Wrist Hand Finger Evaluation ATTR 322 Krzyzanowicz Spring





- V (little finger) �Phalanx �Proximal �Middle �Distal")



 and interphalangeal (IP) joints ◦ MCP flex/ext and abd/add ◦")
 ◦ Posterolateral forearm; innervated by radial nerve")

























 � Range of Motion")













, and TFCC")
 � Treatment ◦")





 ◦")




























 of the thumb (MCP Joint)")







- Slides: 109
Wrist, Hand Finger Evaluation ATTR 322 Krzyzanowicz- Spring ‘ 14
Objectives � Understand bony and soft tissue anatomy of the wrist, hand fingers � Understand movement relationships of the wrist, hand fingers � Describe common injuries including deforimities to the wrist, hand fingers � Demonstrate the proper evaluation of the wrist, hand fingers to include ◦ Special tests ◦ Palpation ◦ MMT’s � Utilize EBP principles' in evaluation techniques
Clinical Anatomy
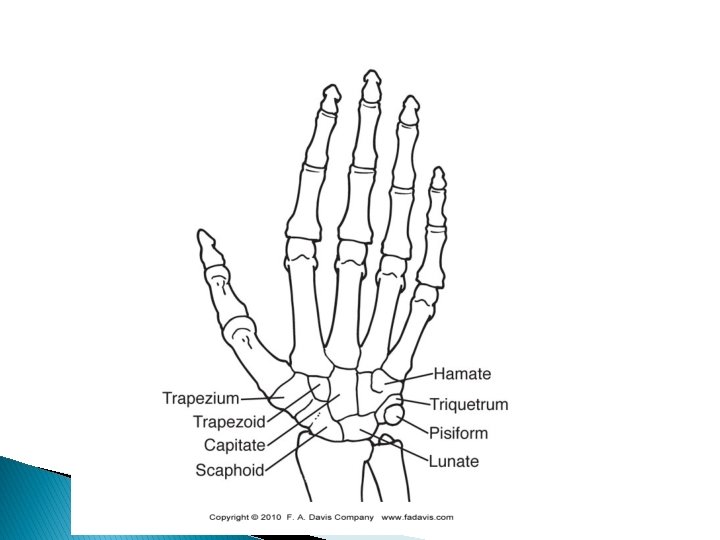
Clinical Anatomy � Forearm ◦ Distal Ulna ◦ Distal Radius � Wrist ◦ 8 carpal bones � Hand ◦ 5 metacarpals � Fingers ◦ 14 phalanges
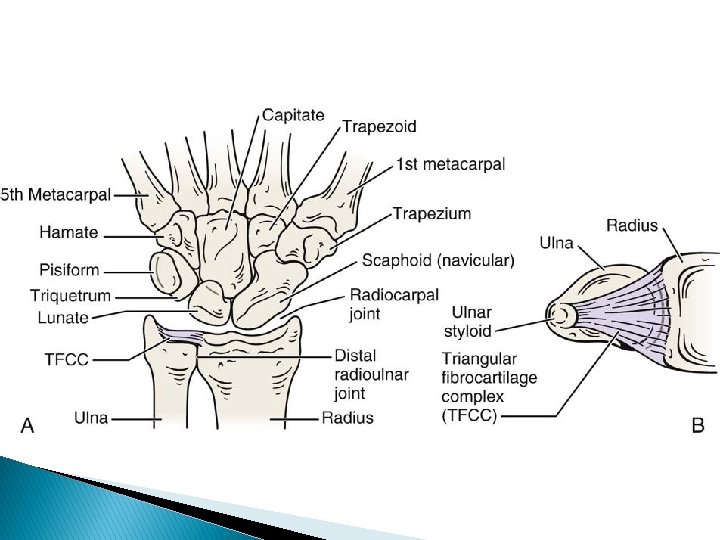
Clinical Anatomy � Forearm ◦ Distal radius broadens to form the ulnar notch on the medial surface to accept the ulnar head ◦ Radial styloid process- anterolateral border � Carpal bones ◦ Unusual shapes and irregular surfaces ◦ Aligned in two rows �Proximal: scaphoid, lunate, triquetrum, pisiform �Distal: trapezium, trapezoid, capitate, hamate
Clinical Anatomy � Metacarpals ◦ I (thumb)- V (little finger) �Phalanx �Proximal �Middle �Distal
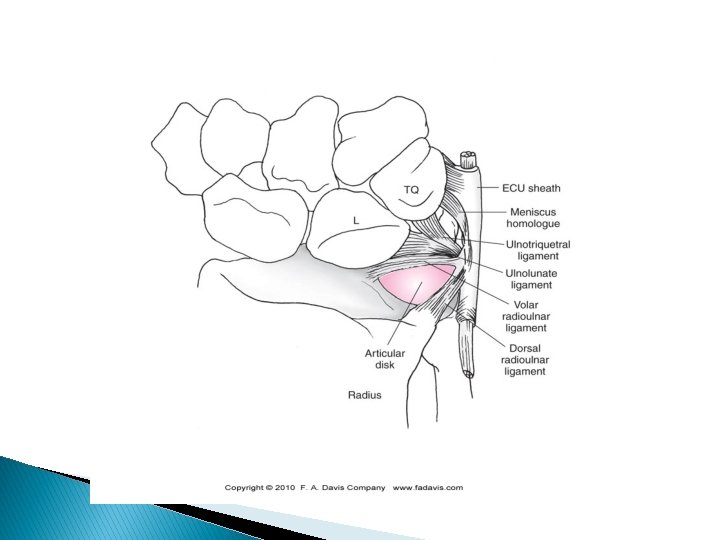
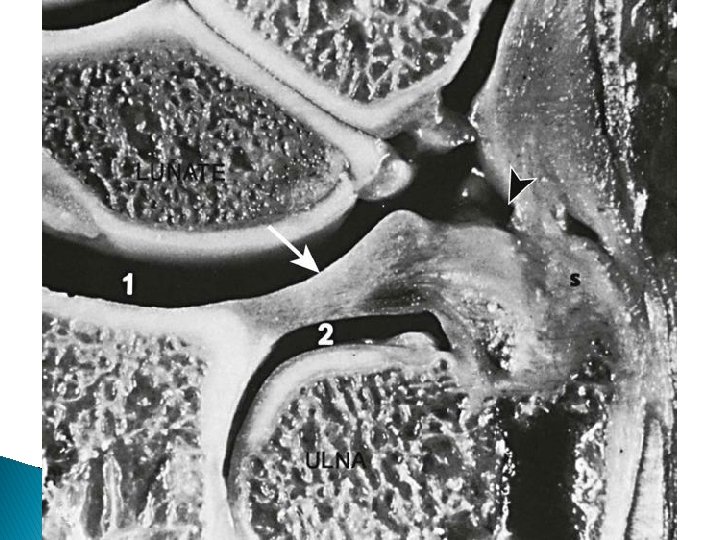
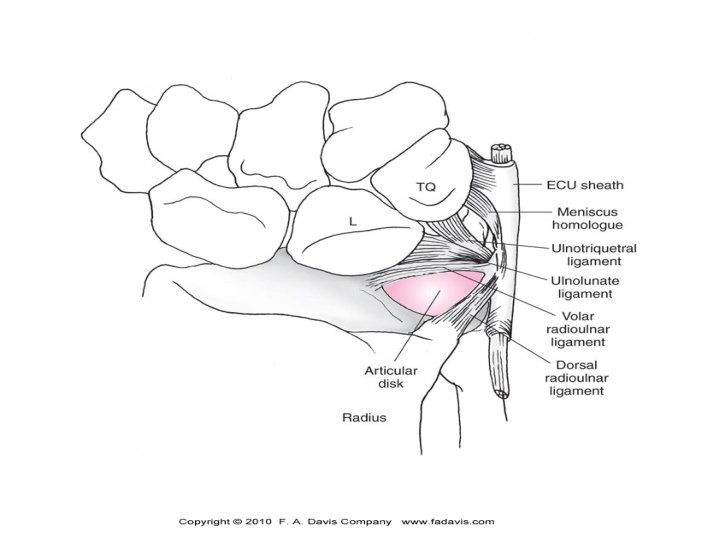
