DILATED CARDIOMYOPATHY Aarti Raghu CARDIOMYOPATHY Cardiomyopathies are diseases


 Task Force on the Definition")
 is characterized by Dilation and impaired contraction of one")






















 • serum calcium (hypocalcemia) • serum creatinine and")











 negative chronotropic effect with reduced myocardial")







 have echocardiographic abnormalities,")


 may have a role in")




- Slides: 60
DILATED CARDIOMYOPATHY Aarti Raghu
CARDIOMYOPATHY Cardiomyopathies are diseases whose dominant feature is direct involvement of the heart muscle itself. n The World Health Organization (WHO) in 1980 defined cardiomyopathies as "heart muscle diseases of unknown cause, " to distinguish cardiomyopathy from cardiac dysfunction due to known entities such as hypertension , pericardial, congenital, ischemic heart disease, or valvular disease. n In clinical practice, however, the term "cardiomyopathy" has also been applied to diseases of known cause (eg, ischemic cardiomyopathy and hypertensive cardiomyopathy).
n 1995 WHO/International Society and Federation of Cardiology (ISFC) Task Force on the Definition and Classification of the Cardiomyopathies expanded the classification to include all diseases affecting heart muscle and to take into consideration etiology as well as the dominant pathophysiology. n In this classification, the cardiomyopathies were defined as "diseases of the myocardium associated with cardiac dysfunction. " They were classified according to anatomy and physiology into the following types, each of which has multiple different causes: n Dilated cardiomyopathy Hypertrophic cardiomyopathy Restrictive cardiomyopathy Arrhythmogenic right ventricular cardiomyopathy Unclassified cardiomyopathies (this includes endomyocardial fibroelastosis and ventricular non compaction) n Cardiomyopathies that are associated with specific cardiac or systemic disorders generally fall into one of these categories. These include ischemic, valvular, hypertensive, and a host of "inflammatory, " metabolic, toxic, and inherited disorders.
DILATED CARDIOMYOPATHY Dilated cardiomyopathy (DCM) is characterized by Dilation and impaired contraction of one or both ventricles n Impaired systolic function Patients may or may not develop overt heart failure The earliest abnormality usually is ventricular enlargement and systolic contractile dysfunction, with the signs and symptoms of congestive heart failure often (but not invariably) developing later. n
The numbers n 10, 000 deaths/year due to DCM n 46, 000 hospitalizations / year in the United States n Incidence 5 -8 cases per 100, 000 population n Prevalence of 36 per 100, 000 n These figures may underestimate the frequency of the disorder because so many patients with dilated cardiomyopathy are asymptomatic. It has been suggested that 14 percent or more of the middle-aged and elderly population have asymptomatic left ventricular systolic dysfunction n It occurs almost three times more frequently in blacks and males as in whites and females (this difference does not appear to be related solely to differing degrees of hypertension, cigarette smoking, or alcohol use) n Survival in blacks and males appears to be worse than in whites and females. n Idiopathic DCM is the primary indication for cardiac transplantation
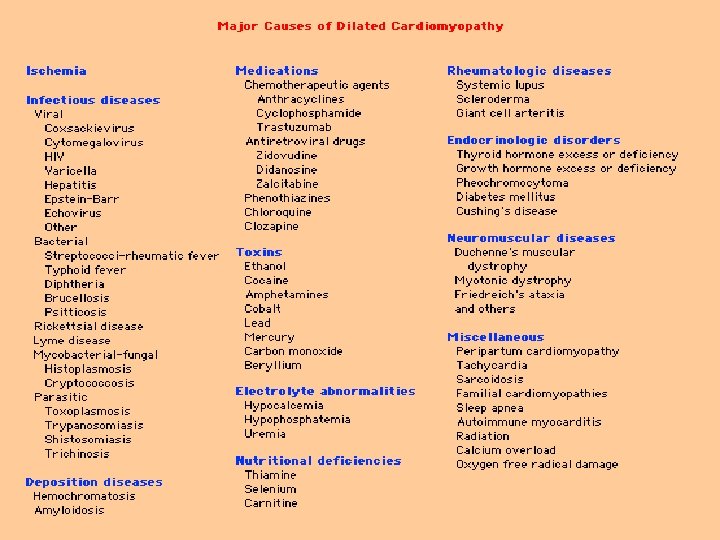
ETIOLOGY-the shorter list CAUSES OF DCM The relative frequency of the different causes in patients with initially unexplained cardiomyopathy was assessed in a review of 1230 patients at Hopkins Idiopathic — 50 percent THE Cs OF CARDIOMYOPATHY n n CARDITIS/COXSACKIE Cause Unknown/IDIOPATHIC n CHAGAS DISEASE n CAD n COLLECTION OF INTRACELLULAR DEPOSITS n CONCEPTION n COCAINE Hypertension — 4 percent n COORS HIV infection — 4 percent n CONNECTIVE TISSUE DISEASE Connective tissue disease — 3 percent n CHEMOTHERAPY Substance abuse — 3 percent n CONGENITAL / familial Doxorubicin— 1 percent n CARNITINE DEFICIENCY Other — 10 percent n un COMMON Myocarditis — 9 percent Ischemic heart disease — 7 percent Infiltrative disease — 5 percent Peripartum cardiomyopathy — 4 percent ……………… OR COGNAC!!!
Does etiology matter?
Yes! What is important is the recognition that the complete list of possible causes of DCM is extensive, and that accurate diagnosis is important because some entities respond to specific preventive or therapeutic management. Hence, prognosis varies depending on the cause of DCM.
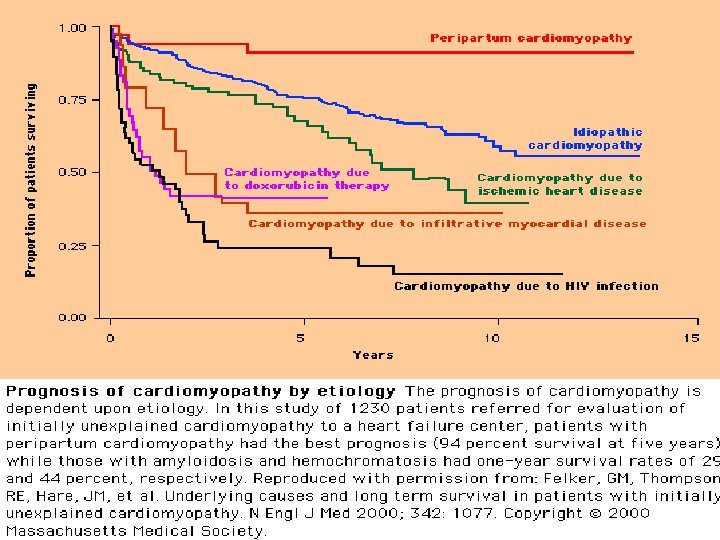
NATURAL HISTORY n n n Symptomatic patients -the course usually is one of progressive deterioration 1/4 newly diagnosed patients referred to major medical centers die within a year 1/2 die within 5 years 1/4 with recent-onset DCM improve spontaneously with a reduction in cardiac size and longer survival, even some sick enough initially to be considered for cardiac transplantation. In some patients clinical and functional improvement may occur years after initial presentation. n Patients with minimal or no symptoms- the progression of the disease in these patients is unclear, although there is some evidence that the longterm prognosis is not good. n In patients with mild dilatation not referred to a medical center the prognosis may be more favorable, due in part to earlier diagnosis and perhaps more effective treatment options now available in the community.
