Periradicular Periapical Diseases Introduction u Periradicular tissues consist









 –")










- Slides: 22
Periradicular/ Periapical Diseases
Introduction u Periradicular tissues consist of cementum, periodontal ligament, and alveolar bone. u The response of the periradicular tissues to various injuries is similar to that of other connective tissues elsewhere in the body- an immuno inflamatory response
Apical Periodontitis u Apical Periodontitis is a inflammatory lesion in the periodontal tissues that is caused mostly by bacterial elements derived from the infected root canal system of teeth. u Other causes: – Physical (overinstrumentation, overfilling) – Chemical (irrigants, intracanal medication, root canal filling materials) insults – traumatic injury
Prevalence of AP u Epidemiologic study of apical periodontitis documents that the prevalence of apical periodontitis varies among patients aged u 20 to 30 (33%), u 30 to 40 (40%), u 40 to 50 (48%), u 50 to 60 (57%), u ≥ 60 years of age (62%)
Types of apical periodontitis u Asymptomatic apical periodontitis u Symptomatic apical periodontitis u Acute apical abscess u Chronic apical abscess u Cellulitis u condensing osteitis
Histological classification u On a microscopic level, different structural frameworks of apical periodontitis can be identified. u These forms include: u Apical granuloma, u Apical abscess and u Apical cyst.
Apical granuloma Most common form of apical periodontitis and consists of an inflammatory lesion dominated by lymphocytes, macrophages and plasma cells u Numerous fibroblasts and connective tissue fibers are usually present with abundant capillaries u Epithelial cell proliferation is a common finding in longstanding apical granulomas and may occur in up to 50% of the lesions u
Apical abscess u Denotes the presence of pus within the lesion. u Abscess formation may reflect a shift in cellular dynamics within a preexisting apical granuloma or be a direct outcome of an acute primary infection
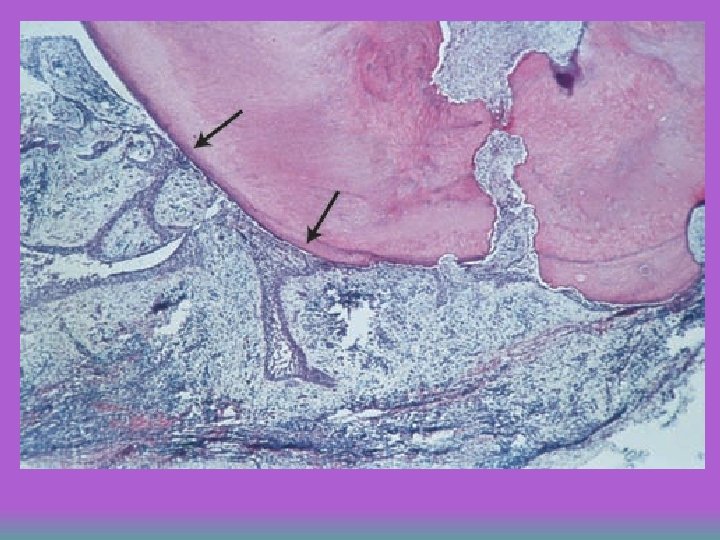
Apical Cyst u An epithelium-lined cavity that contains fluid or semi-solid material and is commonly surrounded by dense connective tissue variably infiltrated by mononuclear leukocytes and PMNs. u Cyst cavity is most commonly lined with stratified squamous epithelium of varying thickness that originates from the epithelial rest cells of Malassez
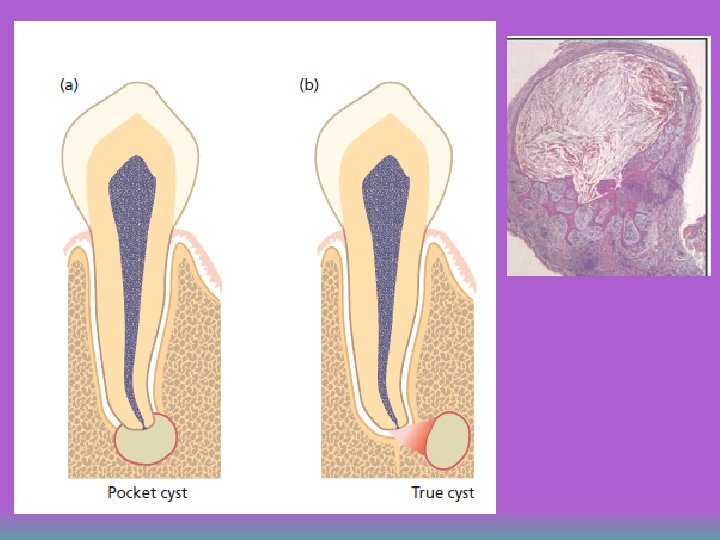
Apical cyst u Apical cysts are divided into – Pocket Cysts (Bay Cyst) – True Cysts A pocket cyst is an apical inflamatory saclike, epithelium lined cavity that is open to and continuous with the root canal space. u True apical cysts are located within the periapical granuloma with no apparent connection between their cavity and that of the root canal space u
Lining of a periapical cyst. Stratified squamous epithelium.
Mechanism of Apical Cyst u Two main theories were proposed. – The “nutritional deficiency” theory – The “abscess” theory u The exact mechanism of cyst formation in periapical inflammatory lesions has been the subject of much debate. u. A multitude of factors are involved: increased osmotic tension, decreased nutrition, release of bone-resorbing factors and other inflamatory mediators.
Symptomatic AP u History -symptoms of pulpitis or necrosis + pain on bite u Clinical examination: – pain on percussion u X-ray: – thickening of periodontal ligament space u Treatment: – root canal treatment, (adjustment of occlusion)
Asymptomatic AP u u asymptomatic apical periodontitis may go unnoticed by the patient and is often discovered only by routine radiographic examination or by careful patient history. History : – asymptomatic or slight discomfort u Clinical examintaion: – little or no pain on percussion u X-ray: – interruption of lamina dura or apical radiolucency u Treatment: – root canal treatment
Acute apical abscess u History: – severe discomfort, swelling, fever u Clinical examination: – swelling, localisation? u X-ray: – interruption of lamina dura or apical radiolucency u Treatment: – root canal treatment, drainage, (antibiotics)
Common pathways of an apical abscess.
Chronic apical abscess u History: – asymptomatic or slight discomfort – A sinus tract is the typical feature of the chronic apical abscess. u Clinical examintaion: – little or no pain on percussion u X-ray: – radiolucent lesion (localisation) u Treatment: – root canal treatment
Examples of various routes of draining of a chronic apical abscess to the oral environment: (a) through the alveolar bone; (b) along the periodontal ligament.
Cellulitis Symptomatic oedematous inflammation associated with diffuse spreading of invasive microorganisms through connective tissue and fascial planes. u Clinical examintaion: u – diffuse swelling of facial or cervical tissues. u Complications: Cases of – Ludwig’s angina, – Orbital cellulitis – Cavernous sinus thrombosis – Brain abscess
Condensing osteitis A diffuse radiopaque lesion believed to represent a localized bone reaction to a lowgrade inflammatory stimulus, usually seen at an apex of a tooth (or its extraction site) in which there has been a longstanding pulp disease. u Characterized by overproduction of bone in the periapical area, mostly around the apices of mandibular molars and premolars that had longstanding chronic pulpitis u