Articulations and Ligamentous Support � Distal radioulnar joint ◦ Supination and pronation � Radiocarpal joint ◦ Flexion and extension ◦ Radial and ulnar deviation �Radial collateral ligament � Triangular fibrocarilaginous complex (TFCC) ◦ On the ulnar side �Composed of an articular disk, ligaments and bone �Dissipates stresses on forearm during loading �Damaged by forced extension and pronation
Articulations � Intercarpal joints ◦ Joints between each carpal bone held in place by interosseous ligaments � Midcarpal joints ◦ Separation of the proximal and distal carpal rows � Carpometacarpal Joints ◦ First 3 metacarpals articulate with the carpal bone ◦ Thumb is 1 st CMC joint �Saddle joint, flex/ext and abd/add
Articulations � Metacarpophalangeal (MCP) and interphalangeal (IP) joints ◦ MCP flex/ext and abd/add ◦ IP flex/ext
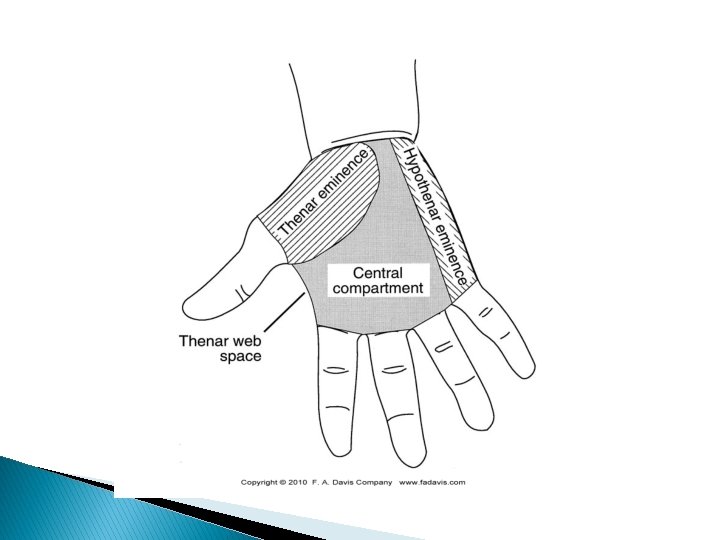
Musculature � Extensor muscles (p. 756 -759) ◦ Posterolateral forearm; innervated by radial nerve � Flexor muscles ◦ Anteriomedial forearm; innervated by median nerve - except flexor carpi ulnaris (ulnar) � Palmar muscles ◦ Intrinsic muscles �Thenar eminence (thumb side) �Hypothenar eminence (5 th digit side)
Nerves � Ulnar nerve ◦ Superficial just medial to carpal tunnel �Passes through the Tunnel of Guyon formed by the hamate and pisiform �Superficial branches provide sensory input on palmar side of little finger and medial side of ring finger �Deep branch innervates the hypothenar eminence � Radial nerve ◦ Motor (posterior interosseous nerve) and sensory (superficial radial nerve) �Innervates wrist and finger extensors and dorsal hand �Easy way to check for nerve issue is wrist extension
Nerves � Median nerve ◦ Follows the flexor digitorum superficialis through the forearm �Travels through the carpal tunnel laterally and divides into motor and palmar branches �Motor- supply thenar emience �Palmar- sensation to palmar surface of the thumb, index and middle finger
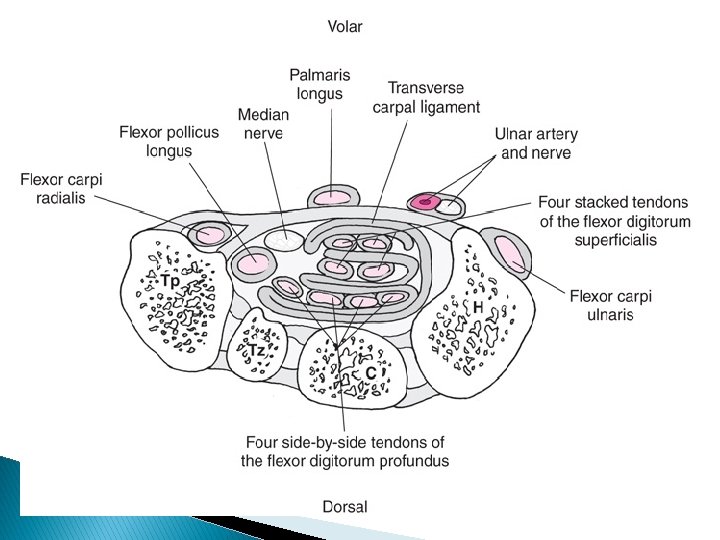