CLINICAL PRESENTATION n n n n Most patients present between the ages of 20 and 60, but DCM can occur in children and the elderly Affected patients can present in a number of different ways. The most striking symptoms of DCM are those of left ventricular failure. Fatigue and weakness due to diminished cardiac output are common. Right-sided heart failure is a late and ominous sign and is associated with a particularly poor prognosis. Chest pain occurs in about one third of patients and may suggest concomitant ischemic heart disease. The demonstrated reduction in the vasodilator reserve of the coronary microvasculature in DCM suggests that subendocardial ischemia may play a role in the genesis of chest pain that occurs despite angiographically normal coronary arteries. Chest pain secondary to pulmonary embolism and abdominal pain secondary to congestive hepatomegaly are frequent in the late stages of illness.
Case 1 A 40 y/o AA lady with h/o copd, asthma, HTN, DM, gout presents to the ER with cough, SOB of 2 weeks duration not relieved by inhalers. She was treated at Parkland for pneumonia with levaquin 10 days ago with no improvement in symptoms. No orthopnea or PND. H/o occasional alcohol consumption. She is tachypneic and is satting at 87% on room air. On exam you note she has diffuse wheezes, bibasilar crackles and b/l pitting pedal edema. BNP comes back at 560. Chest X ray shows increased vascular markings and significant cardiomegaly. EKG shows non specific ST changes. Dobutamine stress echo shows no regional wall motion abnormalities and EF of 30 -35%. You consult a cardiologist and she undergoes cardiac cath which shows no CAD. Ventriculogram shows EF of 17%. She improves on diuretics and placed on spironolactone and hydralazine (A-HEFT) but no beta blockers due to her asthma/copd. She later reports that her sister died of “heart failure” at the age of 36!! Familial linkage of DCM - in 20 percent or more of patients, a firstdegree relative also shows evidence of DCM. Some asymptomatic relatives of patients with DCM have subclinical left ventricular enlargement and/or dysfunction that may progress to overt symptomatic DCM.
Types of transmissionn Autosomal dominant transmission- seen in most familial cases - six chromosomal loci have been identified. n Autosomal recessive transmission n X-linked inheritance- One form of familial X-linked DCM is due to a deletion in the promoter region and the first exon of the gene that codes for the protein dystrophin, a component of the cytoskeleton of myocytes. This has fueled speculation that a resulting deficiency of cardiac dystrophin is the cause of the associated DCM n Mitochondrial DNA mutations have been reported as well. n Whether any of the patients without apparent familial linkage has a genetic predisposition to DCM remains unknown. There is great interest in using molecular genetic techniques to identify markers of disease susceptibility in asymptomatic carriers at risk for the eventual development of overt clinical DCM. n An example of such a marker may be the angiotensin-converting enzyme DD genotype that is found with increased frequency in DCM patients. n One intriguing familial metabolic deficiency is that of carnitine, with improvement occurring in the myopathy with carnitine repletion
Diagram showing the cardiac myocyte and the molecules that have been implicated in dilated cardiomyopathy. The actin cytoskeleton is linked to the extracellular matrix by dystrophin and the dystrophin-associated glycoprotein complex. Linkage of the actin cytoskeleton to the contractile apparatus is hypothesized to occur through the muscle LIM (Lin-11, Isl-1, Mec-3) protein (MLP). A nuclear transcription factor, cyclic AMP response-element binding protein (CREB), is shown binding to a cyclic AMP response element in the myocyte DNA. Mutations in dystrophin and other members of the dystrophin-associated glycoprotein complex, as well as in MLP and CREB, have all been shown to result in dilated cardiomyopathy in mice or humans. (From Leiden JD: The genetics of dilated cardiomyopathy: Emerging clues to the puzzle N Engl J Med 337: 1080, 1997. Copyright 1997, Massachusetts Medical Society. )
Case 2 60 y/o white male with h/o acute onset fever, chills, nausea, dry cough who recently stayed at a motel in Louisiana is found to have few bilateral crackles and bilateral fluffy infiltrates on CXR and also an enlarged cardiac silhouette. Urine legionella antibody is positive (of course!!). After addressing his infection you work him up with an echo for function and find an EF of 40%. He is completely asymptomatic at discharge but you put him on beta blockers and ACE inhibitors and ask him to follow up with a cardiologist every year. Some patients are asymptomatic and yet have left ventricular dilatation for months or even years. This dilatation may be recognized clinically only later when symptoms develop or when routine chest roentgenography demonstrates cardiomegaly.
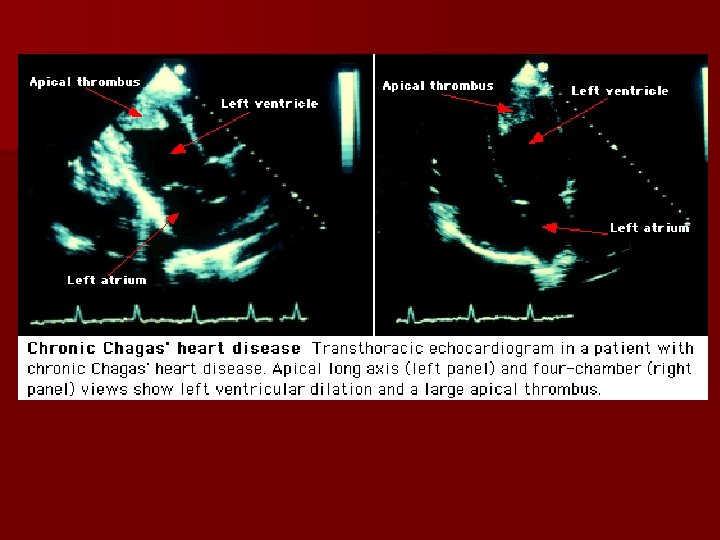
n Case 3 - 45 y/o AAM with gradually progressive dyspnea who now has dyspnea at rest, orthopnea, PND, cough with pink frothy sputum and pulse ox of 85%. n Case 4 – 40 y/o lady with h/o CA breast and SOB, palpitations after chemotherapy. EKG shows AF. CXR shows cardiomegaly. Case 5 - Stroke in a young lady with h/o anorexia and alcoholism. Echo shows 4 chamber dilation and mural thrombus. One complication is the presence of left ventricular thrombus and, in certain circumstances, development of left atrial thrombi. Detection of the latter requires TEE. n n Case 6 - CHF in a 60 y/o wm with h/o DM, HTN- no segmental wall motion abnormalities on ECHO but CAD on catheterization.
n Case 7 -17 y/o with DOE and new onset HSM on exam. This is a case of congenital DCM. Left ventricular dilation----> distortion of the bullet-shaped geometry of the left ventricle ----->the left ventricle becomes more spherical---->draws the papillary muscles away from the mitral valve annulus ---->results in annular functional mitral regurgitation due to abnormal coaptation of the mitral valve. Mitral regurgitation severity may range from mild to severe-- left atrial dilation Right ventricle can be primarily affected with dilation and hypokinesis and secondarily affected due to subsequent pulmonary hypertension from MR. The magnitude of secondary and pulmonary hypertension can be reliably determined from Doppler tracings of the tricuspid valve. Evaluation of diastolic properties of the left ventricle may provide valuable prognostic information.
Case 8 n An 86 y/o lady from an assisted living facility with h/o chronic A-fib on coumadin and diltiazem for rate control presents with CP, palpitations and confusion. She has no h/o CHF. Exam, Xray, labs, bnp show evidence of CHF/cardiomegaly and RVR. She is diuresed and rate controlled and her confusion resolves. n Virtually every form of supraventricular tachyarrhythmia, including ectopic atrial tachycardia, nonparoxysmal junctional tachycardia, and atrial fibrillation (AF), has been associated with reversible left ventricular dysfunction or "cardiomyopathy. " The development of a cardiomyopathy has also been documented with ventricular tachyarrhythmias. n Atrial fibrillation (AF) – cause or effect?
