Controversies in renal arterial interventions ACHILLES CHATZIIOANNOU MD

 • 3 anti-HTN medications •")

 • Classic studies by Goldblatt (1930): RAS is the cause of")

 • Young patients –more commonly females. • Medial fibroplasia (80%). •")

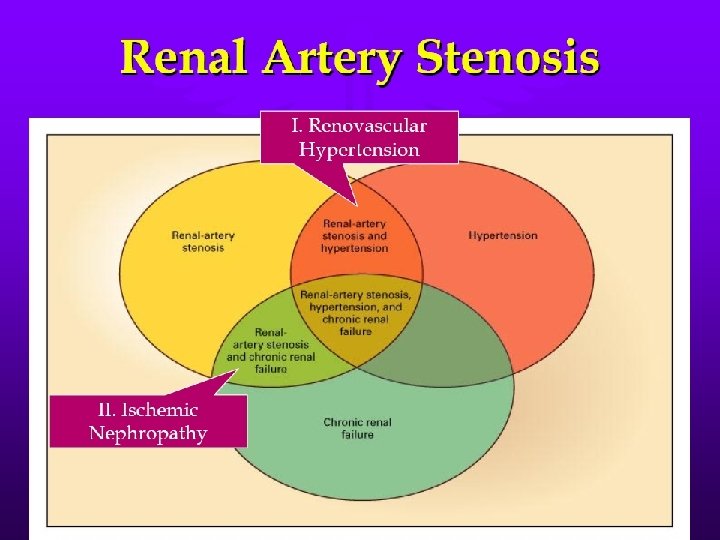
 Renal Artery Stenosis Incidental RAS Renovascular Hypertension")
 is always indicated in RAS? • 7660 interventions in 1996 •")


. 1. Progressive nature")



















")
