Carpal Tunnel � Tunnel’s floor ◦ Formed by the proximal carpal bones � Roof ◦ Formed by the transverse carpal ligament � Ten structures pass through the tunnel ◦ Listed in text � Inflammation ◦ Median nerve is effected �Grip strength is decreased
Carpal Tunnel
Clinical Examination � Kinetic Chain ◦ Evaluation of elbow, shoulder, cervical spine may be needed in wrist, hand finger evaluations � History ◦ Previous injury, fractures (common) ◦ General medical health �Peripheral vascular disease (raynaud’s) �Diabetic- chronic wrist pain �Pregnancy- increased risk of carpal tunnel syndrome
Clinical Examination � History of present condition ◦ Location of pain �Which nerve? ◦ MOI �FOOSH? Compression? ◦ Sounds �Clicking usually means TFCC ◦ Duration �Scaphoid? ◦ Description of Sx �Aching/throbbing=bony or soft tissue �Burning/tingling=neurolo gic or vascular ◦ Change in activity �ADL’s �Job (ergonomics) � Computer work
Inspection � Functional Observation ◦ Replicate activities that cause pain and ADL’s �Compensating in shoulder? �Decreased grip strength � General Inspection ◦ Posturing of wrist and hand ◦ Gross deformity ◦ Palmar creases ◦ Lacerations or scars ◦ Nails
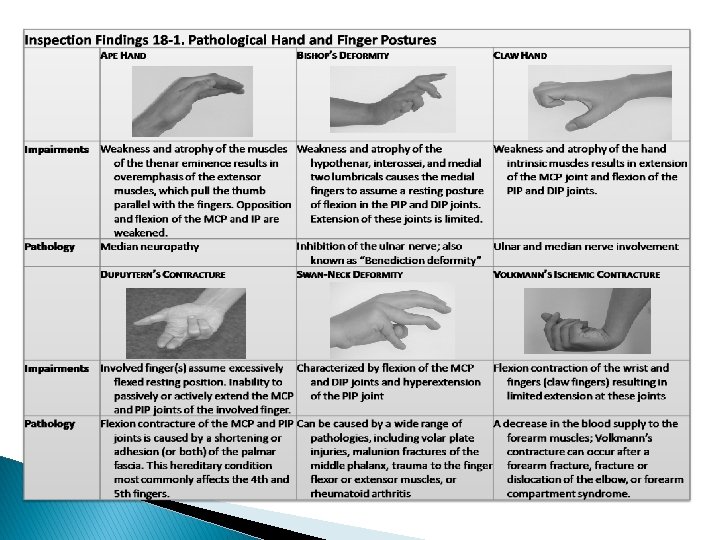
Ape
Bishop’s
Claw Hand
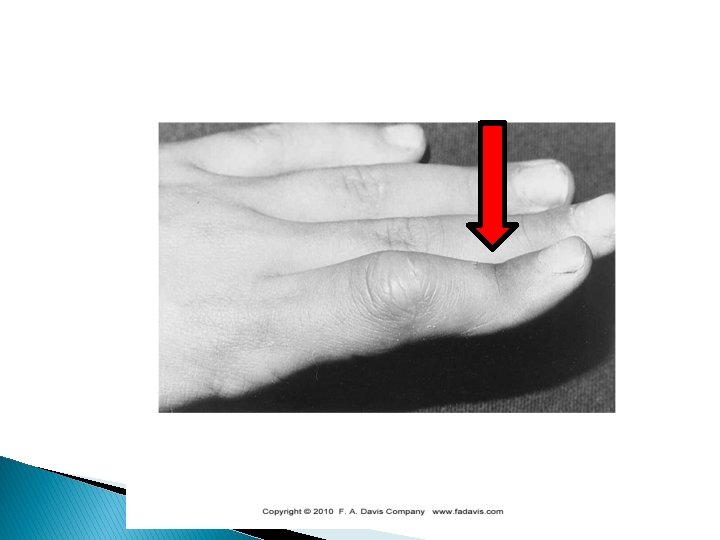
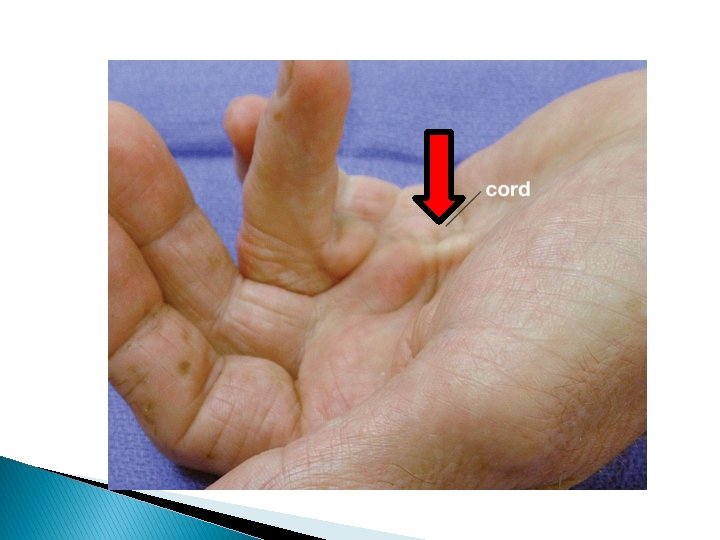
Dupuytern’s
Swan-neck
Volkmann’s
Inspection � Wrist and Hand ◦ Continuity of distal radius/ulna; carpals/metacarpals ◦ Alignment of MCP joints ◦ Ganglion cyst � Thumb and Fingers ◦ Skin and fingernails
Finger Deformities
Jersey finger
Mallet
Boutonniere deformity
Palpation � Palpation group ◦ ◦ ◦ ◦ of the wrist and finger flexor muscle Wrist flexor group Flexor carpi ulnaris Flexor digitorum profundus Flexor digitorum radialis Flexor carpi radialis Palmaris longus Carpal tunnel