PATHOPHYSIOLOGY — n n Depletion of myocardial energy stores — reduced myocardial levels of creatine, phosphocreatine, and adenosine triphosphate (ATP), and diminished activity of the Na-K-ATPase pump. alterations in cellular metabolism with mitochondrial injury and increased activity of Krebs cycle oxidative enzymes. tachycardia-mediated depletion of high energy stores, which may be mediated in part by ischemia, is reversible and may explain the reversibility of this cardiomyopathy. Myocardial ischemia — Abnormalities in subendocardial to subepicardial flow ratios and impaired coronary flow have been found in tachycardia mediated cardiomyopathy. The impaired coronary blood flow occurs in association with elevation in cardiac filling pressures and impaired left ventricular diastolic function. Abnormal calcium handling and beta adrenergic responsiveness n n Abnormalities in both calcium channel activity and sarcoplasmic reticulum calcium transport Diminished beta-adrenergic responsiveness due to reduced myocyte beta-1 receptor density (downregulation) . The reduction in beta receptor density and responsiveness is independent of hemodynamic and neurohumoral factors. (While on the subject- beta receptor polymorphisms are associated with different risks of progression to failure-The Gly 49 allele in the beta 1 -adrenergic receptor and the 5' LC-Cys 19, Arg 16, and Gln 27 alleles in the beta 2 -adrenergic receptor were associated with a lower risk of heart failure in idiopathic dilated cardiomyopathy, suggesting that the beta 1 - and beta 2 -adrenergic receptor genes are modifier genes. ) Oxidative stress and injury In patients with AF and atrial dysfunction, there is histologic evidence of oxidative stress and injury in the atrial myocardium. This results in peroxynitrite formation-- which modifies myofibrillar proteins---- contributes to loss of fibrillar protein function--- alters myofibrillar energetics.
Case 9 A 30 y/o WM develops CHF after flu like symptoms with CP. A relatively small number of patients develop symptoms of heart failure for the first time after recovery from what appears to be a systemic viral infection. In still others, severe heart failure develops acutely during an episode of myocarditis; although some recovery occurs, chronic manifestations of diminished cardiac reserve persist and heart failure reappears months or years later. n n n Coxsackie B virus enters cardiac myocytes through the coxsackievirusadenovirus receptor and perhaps decay accelerating factor (CD 55). Initial cardiomyocyte infection results in myocyte necrosis and apoptosis with release of sequestered intracellular antigens. Some myocytes survive and harbor viral genomes. Sequestered viral genomes can result in a direct cytopathic effect of the virus. For eg. , enteroviral protease 2 a can directly cleave the myocyte cytoskeletal protein dystrophin An immune reaction develops in the heart that is comprised of antibodies against cardiac antigens and autoreactive T-lymphocytes. This contributes to myocardial dysfunction in the weeks following acute viral infection. Over months to years, chronic neurohumoral activation and hemodynamic remodeling lead to chronic dilated cardiomyopathy.
Is myocarditis the cause of Idiopathic DCM? Around 15 percent of patients with myocarditis progress to DCM. n Only around 10 percent (or less) of patients with DCM have biopsy evidence of myocarditis n Although there is the presence of high antibody viral titers, viral-specific RNA sequences, and apparent viral particles in patients with “idiopathic” DCM, the more rigorous technique of polymerase chain reaction generally has not confirmed the presence of viral remnants in the myocardium of most cardiomyopathy patients. n
n n n n n Case 10 - 55 y/o WM cirrhotic with ascites and SOB. CXR shows marked cardiomegaly- ALCOHOLIC CARDIOMYOPATHY Long-term alcohol consumption is a major cause of secondary, nonischemic DCM in the western world and accounts for upward of one third of all cases of DCM. ACM is lower in women compared to men Alcoholics in their late 40 s. 90 g/d or more than eight drinks per day for > 5 years are at risk for the development of ACM. Women may be more vulnerable ACM develops in women with a less total lifetime exposure to alcohol compared to men. There is an asymptomatic stage of ACM that, characterized by LV dilation, increased LV mass, diastolic dysfunction and wall thinning. The symptomatic ACM stage develops in those who continue to drink and is characterized by pronounced LV dilation, increased LV mass, wall thinning, systolic dysfunction, and signs and symptoms of heart failure. Treatment of both groups of ACM patients should include alcohol abstinence which may lead to reversal, and symptomatic patients should be treated with recommended heart failure pharmacotherapies.
The pathophysiology of ACM is complex and may involve cell death (possibly due to apoptosis) and changes in many aspects of myocyte function. Changes in mitochondrial, sarcoplasmic reticulum, contractile protein, and calcium homeostasis culminate in intrinsic cell dysfunction The consumption of alcohol may result in myocardial damage by three basic mechanisms: n (1) a presumed direct toxic effect of alcohol or its metabolites; n (2) nutritional effects, most commonly in association with thiamine deficiency that leads to beri heart disease n (3) rarely, toxic effects due to additives in the alcoholic beverage (cobalt) There had been speculation that alcohol caused myocardial damage only through dietary deficiencies, but it is now clear that alcoholic cardiomyopathy occurs in the absence of nutritional deficiencies. n The distinguishing features of each include peripheral vasodilatation and high-output heart failure, often right sided, in beri and reduced contractility with typically leftsided low-output failure in the latter. n May depend on the level, duration, and consistency of the person's drinking. Furthermore, in women, it is unknown as to how the incidence and pathophysiology of ACM is influenced by estrogen. Interindividual variations in the sensitivity of the myocardium to alcoholinduced myocardial damage, may be a multifactorial disease in which environmental and/or genetic traits influence the occurrence, pathogenesis, and progression of disease. Investigators found that 40% ACM patients in a study had multiple-point m. DNA mutations which are associated with the occurrence of some cardiomyopathies. Further research is needed to identify these vulnerable patients. n n
n n n a standard drink contains approximately 12 g of alcohol 12 fluid oz or 340 m. L of beer (5% v/v), 5 fluid oz or 142. 2 m. L of wine (12. 5% v/v), and 1. 5 fluid oz or 42. 6 m. L of 80 -proof (40% v/v) spirits/liquor. two thirds of the adult population use alcohol to some extent, and more than 10 percent are heavy users National Institute on Alcoholism and Alcohol Abuse has recommended that men drink no more than 14 drinks per week or no more than 4 drinks on any given occasion, and women should drink no more than 3 drinks on any given occasion and no more than 7 drinks per week. n In the United States, moderate drinking is defined as no more than one standard drink per day for women and two standard drinks per day for men, as well as anything less than this amount. n n n COBALT CARDIOMYOPATHY A previously unrecognized syndrome of severe congestive heart failure appeared in the mid 1960 s, first in Canada and subsequently in the United States and Europe. The disease was found in people who drank a particular brand of beer to which cobalt sulfate had been added as a foam stabilizer. Since cobalt was removed from the process, no more cases of the disease have been reported. On very rare occasions occupational exposure to cobalt may result in myocardial damage and attendant congestive heart failure.
