The Spine Chapter 25 Anatomy of the Spine






 –cervical sprain • Etiology: sudden snap of")
 • Etiology: cold draft of air or head")
 • Etiology: stretch or compression")



")
- Slides: 15
The Spine Chapter 25
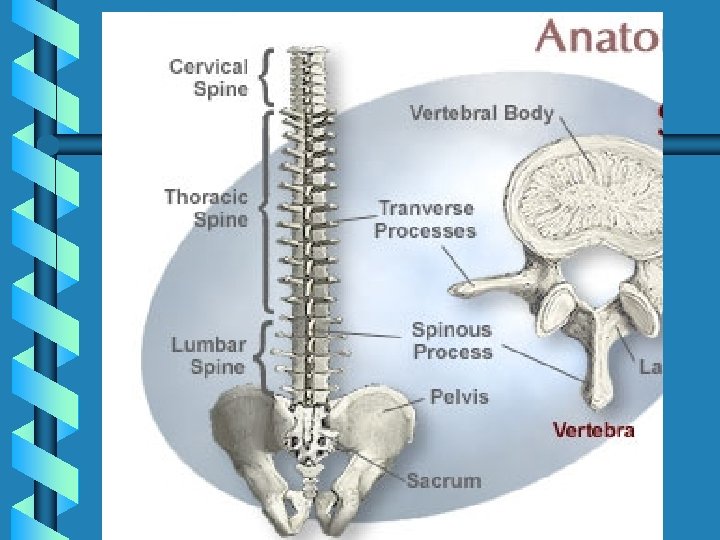
Anatomy of the Spine b b b Bones of the vertebral column • Cervical (7), thoracic (12), lumbar (5), sacral (5 fused), coccyx (4+ fused) – Intervertebral Disks - shock absorbers • Ligamentous Structures (anterior and posterior longitudinal and supraspinous) Muscles of the Spine (superficial and deep) • Erector spinae muscle group: superficial portion • Interspinalis, multifidus, rotatores, and semispinalis : Deep portion Spinal Cord, Nerves and Peripheral Branches
b 1. Disc b 2. Body b 3. Dura mater b 4. Epidural space b 5. Spinal cord b 6. Subarchnoid space
Preventing Injuries to the Spine b b Cervical Spine • Strengthening – protect by resisting excessive motion • Range of Motion – flexibility • Using correct techniques Lumbar Spine • Avoid Stresses – completing ADLs properly • Correct Biomechanical Abnormalities – strength and flexibility in the core • Correct techniques when lifting
Assessment of the Spine b b History “very important” – R/O cord injury Observation • posture and movement evaluation – Fatback: decrease lumbar curve with increase pelvic – Swayback: hip exten. at hip, flex of thoracic on lumbar spine; lumbar in lordosis, thoracic in kyphosis – Lordosis: increase in lumbar curve – Scoliosis: lateral curvature of spine – Kyphosis: increase in thoracic curve
b Palpation – proximal to distal; muscles and bony prominence b Special Tests • stress tests • Range of Motion b Neurological Exam • reflex
Injuries to the Spine Cervical Sprain (whiplash) –cervical sprain • Etiology: sudden snap of the head • Signs and Symptoms: similar to sprain but last longer • Management: Referral to r/o fracture an neurological problems; collar, RICE, NSAIDs, etc
Spine Injuries b Acute Toticollis (Wryneck) • Etiology: cold draft of air or head in unusual position for extended period of time • Signs and Symptoms: point tender, muscle spasm • Management: r/o more serious injury; break pain spasm cycle b Cervical Cord and Nerve Root Injuries • Etiology – – Laceration : dislocation or fracture Hemorrhage: dislocation, fx, sprain and strains Contusion: violent force to neck that does not cause dislocation Spinal Shock: severe twist or snap; transient signs of spinal cord injury • Signs and Symptoms: paralysis, motor and sensory systems affected • Management
Injuries to the Spine b Brachial Plexus Neurapraxia (Burner) • Etiology: stretch or compression of brachial plexus • Signs and Symptoms: burning sensation, numbness, tingling, weakness • Management: once symptoms resolve, athlete can return b Cervical Spine Stenosis • Etiology: narrowing of spinal canal; congential or developed • Signs and Symptoms: transient quadriplegia; persistent burners; weakness • Management: referral for diagnosis; advise to D/C participation
Injuries to the Spine b Mechanisms • Congenital: spondylolisthesis (forward subluxation of 5 th vertebrae); abnormal bony structure )length, width of vertebrae), etc • Idiopathic (mechanical or traumatic) – Mechanical: faulty posture, bad mechanics – Back Trauma: injuries occuring in competition; WATCH OUT FOR MIS-MANAGEMENT – Recurrent or chronic low back pain: malalignment, nerve rot compressions, muscle weakness
Injuries to the Spine b Herniated Lumbar Disk: usually L 4 -L 5 or L 5 -S 1 • Etiology: forward bending and twisting • Signs and Symptoms: Radiating pain unilaterally • Management: pain control; if persists, surgery may be indicated b Spondylolysis (degeneration of vertebrae) and Spondylolisthesis (slipping of the vertebral disk) • Etiology: hyperextension, direct blow, sudden twist • Signs and Symptoms: aching pain, change positions often, possibly some neurological symptoms • Management: bracing, rest, rehab focuses on trunk strengthening
Injuries to the Spine b Coccyx Injuries: sprain, subluxations, fractures • Etiology: direct impact • Signs and Symptoms: refer for x-ray, pain • Management: ring seat, analgesics b Sacroiliac Joint Dysfunction(sprain, inflammation, hypermobility, hypomobility) • Etiology: twisting, falling, landing heavy on one leg, etc • Signs and Symptoms: tenderness over site, guarding, pain, ASIS or PSIS asymmetrical • Management: manage pain, mobilizations, exercises to strengthen and re-align
Rehabilitation Principles for the Spine b Joint Mobilization (decrease pain, increase mobility, increase ROM) b Flexibility Exercises b Strengthening Exercises b Techniques for the Low Back • • • Pain Control (mobs, traction, modalities, etc) General Body Conditioning Joint Mobilization Traction Flexibility Exercises Strengthening Exercises