Palpation � Palpation of the wrist and finger extensor muscle group 1. 2. 3. 4. 5. 6. Wrist and finger extensor group Extensor digitorum communis Extensor pollicis longus Abductor pollicis longus Extensor pollicis brevis Abductor pollicis longus
Anatomical Snuffbox
Palpation � Palpation of the hand 1. Metacarpals 2. Collateral ligaments of the MCP joints 3. Phalanges 4. Collateral ligaments of the IP joints 5. Thenar compartment 6. Thenar webspace 7. Central compartment 8. Hypothenar compartments 9. Ulna 10. Ulnar styloid process 11. Ulnar collateral ligament 12. Distal radius and styloid process 13. Lister’s tubercle 14. Radial collateral ligament
Palpation � Palpation of the carpals 1. 2. 3. 4. 5. 6. 7. 8. Scaphoid Trapezium Lunate Triquetrum Pisiform Hamate Capitate Trapezoid Acronym?
Joint and Muscle Function Assessment � Range of Motion (wrist) � Range of Motion (fingers and thumb) ◦ Flexion (80 -90) and extension (75 -85) ◦ Ulnar deviation (35 degrees) and radial deviation (20 degrees) �Flexion and extension �Abduction and adduction �Opposition (thumb only)
Wrist ROM
First CMC Joint ROM
Finger ROM
Grip Dynamometry
Joint Stability Testing � Stress testing ◦ Tests for collateral support of wrist ligaments �UCL (TFCC involvement) �RCL ◦ Tests for collateral support of IP joints �UCL �RCL �Laxity in either could be an avulsion fracture
WRIST PATHOLOGIES
Scaphoid Fractures � About 70% of all carpal fx’s involve the scaphoid ◦ Bony block limiting wrist extension ◦ Most prevalent in 15 -30 y/o ◦ Poor blood supply �If fractured- compromises nutrition to proximal part �Causes nonunion fractures and avascular necrosis ◦ Can result in instability of proximal carpal row
Scaphoid Fractures � MOI ◦ Usually FOOSH or forceful hyperextension � S&S ◦ Ache in area of anatomical snuffbox, increases with palpation ◦ Crepitus ◦ Severe P! with overpressure (radial deviation, flex/ext)