n n n n n PHYSICAL EXAMINATION Examination usually reveals variable degrees of cardiac enlargement and findings of congestive heart failure. The systolic blood pressure is usually normal or low, and the pulse pressure is narrow, reflecting a diminished stroke volume. Pulsus alternans is common when severe left ventricular failure is present. Cheyne-Stokes breathing may be present and is associated with a poor prognosis. The jugular veins are distended when right-sided heart failure appears, but on initial presentation most patients do not have evidence of this. Prominent a and v waves may be visible. Grossly pulsatile jugular veins with prominent regurgitant waves indicate the presence of tricuspid valvular regurgitation; this is usually a late and often ominous finding. The liver may be engorged and pulsatile. Peripheral edema and ascites are present when right-sided heart failure is advanced. The precordium usually reveals left and, occasionally, right ventricular impulses, but the heaves are not sustained as they are in patients with ventricular hypertrophy. The apical impulse is usually displaced laterally, reflecting left ventricular dilatation. A presystolic a wave may be palpable on occasion and is generated in a similar manner as a presystolic (S 4 ) gallop heard on auscultation. The second heart sound (S 2 ) is usually normally split, although paradoxical splitting may be detected in the presence of left bundle branch block, an electrocardiographic (ECG) finding that is not unusual in DCM. If pulmonary hypertension is present, the pulmonary component of S 2 may be accentuated and the splitting may be narrow. Presystolic gallop sounds (S 4 ) are almost universally present and often precede the development of overt congestive heart failure. Ventricular gallops (S 3 ) are the rule once cardiac decompensation occurs, and a summation gallop is heard when there is concomitant tachycardia. Systolic murmurs are common and are usually due to mitral or, less commonly, tricuspid valvular regurgitation. Mitral regurgitation results from enlargement and abnormal motion of the mitral annulus; ventricular dilatation with resultant distortion of the geometry of the subvalvular apparatus (“papillary muscle dysfunction”) plays a lesser role. Gallop sounds and regurgitant murmurs can often be elicited or intensified by isometric handgrip exercise with its attendant enhancement of systemic vascular resistance and impedance to left ventricular outflow. Systemic emboli resulting from dislodgement of intracardiac thrombi from the left atrium and ventricle and pulmonary emboli that originate in the venous system of the legs are common late complications.
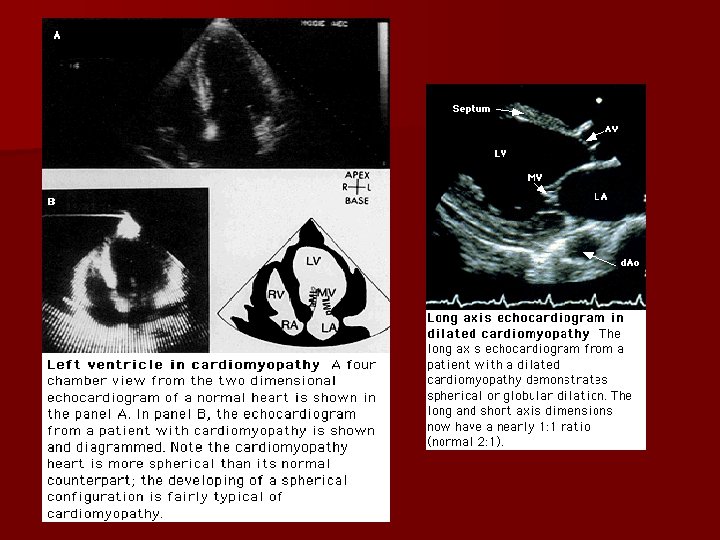
Pathology MACROSCOPIC EXAMINATION. n This reveals enlargement and dilatation of all four cardiac chambers; the ventricles are more dilated than the atria. Although the thickness of the ventricular wall is increased in some cases, the degree of hypertrophy often is less than might be expected given the severe dilatation present. The development of left ventricular hypertrophy appears to have a protective or beneficial role in DCM, presumably because it reduces systolic wall stress and thus protects against further cavity dilatation. The cardiac valves are intrinsically normal, and intracavitary thrombi, particularly in the ventricular apex, are common. The coronary arteries usually are normal. The right ventricle is preferentially involved in some cases of DCM, sometimes on a familial basis. n Gross pathology of dilated cardiomyopathy. Prominent ventricular dilatation is apparent in this heart, which has been opened so that the interior of the left ventricle can be seen. Wall thickness is normal, but the shape of the heart has become more globular. n (From Kasper EK, Hruban RH, Baughman KL: Idiopathic dilated cardiomyopathy. iInr Abelmann WH, Braunwald E ; obeds. ; cb: Atlas of Heart Diseases. Vol 2. Cardiomyopathies, Myocarditis, and Pericardial Disease. Philadelphia, Current Medicine, 1995, pp 3. 18
Pathogenesis Hypotheses to explain the pathogenesis of dilated cardiomyopathy. MHC=myosin heavy chain. (From Mestroni L, Krajinovic M, Severini GM, et al: Familial dilated cardiomyopathy. Br Heart J 72: S 35, 1994. )
DIAGNOSTICS LABS • serum phosphorus (hypophosphatemia) • serum calcium (hypocalcemia) • serum creatinine and urea nitrogen (uremia) • thyroid function studies (hypothyroidism and hyperthyroidism) • iron studies (hemochromatosis) • HIV is an important and often unrecognized cause of CHF CHEST X RAY n generalized cardiomegaly n pulmonary vascular redistribution n interstitial and alveolar edema are less common on initial presentation n Pleural effusions may be present n azygos vein and superior vena cava may be dilated when right-sided heart failure supervenes.
XRAY COMPARISON
NONINVASIVE LABORATORY EXAMINATIONS. EKG Rate/Rhythm - sinus tachycardia when heart failure is present - entire spectrum of atrial and ventricular tachyarrhythmias n Ambulatory monitoring demonstrates the ubiquity of ventricular arrhythmias, with about half of monitored patients with DCM exhibiting nonsustained ventricular tachycardia. n There is no consensus that complex or frequent ventricular arrhythmias predict sudden (presumably arrhythmic) death, although they do appear to predict total mortality. Perhaps ventricular arrhythmias as detected on ambulatory monitoring are a marker for the extent of myocardial damage in DCM and therefore associated with sudden death without necessarily being its cause n In occasional cases, particularly in children, recurrent and/or incessant supraventricular or ventricular tachyarrhythmias may actually be the cause (rather than the result) of ventricular dysfunction - restoration of sinus rhythm or slowing of the heart rate may reverse the cardiomyopathy n Poor R wave progression and intraventricular conduction abnormalities, especially left bundle branch block, are common. n Anterior Q waves may be present when there is extensive left ventricular fibrosis, even without a discrete myocardial scar or evidence of coronary artery disease. n ST segment and T wave abnormalities are common
Echocardiography Degree of impairment of left ventricular function For excluding concomitant valvular or pericardial disease size of the ventricular cavity thickness of the ventricular walls. Doppler studies are useful in delineating the severity of mitral (and tricuspid) regurgitation n Combining echocardiography with dobutamine infusion may identify patients with left ventricular dysfunction due to coronary artery disease. n Thallium-201 imaging may be helpful in distinguishing left ventricular enlargement caused by DCM from that caused by coronary artery disease n Scanning with gallium or antimyosin antibody may help to identify patients more likely to have evidence of myocarditis on biopsy n n n Radionuclide Ventriculography Radionuclide ventriculography reveals increased end-diastolic and end-systolic left ventricular volumes, reduced ejection fraction in one or both ventricles, and wall motion abnormalities); it is used most commonly when echocardiography is technically suboptimal. Like echocardiography, it may demonstrate segmental wall motion abnormalities in DCM even in the absence of coronary artery disease, the disease process that most commonly produces regional dysfunction.
