths- airway obstruction � Peak Flow Meter ◦ Practice in class
Pneumothorax � Accumulation of air in the pleural cavity ◦ Disrupts lungs ability to expand draw in oxygen �Can result in hypoxia, respiratory distress ◦ Usually due to a blunt or penetrating trauma �Could occur after a rib fracture ◦ Difficulty breathing � This is a medical emergency ◦ Lay them on the side that is injured while waiting for EMS � Tx ◦ Decompression- tube inserted into ribs
Hemopneumothorax � https: //www. youtube. com/watch? v=7_X 9 PDc t. Wh 8 � Same as a pneumothorax but now blood is collecting in the pleural cavity ◦ Patient is coughing up frothy blood �Actually common in football, ice hockey and men’s lacrosse
Splenic Injury � MOI ◦ Blunt trauma �Led to contusion or laceration ◦ Mono patients? � S&S ◦ Kehr’s sign- P! in left shoulder �Aggravated by movement, vomiting � Tx �Vomit could be greenish from bile ◦ Depends- surgical or observation ◦ Refer to ED immediately though
Kidney Pathologies � Contusion or Laceration ◦ Blunt trauma, fractured rib �Tenderness over impact site, abdominal rigidity �Blood in urine ◦ Refer to ED immediately � Kidney Stones ◦ Result from collection of incomplete kidney filtration �Formed by crystals of uric acid or calcium �Family hx, hypertension, ingesting caffeinated drinks, beer, wine or other foods high in calcium, sodium
Kidney Stones � S&S ◦ P! on flank (side that stone is on) ◦ P! during urination �Male equivalent to giving birth
Appendicitis � MOI ◦ Rapid, not usually blunt trauma � S&S ◦ Initially diffuse P! in abdomen, slowly moves to lower right quadrant, nausea, vomiting, constipation, low grade fever �Right leg bent up vs. down on table ◦ Usually males between 15 -25 ◦ P! over Mc. Burney’s point � Tx ◦ Immediate referral to ED ◦ Surgical removal- usually laproscopy
Hypertrophic Cardiomyopathy � Sudden death due to enlarged left ventricle ◦ Usually have no symptoms until collapsing and then death ◦ Family history is huge here �Echocardiogram
On-Field Evaluation � ABC’s (thoracic or abdominal injury) ◦ Thoracic-try to rule out life threatening emergencies �Can be difficult on the field because these pathologies progress ◦ Abdominal injury �Same thing, r/o life-threatening injury � Watch ◦ Injuries will progressively worsen- monitor patient on sidelines �If worse don’t hesitate to send to ED
Review � Facet dysfunction is the most common thoracic injury � Injury to internal organs need to be referred to emergency department to rule out major pathology ◦ Better to be safe than sorry � Auscultation of heart and lungs takes practice ◦ Clinical experiences, General Medicine Course