Scaphoid Fractures � Management ◦ X-ray �Usually doesn’t show though ◦ MRI/CT scan �Better, but still not as sensitive ◦ Treat as a fracture �Immobilize thumb and wrist (6+ weeks) ◦ Surgical intervention �Bone from hip inserted at fx site ◦ We miss scaphoid fx’s all the time! When in doubt refer it out
Scaphoid Fractures
Hamate Fractures � MOI ◦ FOOSH; trauma to the palm swinging a golf club or baseball bat �Fractured through axial load applied to 4 th or 5 th metacarpal � S&S ◦ Minimal swelling in the hypothenar eminence ◦ Possible protrusion over hamate ◦ Point tender over hamate �P! with 5 th finger abd/add and with passive extension of 5 th finger
Lunate Dislocation � MOI ◦ Forced hyperextension �Can displace dorsally or palmarly � S&S ◦ P! along radial side of palmar or dorsal aspect of wrist that limits ROM ◦ Bulge may be visible ◦ Can cause parethesia in middle finger ◦ Third knuckle is level with other knuckles ◦ Possibility of scaphoid fx as well
� http: //www. imageinterpretation. co. uk/wrist. h tml
Wrist Sprains � Very general term ◦ Rule out carpal fx (scaphoid), and TFCC � Scapholunate ligaments ◦ Most common sprain to the wrist � MOI ◦ Typically forced hyperextension � S&S ◦ Wrist and hand giving way; numbness; decreased ROM
Wrist Sprains � Special Tests ◦ Watson’s test (show in lab) � Treatment ◦ X-ray to r/o fx (if you think it’s needed) ◦ Rest �Soft splint, cast, etc
Watson’s Test
Triangular Fibrocartilage Complex � TFCC ◦ Trauma or repeated injury to TFCC and UCL can result in permanent disability �Increased risk in sports in the closed kinetic chain � MOI ◦ Forced hyperextension (blocking, weightlifting) ◦ Repeated weight bearing causing degeneration � S&S ◦ P! along ulnar side of wrist; decreased ROM due to P!