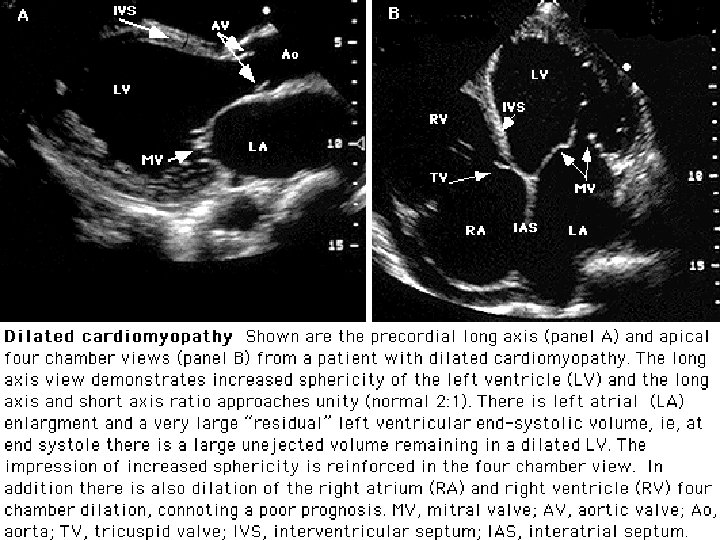
n Transthoracic two-dimensional echocardiogram recorded in a patient with a dilated cardiomyopathy. The left panel is an apical four-chamber view showing dilation of all four cardiac chambers. Note that the mitral valve protrudes into the left ventricular cavity during systole consistent with papillary muscle dysfunction (arrows). There is also incomplete closure of the tricuspid valve due to annular dilation. The two right panels were recorded in a short-axis view in diastole (top) and systole (bottom). Note again the dilated right ventricle in the severe systole dysfunction with global hypokinesis of both chambers when diastolic and systolic frames are compared.
n n n n n CARDIAC CATHETERIZATION AND ANGIOCARDIOGRAPHY. Only certain patients with DCM require cardiac catheterization (particularly those with chest pain and a suspicion of ischemic disease or patients thought to have a treatable systemic disease such as sarcoidosis or hemochromatosis, where myocardial biopsy is an important part of the catheterization procedure) Left ventricular end-diastolic, left atrial, and pulmonary artery wedge pressures usually are elevated. Modest degrees of pulmonary arterial hypertension are common. Advanced cases may demonstrate right ventricular dilatation and failure as well, with resultant elevation of the right ventricular end-diastolic, right atrial, and central venous pressures. Left ventriculography demonstrates enlargement of this chamber, typically with diffuse reduction in wall motion. Segmental wall motion abnormalities may simulate the angiographic findings in ischemic heart disease. However, prominent localized wall motion disturbances are more characteristic of ischemic heart disease, whereas diffuse global dysfunction is more typical of DCM. The ejection fraction is reduced and the end-systolic volume is increased as a result of the impairment of left ventricular contractility. Sometimes left ventricular thrombi may be visualized within the left ventricle as intracavitary filling defects. Mild mitral regurgitation is often present. On occasion, it may be difficult to distinguish left ventricular dilatation secondary to severe mitral regurgitation due to intrinsic mitral valve disease from DCM with secondary mitral regurgitation.
Coronary arteriography usually reveals normal vessels, although coronary vasodilatory capacity may be impaired (may relate to marked elevation of the left ventricular filling pressures). n This examination may be of particular value in excluding coronary artery disease in patients with abnormal Q waves on the ECG or regional left ventricular wall motion abnormalities on noninvasive evaluation (although noninvasive testing, including electron-beam computed tomography [CT], may be sufficiently reliable to exclude important coronary artery disease without resorting to arteriography) n Coronary arteriography, when necessary, thus helps to distinguish between myocardial infarction as a result of obstructive coronary artery disease and extensive localized myocardial fibrosis secondary to severe DCM in the absence of coronary artery obstruction. n
Endomyocardial Biopsy n Using a flexible bioptome, the clinician may obtain tissue samples from the right ventricle (and left ventricle when required) through a transvenous (or transarterial) approach with ease and safety n Endomyocardial biopsy results in a small tissue sample (average size 1 to 2 mm), and multiple samples (usually four or more) are required because pronounced topographical variations may be found within the myocardium. n Although on occasion endomyocardial biopsy may identify a specific etiological agent in an individual patient with cardiac disease of uncertain cause, the clinical utility of routine biopsy in cardiomyopathy is limited. It has been estimated that a specific etiological diagnosis is obtained by biopsy in fewer than 10 percent of patients with cardiomyopathy and a treatable disease is found in only about 2 percent. n The sensitivity of endomyocardial biopsy is at best around 35%. . n n DALLAS CRITERIA. Interpretation of biopsy specimens had been plagued by a high degree of interobserver variability the adoption of a generally accepted set of histological definitions, the Dallas criteria, has improved agreement. It is hoped that newer immunohistochemical and molecular biological techniques (such as the polymerase chain reaction or in situ hybridization techniques to detect viral infection of the heart) may expand further the diagnostic utility of endomyocardial biopsy A recent clinical trial has suggested that immunoperoxidase staining for human leukocyte antigen expression on endomyocardial biopsy can identify patients who will benefit from targeted immunomodulatory therapy n n n
CLINICAL INDICATIONS FOR ENDOMYOCARDIAL BIOPSY n n n DEFINITE Monitoring of cardiac allograft rejection Monitoring of anthracycline cardiotoxicity Infiltrative diseases- hemochromatosis, amyloidosis etc. n n n POSSIBLE Detection and monitoring of myocarditis Diagnosis of secondary cardiomyopathies Differentiation between restrictive and constrictive heart disease n n n UNCERTAIN Unexplained, life-threatening ventricular tachyarrhythmias Acquired immunodeficiency syndrome Formulation of prognosis in idiopathic dilated cardiomyopathy From Mason JW, O'Connell JB: Clinical merit of endomyocardial biopsy. Circulation 79: 971, 1989. Copyright 1989, American Heart Association.
morphological, ultrastructural, or microbiological marker that might be used to establish the diagnosis of idiopathic DCM or to clarify its cause Histological specimens obtained by right ventricular endomyocardial biopsy. A, Idiopathic dilated cardiomyopathy with varying degrees of interstitial fibrosis and myocyte hypertrophy (trichrome stain, 210×). B, Myocarditis with dense focal area of mononuclear cell infiltrate adjacent to necrotic and degenerating myocytes, with irregular myocytic hypertrophy and dense interstitial fibrosis (hematoxylin-eosin, 210×). (From Dec GW, Fuster V: Idiopathic dilated cardiomyopathy. N Engl J Med 331: 1564, 1994. Copyright 1994, Massachusetts Medical Society. ) (From Dec GW, Fuster V: Idiopathic dilated
PROGNOSIS A variety of clinical predictors of patients at enhanced risk of dying of DCM have been identified n protodiastolic (S 3 ) gallop n ventricular arrhythmias n advanced age n specific endomyocardial biopsy features (such as loss of intracellular myofilaments) The predictive reliability of any single feature is not high. The clinical course is largely unpredictable in the individual patient and may depend in part upon the cause of the heart disease. There also disease-independent predictors of survival n New York Heart Association functional class n left ventricular ejection fraction maximal oxygen consumption. Cardiopulmonary exercise testing also can provide prognostic information. Marked limitation of exercise capacity manifested by reduced maximal systemic oxygen uptake (especially when below 10 to 12 ml/kg/min- normal 20 ml/kg/min) is a reliable predictor of mortality and is used widely as an indicator for consideration of cardiac transplantation. n These prognostic determinants assume that the cause of the myocardial dysfunction cannot be treated n Greater ventricular enlargement and worse dysfunction tend to correlate with poorer prognosis particularly if the right ventricle is also dilated and dysfunctional. n LA enlargement has an independent and additional prognostic value in elderly patients(>70 yrs) with LV dysfunction n
ement Manag Because the cause of idiopathic DCM, by definition, is unknown, specific therapy is not possible. Treatment, therefore, is for heart failure. n Regular physical exercise (as tolerated) increases exercise capacity by improving endothelial dysfunction and augmenting blood flow in skeletal muscles. Exercise training improves exercise tolerance and LV function. This is accompanied by a decrease in biventricular oxidative metabolism and enhanced forward work efficiency. Therefore, exercise training elicits an energetically favorable improvement in myocardial function and exercise tolerance in patients with DCM. n Diet- low salt, low fat, heart healthy n Only cardiac transplantation and specific pharmacological therapy (the vasodilators enalapril or hydralazine plus nitrates, the beta-adrenoceptor blocker carvedilol, and the aldosterone receptor blocker spironolactone) have been shown to prolong life.