Triangular Fibrocartilage Complex � S&S ◦ P! when pushing up from a chair � Palpation ◦ Ulnar styloid process- avulsed UCL? � Treatment ◦ Cortizone injection ◦ Surgical management ◦ Casting usually 6 -8 weeks
Carpal Tunnel Syndrome � Refers to the S&S caused by compression of median nerve as it passes through the carpal tunnel ◦ Most frequented causes is fibrosis of the synovium of the flexor tendons secondary to tenosynovitis �May occur due to repetitive microtrauma, acute trauma to the carpal tunnel or progressive degeneration of the carpal tunnels structures
Carpal Tunnel Syndrome � S&S ◦ Paresthesia and P! along median nerve distribution �Thumb, index, middle & lat. Half of ring finger) �Often occurring at night �Relieved when shaking ◦ Inspection may reveal �Atrophy of thenar muscles �Decreased grip strength ◦ Other symptoms �Decreased strength in abductor pollicis brevis and opponens pollicis
Carpal Tunnel Syndrome � Other symptoms ◦ Poor posture (forward head, rounded shoulders) ◦ Mimic s&s for C 7 impingement �May need to evaluate c-spine and elbow � Special Tests ◦ Tinel’s sign= not a great test ◦ Phalen’s and reverse phalen’s � Tx ◦ Rest, postural training, NSAID’s, splinting ◦ Surgical intervention
Phalan’s Test
Wrist Ganglion � “Bible ◦ ◦ ◦ Cyst” A synovial cyst characterized by herniation of synovial fluid through the joint capsule or synovial sheath of the tendon May form on dorsal or volar aspect Signs and symptoms � Observable and palpable localized mass � Tenderness and discomfort with wrist extension (dorsal ganglion) � May or may not impede ROM or function
Ganglion Cyst
HAND FINGER PATHOLOGIES
Metacarpal Fractures � Typically fractured due to a compressive force along the bone’s shaft ◦ Such as punching with a fist ◦ Common to hear the bone snap ◦ Gross deformity is common �Immediate swelling ◦ Tenderness along fracture site (pinpoint usually) �crepitus? ◦ Fingers or metacarpal may rotate when hand is attempting to flex ◦ Could happen to any of the metacarpals
Boxer’s Fracture � Fracture to the 5 th metacarpal ◦ Common incidence after an improperly thrown punch ◦ Depressed 5 th MCP joint � Treatment ◦ Casting or ORIF �Usually casted 6 -8 weeks � Special Tests ◦ Compression test (rotate)
Collateral Ligament Injuries � Trauma to the collateral ligaments of the fingers usually results from a dislocation ◦ Can result from direct trauma too though �Stub, jam your finger ◦ Pain and swelling usually set it �Hurts like hell! ◦ Varus/Valgus testing �Treatment though?
Phalanx Fractures � Fractures common of distal phalanx are the most ◦ MOI is usually direct trauma, shear force or crushing force ◦ S&S include �Gross deformity, swelling, inability to move finger, heard and felt a snap, crepitus ◦ Tx �Splint, surgical intervention
Finger Dislocations � Very common in contact sports and basketball ◦ ALWAYS CHECK FOR AN OPEN DISLOCATION ◦ DO NOT relocate as a student �DO NOT relocate a thumb! ◦ MOI: �Direct truama, shear force ◦ S&S �Gross deformity, pain and inability to move joint ◦ Tx �Reduce (if possible), splint and refer for x-ray (good chance it’s fractured)
Volar Plate Rupture � ◦ ◦ ◦ Results from hyperextension of the PIP joint Pain and tenderness on the palmer aspect Loss of function Swelling Disruption cause subluxation and permanent hyperextension Complications are a swan-neck or pseudoboutonniere deformity
Volar Plate Injury
Volar Plate Injury
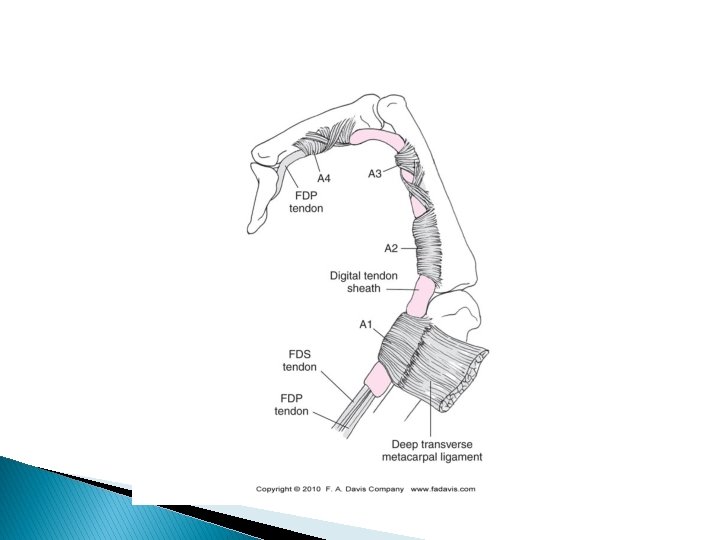
Tendon Avulsions � Very common and can occur from direct blows or abrupt forces (throwing) ◦ Flexor Digitorum Profundus (Jersey Finger) rupture�Occurs when distal phalanx is forcefully extended while the finger is flexing (grabbing) �Signs and symptoms Immediate pain and LOF Swelling Point tenderness at tendinous attachment Complete rupture results in inability to flex distal phalanx � Incomplete rupture results in pain and weakness � Unable to flex DIP joint against resistance � �
Jersey finger
Extensor Tendon Avulsion � Mallet finger ◦ Results from an extended distal phalanx that is suddenly and forcefully flexed (catching) ◦ May be an avulsion fracture or tendon rupture ◦ Signs and symptoms � Severe pain and immediate LOF � Point tenderness over distal attachment � Flexion deformity of the distal phalanx � Inability to actively extend the distal phalanx � Avulsion fracture has better chance to heal without surgery
Mallet Finger
Boutonniere Deformity � Extensor ◦ ◦ ◦ Tendon Rupture Characterized by flexion of the PIP joint and hyperextension of the DIP joint Injury to the central slip of the extensor digitorum tendon at the PIP joint from forceful flexion (“Buttonhole rupture”) Signs and symptoms � � Localized pain and swelling over middle phalanx Point tenderness near the tendon insertion Weakness with extension of the PIP joint will be flexed; DIP joint is hyperextended
Boutonniere Deformity
Splinting of Common Finger Injuries Deformity Splinting Position Jersey Finger DIP Joint in flexion Mallet Finger DIP Joint in extension Boutonniere Deformity PIP and DIP joints in extension Phalanx fracture Position found Metacarpal fracture Palmar surface of wrist and hand Unreduced dislocations Position found
Dupuyten’s Contracture � ◦ ◦ Flexion deformity typically seen in the older adult population Flexion contracture of the MCP and PIP joints as a result of contracture of the palmar fascia Typically affects the fourth and fifth digits
Tendonitis/Tendosynovitis � ◦ ◦ Inflammation of the tendon or its synovial sheath Results from overuse or repetitive motion, direct trauma, and continued use following a tendon injury Signs and symptoms � � � Point tenderness over involved tendon Swelling Palpable crepitus Pain with active and resisted motion Pain with passive stretching of the tendon