BETA-ADRENERGIC RECEPTOR BLOCKADE n n n n (1) negative chronotropic effect with reduced myocardial oxygen demand (2) reduced myocardial damage due to catecholamines (3) improved diastolic relaxation (both early active and late passive properties) (4) inhibition of sympathetically mediated vasoconstriction (5) increase (“upregulation”) in myocardial beta-adrenoceptor density (6) improved calcium handling at slower heart rates, (7) modulation of postreceptor inhibitory G proteins, and/or (7) a direct effect on myocyte and interstitial growth, with attendant inhibition of the remodeling process (remodeling refers to the change in ventricular shape, size, and geometry that occurs after myocyte dysfunction). n The use of beta-blockers in patients with heart failure has been shown to improve overall mortality considerably This survival benefit has been demonstrated for bisoprolol, metoprolol and carvedilol. Therefore, one of these three beta-blocking agents should be administered routinely starting with low doses in all patients with New York Heart Association (NYHA) class II or III heart failure in addition to ACE inhibitors, unless there is a contraindication to beta-blocker use. n In addition, NYHA class IV heart failure patients have been shown to benefit from carvedilol therapy, if tolerated. n Beta-adrenergic blocker therapy is now accepted as part of the four-drug approach (along with digoxin, vasodilators and diuretics) advocated for all suitable patients with symptomatic congestive heart failure. n Despite routine use of angiotensin-converting enzyme (ACE) inhibitors, beta-blockers and spironolactone in patients with heart failure due to dilated cardiomyopathy (DCM), these patients still have a considerable annual mortality rate of 5 -10%. n Patients with advanced heart failure or in a decompensated state should not ordinarily be given a betaadrenergic blocker for fear of worsening the failure.
n CALCIUM ANTAGONISTS. n Because of the possible link between DCM, microvascular circulatory abnormalities, and abnormal myocardial calcium handling, there has been interest in the use of calcium antagonists. These agents have generally been well tolerated when used in DCM patients, although myocardial depression is an important potential side effect of the calcium antagonists as a group. Unfortunately, combining a calcium antagonist with traditional standard therapy (digoxin, diuretics, and vasodilator) does not appear to have substantial clinical benefit, nor does it reduce further the mortality in DCM. At present, the routine use of calcium antagonists in DCM is considered nonstandard and not first-line therapy. n ANTIARRHYTHMICS. n Sudden unexpected death accounts for up to 50% of all deaths and is most often due to rapid ventricular tachycardia or ventricular fibrillation and less often due to bradyarrhythmias or asystole n Although there is no definitive evidence that antiarrhythmic agents prolong life or prevent sudden death in DCM it may be appropriate to use them in the treatment of symptomatic arrhythmias. The conflicting results of GESICA and CHF-STAT studies do not support a strategy of "prophylactic" amiodarone therapy in patients with DCM in order to prevent sudden cardiac death. The implantable cardioverter-defibrillator should be considered in appropriate candidates with symptomatic ventricular tachyarrhythmias n Even patients with unexplained syncope and no demonstrated tachyarrhythmia (even during electrophysiological testing) may profit from the insertion of an ICD. n
n n ANTICOAGULANTS. There is a lack of agreement as to the appropriateness and usefulness of chronic anticoagulant therapy in DCM to protect against pulmonary and especially systemic emboliand heart failure. There is general agreement that anticoagulants should be used in the presence of atrial fibrillation, if the patient has previously had a stroke, and when there is visible thrombus on echocardiography. Oral warfarin is used to achieve a prolongation of the prothrombin time of 2. 0 to 3. 0 international normalized ratio. n n IMMUNOSUPPRESSIVES. In those patients with chronic heart failure secondary to DCM and lymphocytic infiltrate on myocardial biopsy, treatment with corticosteroids and immunosuppressive agents had been advocated in the past. Unfortunately, such therapy does not appear to have a clinically important effect on symptoms, exercise performance, or ejection fraction (in more than just the short term) and may be associated with significant complications. Routine clinical use of immunosuppressive therapy thus cannot be recommended at present.
n n n n DUAL CHAMBER PACING. This has been used in some patients with DCM and intact atrioventricular conduction changes the sequence of ventricular depolarization reduces functional mitral regurgitation improves clinical status some symptomatic and hemodynamic improvement has been reported Patients with intraventricular conduction delay or those with disturbed timing of atrioventricular mechanical activation had maximum benefit. SURGICAL TREATMENT. Mitral annuloplasty or replacement of regurgitant valves has been attempted in some patients with DCM and prominent atrioventricular valvular regurgitation. n The results of operation are usually less than satisfactory because of the degree of preexisting cardiac dysfunction and damage, although some patients have shown some degree of symptomatic improvement, at least over the intermediate term. n n n In appropriately selected patients, cardiac transplantation may be an attractive alternative to medical therapy, with a 5 -year survival rate of about 75 percent. Surgical translocation of the latissimus dorsi muscle to wrap around the heart and augment cardiac performance (dynamic cardiomyoplasty) appears to have benefited some patients who are not otherwise suitable candidates for cardiac transplantation n Excision of part of the left ventricle (partial ventriculotomy) has been proposed as an additional surgical alternative to cardiac transplantation ; the lack of a randomized control trials has limited the widespread adoption of the procedure. n
Experimental therapies Immunohemeadsorption/LVAD the pathogenic role of immunological factors, such as cardiac autoimmune antibodies and cytokines is known. This has led to one possible new therapy, immunoadsorption, which removes antibodies, and it has made a remarkable effect. However, there are other factors to remove. n For the removal of cytokines and neurohormones, the most effective method is hemofiltration (HF). n Also, double-filtration plasmapheresis (DFPP) removes immunoglobulin as well as low-density lipoprotein (LDL) and coagulation factors that may improve blood circulation, including the coronary arteries. n Therefore, to eliminate all deteriorative factors, both apheresis therapies, HF and DFPP, should be performed. n Due to the shortage of donor hearts, left ventricular assist systems (LVAD) have been used as a bridge to transplantation. It has now been reported that the total unloading of the left ventricle does not only maintain, but also recovers, the cardiac function, even from end-stage heart failure. n However, the patients who have obtained a long-lasting recovery of cardiac function from an LVAD are still in a minority. To make this the majority, therapeutic LVAD should be combined with the apheresis therapies, DFPP and HF. n combination of HF and DFPP with therapeutic LVAD, will be the next generation of treatment that has a potential to postpone, or even avoid, heart transplants
A prospective matched-case control study examined 5 -year survival rates, n n n direct medical costs, and cost-effectiveness in Germany (n=34) from a health-care system perspective. In a cost-effectiveness analysis costs per life year gained were calculated. Patients treated with IA showed a greater survival rate: 5 -year survival rate in the intervention group was 82% vs. 41% in controls. Initial intervention costs for IA were found to be 28, 400 euro per patient treated. Direct medical costs for a 5 -year follow-up were 128, 600 euro per patient treated with IA and 75, 500 euro in controls. Considering only the actual survival time calculated annual treatment costs were 24, 900 euro in the IA group and 28, 900 euro in controls. The cost-effectiveness ratio expressed in costs per life year gained was 34, 400 euro. This is the first controlled study to perform 5 -year survival analysis and economic evaluation of this new emerging technology for patients with DCM. Although high initial treatment costs for IA are incurred, the significantly better survival rates lead to reasonable costs per live year gained. Elevated uric acid levels are associated with diastolic dysfunction in CHF. Xanthine oxydase inhibition in patients with CHF might theoretically result in an improvement of diastolic function
Growth Hormone in DCM The data from animal and human in vivo studies suggest that cardiac function is dependent in part on the normal function of the GH/IGF-1 axis (growth hormone/insulin-like growth factor-1). n So far encouraging results from phase II and III clinical trials evaluating the effects of intermittent GH treatment in patients with chronic congestive heart failure (CHF) due to dilated cardiomyopathy (DCM) have been published. n In these studies, growth hormone (i. e. , DNA-derived recombinant human growth hormone) was not used alone but in addition to standard optimal therapy for CHF. n Rationale: n According to Laplace's Law cardiac wall stress (i. e. , the force acting per unit of cross -sectional area of the ventricular wall) is directly related to intraventricular pressure and ventricular radius and inversely related to ventricular wall thickness. n Cardiac (ventricular) wall stress is increased in DCM (mainly because of the dilatation of the ventricles and to a minor extent because of the relative reduction in ventricular thickness). n GH is capable of increasing ventricular wall thickness in DCM thus reducing cardiac wall stress which in turn leads to an improvement in systolic cardiac performance. GH therapyn improved LV ejection fraction n modulates beneficially circulating cytokine network and soluble adhesion molecules in patients with DCM n enhances contractile reserve and diminishes LV volumes. n These GH-induced anti-inflammatory effects may be associated with the improvement in LV contractile performance and exercise capacity n
Discussion Should screening for DCM be done in relatives of patients with early onset/idiopathic DCM?