De. Quervain’s Disease � ◦ ◦ Tenosynovitis of the abductor pollicis longus and extensor pollicis brevis tendons on the radial side of the thumb; Causes inflammation of tendons Results from repetitive motion that combines gripping and wrist ulnar deviation Signs and Symptoms � Pain along thumb side of wrist which may either appear gradually or suddenly; may travel into wrist and forearm � Pain is usually worse with use of the hand & thumb, especially when forcefully grasping things or twisting the wrist � There may be occasional catching or snapping of the thumb
De. Quervain’s Tenosynovitis
Finkelstein’s Test
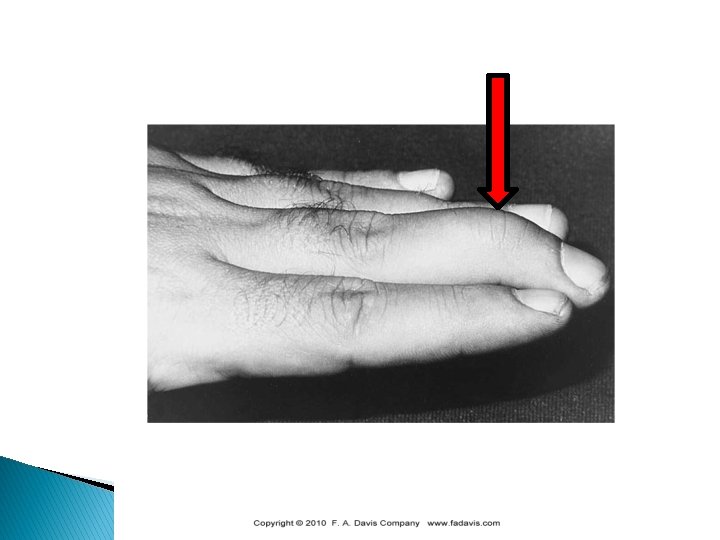
Gamekeeper’s Thumb � Involves the ulnar collateral ligament (UCL) of the thumb (MCP Joint) ◦ A. k. a. –skiers thumb �Results from forced abduction and hyperextension of the thumb or axial load to the thumb �Avulsion fracture is very common ◦ Signs and symptoms � Pain, swelling, and visible bruising � Point tenderness over UCL � Instability consistent with degree of injury � Laxity >35° & absent end feel = rupture of UCL
Figure 14. 6
Classification & Treatment of Gamekeeper’s Thumb � Type 1: incomplete rupture � Type 2: complete rupture; distal end may displace superficial & proximal to the adductor aponeurosis � Short arm thumb spica cast (6 -10 wks) for incomplete rupture � Cast should incase both the IP and MP joints, with thumb in slight adduction � Protective splint until pain free & complete ROM
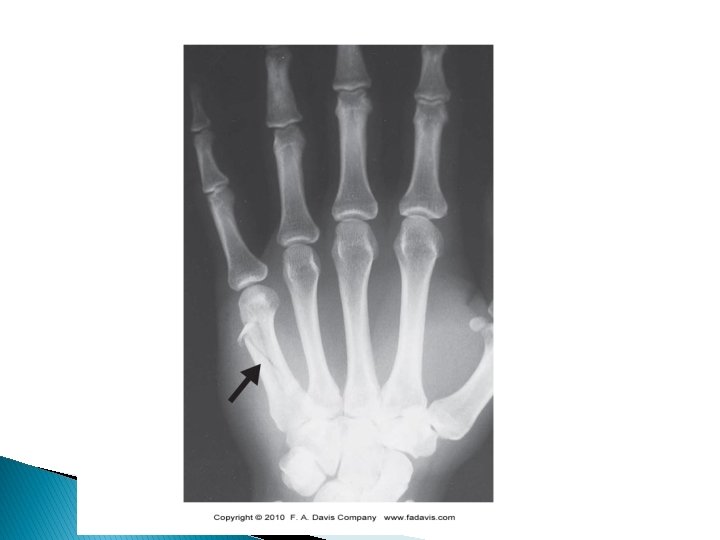
Bennett’s Fracture � Involves the base of first metacarpal bone ◦ MOI: striking an object with a closed fist ◦ �Metacarpal displaced due to pull from abductor pollicis longus Signs and symptoms � � Immediate localized pain, rapid swelling, and LOF Deformity may or may not be present Crepitus at the MCP ↑ pain on axial compression of 1 st metacarpal
Bennett’s Fracture
On-Field Evaluation � Usually athletes with hand, finger or wrist injuries leave the field on their own ◦ Cradling and protecting injured area ◦ Deformity is usually obvious and may involve open or closed fractures or dislocations of the fingers ◦ Always remove the glove(s) �Cut off if needed
Fractures and Dislocations � Fractures of radius and ulna as well as dislocations of the radiocarpal joint must be immobilized in the position found ◦ Vacuum splint or SAM Splint ◦ Always check pulse and neuro status before and after ◦ Open fracture/dislocations should be covered with sterile gauze � IP dislocations ◦ Reduce (if you can), splint and x-ray to r/o fx � Hand finger ◦ Immobilize, splint and x-ray (24 h rule) � Lacerations ◦ Superficial structures of tendons, etc- refer to E. D.
Review � Wrist, hand finger injuries are very common! ◦ Wrist can be difficult to diagnose properly due to many small involved structures � Many injuries ◦ Remember MOI and distinguishing sign or symptom for each injury � Practice ◦ Makes perfect, don’t get scared of the wrist, hand finger- attack it