n According to one study, nearly one-third of asymptomatic relatives (29%) have echocardiographic abnormalities, and 27% of such relatives progress to development of overt DCM. Early identification of such people would permit appropriate intervention that might influence the serious complications and mortality of this disease. n After a study that followed first degree relatives for 10 years, it was recommended that first-degree relatives of patients undergo monitoring every 5 years with electrocardiography and echocardiography for early detection and treatment of disease as there was greater likelihood of developing dilated cariomyopathy in relatives with an enlarged left ventricle, especially in systole (7 of 42, 17%). n Conclusion: over a median follow-up period of 10 years, 7% of previously healthy first-degree relatives of patients with IDC developed IDC when a follow-up LVEF measurement was available. Of the 431 relatives with any follow-up data, regardless of whether they had a follow-up LVEF measurement, a minimum of 3% developed the disease. This is in addition to the relatives who were diagnosed at the time of the initial screening. The risk was highest for relatives with an enlarged left ventricle in systole and/or diastole.
n Should patients titrate drugs like lasix based on symptoms/weight?
n Should we supplement with thiamine, selenium, carnitine? n Cost $50 per month. Cost of biopsy? Cost of CHF treatment for life? n Can be discontinued if no reversal or progression of DCM in 6 -12 months.
Uses of carnitine n n n n L-Carnitine (carnitine) may have a role in the treatment of various cardiac disorders because of its actions on cardioprotection from hypoxia and oxidative stress. Studies on the role of carnitine administration to patients with myocardial infarction (MI), angina, and congestive heart failure generally have been positive. In general, treatment with carnitine (1. 5 to 6 g/d for up to 1 year) results in a beneficial effect of fewer deaths and less heart failure when administered to patients after MI. Compared with placebo, carnitine use resulted in smaller increases in left ventricular end-systolic and end-diastolic volumes over time. In shorter term studies (1 to 3 months), carnitine therapy may have positive effects on symptoms of heart failure and angina in the post-MI period. Carnitine also seems to improve exercise tolerance and oxygen consumption in moderate to severe heart failure. Studies specific to the dialysis population have generally shown that carnitine may have a beneficial effect on a number of cardiac parameters. Because cardiac disease is the most common form of death in patients with end-stage renal disease, these findings may be particularly important for this population. Moreover, because the relationship between conventional cardiac risk factors and cardiac disease is less clear in this population, the role of therapies that address pathological states specific to the dialysis population is worthy of study. Because a dialysis-related carnitine disorder is common among these patients, L-carnitine supplementation would be among these specific therapies.
References n Abelmann, WH. Classification and natural history of primary myocardial disease. Prog Cardiovasc Dis 1984; 27: 73. n Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. Br Heart J 1980; 44: 672. n Richardson, P (Chairman). Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of the Cardiomyopathies. Circulation 1996; 93: 841. n Dec, GW, Fuster , Idiopathic dilated cardiomyopathy. V. N Engl J Med 1994; 331: 1564. Dec, GW, Fuster, Idiopathic dilated n Devereux, R, Roman, M, Paranicas , M, et al. A population-based assessment of left ventricular systolic dysfunction in middle-aged and older adults: the Strong Heart Study. Devereux, R, Roman, M, Paranicas, M, et al. A population-based assessment of left ventricular systolic dysfunction in middle-aged and older adults: the Strong Heart Study. Am Heart J 2001; 141: 439. n Felker, CM, Thompson, RE, Hare, JM, et al. Underlying causes and long-term survival in patients with initially unexplained Engl J Med 2000; 342: 1077. Felker, CM, Thompson, RE, Hare, JM, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N Engl n Association of beta-adrenergic receptor polymorphisms and progression to heart failure in patients with idiopathic dilated cardiomyopathy. Forleo C - Am J Med - 1 -OCT-2004; 117(7): 451 -8 From NIH/NLM MEDLINE NLM Pub. Med)Am J Med. 2004 Oct 1; 117(7): 525 -7 Pub. Med ID: 15464712 - 1 -OCT-2004; 117(7): 451 -8 From NIH/NLM MEDLINE NLM Citation ID: 15464701 (Pub. Med)Am n Prognostic value of left atrial enlargement in patients with idiopathic dilated cardiomyopathy and ischemic cardiomyopathy. Dini FL - Am J Cardiol - 1 -MAR cardiomyopathy. Dini FL - -2002; 89(5): 518 -23 From NIH/NLM MEDLINE n Viral infection, inflammation, and the risk of idiopathic dilated cardiomyopathy: can the fire be extinguished? Leslie T. Cooper Jr. , MD MD a , * Bernard J. Gersh, MB, Ch. B, DPhil The American Journal of Cardiology Volume 90 • Number 7 • October 1, 2002 Copyright © 2002 The American College of Cardiology n Elevated serum uric acid levels are associated with diastolic dysfunction in patients with dilated cardiomyopathy. Cicoira M - Am Heart J - 01 -JUN-2002; cardiomyopathy. Cicoira M - 143(6): 1107 -11 From NIH/NLM MEDLINE n The role of carnitine in myocardial dysfunction. Pauly DF - Am J Kidney Dis - 01 -APR-2003; 41(4 Suppl 4): S 35 -43 dysfunction. Pauly DF - - 01 -APR-2003; 41(4 Suppl 4): S 35 -43 From NIH/NLM MEDLINE n Potential role of humoral immunity in cardiac dysfunction of patients suffering from dilated cardiomyopathy. Staudt A - J Am Coll Cardiol - 18 -AUG-2004; cardiomyopathy. Staudt A - 44(4): 829 -36 From NIH/NLM MEDLINE n Recombinant human growth hormone treatment for dilated cardiomyopathy in children. Mc. Elhinney DB - Pediatrics - 01 -OCT-2004; 114(4): e 452 -8 children. Mc. Elhinney DB - From NIH/NLM MEDLINE n [Dilated cardiomyopathy and growth hormone]Dreifuss P - Z Kardiol - 01 -DEC-2002; 91(12): 973 -7 hormone]Dreifuss P - From NIH/NLM MEDLINE
n n n Genetic predisposition to heart failure Michele Pasotti, MD a Alessandra Repetto, MD a Luigi Tavazzi, MD, FESC, FAC a Eloisa Arbustini, MD, FESC b , * Effects of growth hormone on circulating cytokine network, and left ventricular contractile performance and geometry in patients with idiopathic dilated cardiomyopathy. Adamopoulos S - Eur Heart J - 01 -DEC-2003; 24(24): 2186 -96 From NIH/NLM MEDLINE New insights into the pathogenesis of dilated cardiomyopathy: possible underlying autoimmune mechanisms and therapy. Mobini R - Autoimmun Rev - 01 -JUN-2004; 3(4): 277 -84 From NIH/NLM MEDLINE Economic evaluation and survival analysis of immunoglobulin adsorption in patients with idiopathic dilated cardiomyopathy. Hessel FP - Eur J Health Econ - 01 -FEB-2004; 5(1): 58 -63 From NIH/NLM MEDLINE Therapeutic left ventricular assist device and apheresis on dilated cardiomyopathy. Matoba Y - Artif Organs - 01 -FEB-2004; 28(2): 171 -81 Exercise training improves biventricular oxidative metabolism and left ventricular efficiency in patients with dilated cardiomyopathy. Stolen KQ - J Am Coll Cardiol - 5 -FEB-2003; 41(3): 460 -7 From NIH/NLM MEDLINE NLM Citation ID: 12575976 (Pub. Med) Sudden cardiac death in dilated cardiomyopathy -- therapeutic options. Grimm W - Herz - 01 -DEC 2002; 27(8): 750 -9 From NIH/NLM MEDLINE NLM Citation ID: 12574892 (Pub. Med) Frequency of development of idiopathic dilated cardiomyopathy among relatives of patients with idiopathic dilated cardiomyopathy Virginia V. Michels, MD a , * Timothy M. Olson, MD b, c. Fletcher A. Miller, MD c Karla V. Ballman, Ph. D d A. Gabriela Rosales, MS d David J. Driscoll, MD b Periodic rescreening is indicated for family members at risk of developing familial dilated cardiomyopathy. Crispell KA - J Am Coll Cardiol - 1 -MAY-2002; 39(9): 1503 -7 From NIH/NLM MEDLINE Alcoholic Cardiomyopathy. Incidence, Clinical Characteristics, and Pathophysiology Mariann R. Piano 1 Ph. D 1 University of Illinois at Chicago College of Nursing, Chicago, IL. Braunwald: Heart Disease: A Textbook of Cardiovascular Medicine, 6 th ed. , Copyright © 2001 W. B. Saunders Company
IMMUNOSUPRESSION AND MYOCARDITIS Randomized 84 patients with >6 months of symptoms and human leukocyte antigen expression on right ventricular endomyocardial biopsy specimens to azathioprine and steroids or placebo. They observed an improvement in left ventricular ejection fraction sustained up to 2 years in the immunosuppression group. Novel methods such as human leukocyte antigen staining or perhaps viral genome amplification are needed to identify patients at high risk for death, transplantation, or who may respond to targeted immunomodulatory or antiviral therapy. n One noninvasive test that holds great promise for the diagnosis of myocarditis is magnetic resonance imaging. Postgadolinium inversion-recovery sequence has been used successfully to image myocardial infarcts. Recent reports of the use of magnetic resonance imaging in suspected lymphocytic myocarditis suggest a high sensitivity. Freidrich et al reported a series of 44 consecutive patients with symptoms of acute myocarditis who they followed serially with thallium-weighted magnetic resonance imaging. Increased signal enhancement after gadolinium was noted focally, and later globally in the myocardium compared with controls. Patients with greater symptoms and persistent symptoms had significantly greater myocardial signal intensity. The prognostic value of magnetic resonance imaging and other noninvasive imaging tools such as radiolabeled annexin antibodies remains to be determined. n Timing in therapeutic trials is critical for the design of human studies that seek to evaluate therapy for inflammatory heart disease. In the Myocarditis Treatment Trial, all subjects had <2 years of symptoms, and the mean duration of symptoms was 1 month. The ejection fraction for the whole cohort increased 9%, regardless of immunotherapy. In the Intervention in Myocarditis and Acute dilated Cardiomyopathy (IMAC) trial, patients were enrolled with an ejection fraction <40% and <6 months of symptoms. In that cohort, the ejection fraction increased 14% regardless of immunoglobulin treatment. In contrast to the Myocarditis Treatment Trial cohort, most of these patients were on β blockers. These data suggest that patients with recent-onset dilated cardiomyopathy (who are well enough to be enrolled in a trial) tend to improve with standard care. Perhaps the greatest benefit of immunomodulatory or antiviral therapy is to be found in those patients who fail to clear infection or have persistent myocardial inflammation after the acute illness. The key question is how do we identify them. n The time is ripe for a multicenter study to investigate the prognostic value of novel serologic markers and imaging modalities for acute and ongoing inflammatory heart disease. Prime candidates include human leukocyte antigen expression on biopsy, noninvasive imaging with magnetic resonance imaging or radiolabeled annexin antibody, and serologic tests including s. Fas, s. Fas. L and ultra-sensitive troponin. An objective of this study would be to establish a new “gold standard” for myocarditis based on our current understanding of the pathogenesis of myocardial damage and dysfunction is needed. Obstacles to this effort include a lack of standardization across institutions for the tissue collection, processing, and protocols for the detection of viral genome from endomyocardial biopsy specimens. n Today, the clinician faced with suspected myocarditis can only state the same data that was gathered 15 years ago: namely, that about 1/3 of patients improve, 1/3 stabilize, and 1/3 deteriorate clinically despite optimal conventional care. Now is the time to use the advances of the past decade to better identify patients who will not improve with conventional care. Once identified, this will constitute the “high-risk” population to target for promising new treatments
n ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHY n This unique cardiomyopathy (which is also called arrhythmogenic right ventricular dysplasia [ARVD]) is marked by myocardial cell loss with partial or total replacement of right ventricular muscle by adipose and fibrous tissue; apoptosis appears to be a principal cause of the cell death ARVD is associated with reentrant ventricular tachyarrhythmias of right ventricular origin (producing a left bundle branch block configuration of the QRS complex) and the risk of sudden death. In about one third of the cases there is autosomal dominant inheritance of the disease, and several distinct genetic mutations have been reported. [One variant, found on the Greek island of Naxos, is inherited as a recessive trait but with a high degree of penetrance. n ARVD appears to be distinct from Uhl disease, which is marked by extreme thinning of the ventricular wall. The diagnosis is based on a constellation of clinical, ECG, histological, and echocardiographic findings. Typical clinical features include male predominance, normal physical examination, inverted T waves in the right precordial ECG leads, symptoms of palpitations and syncope, and a risk of sudden death. In some patients with ventricular arrhythmias of no evident cause, clinically subtle right ventricular dysplasia may be etiological. Noninvasive and invasive evaluation demonstrate a dilated, poorly contractile right ventricle, usually with a normal left ventricle, although some degree of left ventricular dysfunction has been seen. Magnetic resonance imaging (MRI) shows promise for identifying patients with this condition. Antiarrhythmic therapy, especially with beta-adrenoceptor blockers, sotalol, or amiodarone, often is effective in controlling the arrhythmias. The arrhythmias may be related to abnormalities of regional right ventricular sympathetic innervation, or impaired presynaptic catecholamine reuptake, as has been demonstrated by noninvasive scintigraphy. Cryo- or catheter-based radiofrequency ablation of the presumed arrhythmogenic focus has been successful in resolving the ventricular arrhythmia in some patients unresponsive to or intolerant of antiarrhythmic drug therapy. Insertion of an ICD or cardiac transplantation is reserved for recalcitrant cases. n