- Slides: 62
Controversies in renal arterial interventions. ACHILLES CHATZIIOANNOU, MD Assoc. Professor of Radiology American Board of Radiology
• 60 -year old male. • Hypertension (180/100) • 3 anti-HTN medications • Cr: 2, 1 mg/dl
• Normotensive • Cr=1. 1 mg/dl with one medication. Herculink 6 X 18 -mm
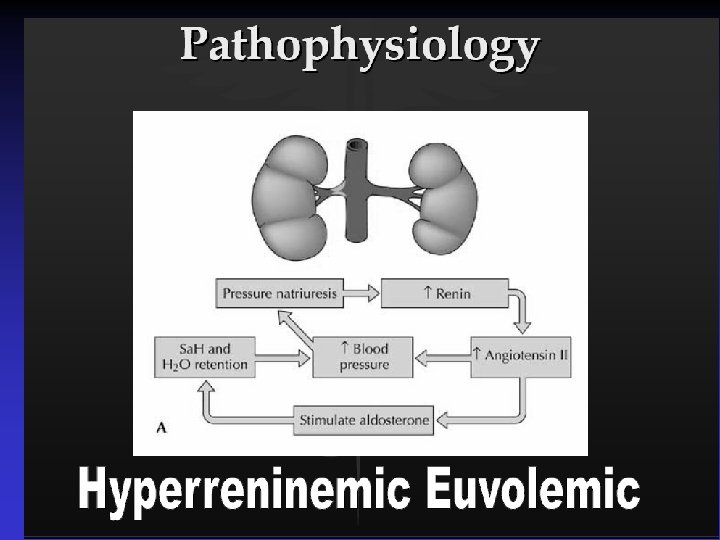
Renovascular Hypertension (RVH) • Classic studies by Goldblatt (1930): RAS is the cause of RVH. • RAS causing RVH: prevalence 3 -5% of the hypertensive patients. • Atherosclerosis: 70 -90% of RHV. FMD: 10 -30% of RVH.
Atherosclerotic disease • The prevalence of RAS is increasing because of population aging, and increased survival. • >60% RAS in 6. 8% of individuals > 65 y. • RAS in pts undergoing coronary DSA: 18%20%. • RAS in pts undergoing peripheral DSA: 35%50%.
Fibromuscular Dysplasia (FMD) • Young patients –more commonly females. • Medial fibroplasia (80%). • Location: distal main renal artery, 25% into 1 st order branches. • >50% of patients have bilateral disease. • Commonly asymptomatic (3%-6% in Transplant donors).
Atherosclerotic disease • Patient 6 th decade or older. • More often male. • The majority of the lesions are incidental findings. • Ostial lesions: within 1 -cm from aorta. • Truncal lesions (less than 10%): more than 1 -cm. • 50% have bilateral disease. • 12%-20% of stenoses>75% will progress to total occlusion within one year (? )
Manifestations of Renovascular Disease (Textor SC, 2004) Renal Artery Stenosis Incidental RAS Renovascular Hypertension Ischemic Nephropathy Accelerated CV Disease CHF Stroke
Endovascular treatment (PTA-stents) is always indicated in RAS? • 7660 interventions in 1996 • 18520 interventions in 2000 • 2. 8 -fold increase by interventional cardiologists (“drive-by”). Medicare data
Why should we NOT treat RAS whenever found? • Complication rates: 13%-24%. • Procedure-related mortality: 2%. • Worsening of renal function (cholesterol embo). • Restenosis: 11%-25%.
Indications for revascularization in RAS When should we proceed to revascularization if a patient has RAS?
Treat RAS whenever found (easier when early, avoid progression to occlusion). 1. Progressive nature of ARVD, progressing at the rate of 10% per year (45%-60% progression rate in 47 year f-u) 2. Pre-occlusive lesions (70 -90%): risk of occlusion 40%. . JVIR 2002
Is there a role for “prophylactic” treatment of hemodynamically significant RAS in pts with normal RF, normotensive, or with easily controlled HTN? NO
Renal artery stenting can treat patients with RAS and hypertension • In FMD: HTN cured in 40%; improved in 51%; cumulative benefit 87%@10 years. • In ARVD: cure 11%; improvement 54% [PTA meta-analysis incl 895 pts]. • Use of stents: benefit in 71% [300 pts Lederman]; benefit in 43%-54% [163 pts Dorros].
Ischemic nephropathy • Kidney damage secondary to RAS. • Not true “ischemia”, rather renal hypoperfusion with impaired nephron function. • RAS is present in 22% of patients >50 years entering dialysis.
Ischemic nephropathy • Progressive disease – Lesion progression 20% per year. – Renal atrophy 10% per year. – Artery occlusion 5% per year. • RAS is a marker of increased cardiovascular mortality, predictors: – Older age – Impaired renal function – Bilateral RAS
Acute renal failure in patients with RAS • 1 -14 days after the initiation of treatment with ACE inhibitors. • After the use of diuterics or other antihypertensive drugs. • After major surgery. • After the spontaneous progression of RAS to total occlusion.
Results of revascularization for ischemic nephropathy • 32 patients with unexplained renal impairment and RAS were treated with renal artery stent. • In 70% of the patients the renal function improved or stabilized (p<0. 007). Harden et al, Lancet 1997
Results of revascularization for ischemic nephropathy • 33 patients with bilateral RAS or RAS in solitary kidney. • Follow up: 20± 11 months. • Significant improvement in 72%; mild improvement in 28%. • Preservation of renal size in all patients. Watson et al. Circulation 2000
Signs that a patient with ischemic nephropathy will benefit from revascularization 1. Normal distal arterioles. 2. Bilateral disease. 3. Recent onset of renal insufficiency. 4. Resistive Index (Doppler sonography) <80 5. Extremely limited renal function (cr>2, 5 mg/dl or 220 μmol/l)* • *Uder M, Huke U CVIR 2005
Percutaneous • Technical success: 98 -100% revascularization • Long term patency rate 85%-98% • Complications: – Mortality 1 -3% – Major complications: 3 -5% – Minor complications 10 -20%
An analysis of the pooled results of studies of • conventional balloon angioplasty in 1118 Hospital death 0. 5% patients • Nephrectomy 0. 3% • Renal surgery 2% • Occlusion of a side branch of the renal artery 2. 2% • Cholesterol embolization 1. 1% • Injury at the site of vascular access 2. 3% The indications and results of PTA and stenting in renal artery stenosis. Semin. Vasc Surg 1996; 9: 188 -197
Evidence 3 randomized controlled trials compared medical treatment to percutaneous renal revascularization: • DRASTIC: Dutch Renal Artery Stenosis Intervention Cooperative Study Group • EMMA: Essai Multicentrique Medicaments vs Angioplastie Study Group • SNRASCG: Scottish and Newcastle Renal Artery Stenosis Collaborative Group
Systolic and Diastolic BP • SNRASCG : no difference • EMMA: no significant difference • DRASTIC: no significant difference • 7%(4 patients) in the PTA group vs. none in the medical treatment group had cure of their HTN • In the patients that underwent PTA from medical treatment group due to refractory HTN or progressive renal dysfunction: there was a significant decrease in BP (P<0. 001) • Nordman. Cochrane Library of Systematic Reviews. 2004: ; vol 2
Number of Antihypertensive Agents • SNRASCG : no difference • EMMA: significant decrease in the defined daily dose of antihypertensive agents • DRASTIC: significant decrease in the number and defined daily dose of antihypertensive agents at 3 months. This difference was no longer significant at 12 months after cross over of medically treated patients to PTA • Nordman. Cochrane Library of Systematic Reviews. 2004: ; vol 2
Meta-analysis PTRA vs Medical treatment Ives et al. Nephrol Dial Transplant 2003 Nordmann et al. Am J Med 2003 Change in blood pressure
Renal function No significant difference in serum creatinine or creatinine clearance between the two groups in any of the trials. • Nordman. Cochrane Library of Systematic Reviews. 2004: ; vol 2
Meta-analysis PTRA vs Medicatie Ives et al. Nephrol Dial Transplant 2003 Nordmann et al. Am J Med 2003 Change in renal function
Cardiovascular and Renovascular Complications In all studies, the risk of cardiovascular and renovascular complications were lower in the PTA vs. Medical treatment group (9. 6% vs 24. 5%) • Cardiovascular complications (myocardial infarction, angina, heart failure, stroke, non -procedure-related symptomatic hypotension, or cardiovascular death) • Renovascular complications (defined as an increase of serum creatinine of more than 50 per cent, cholesterol embolisation, development of renal failure, total occlusion of the stenotic artery, dissection of the renal artery, major complication during balloon angioplasty other than Haematoma at the puncture site, or need for dialysis)
Conclusions 1. In patients whose blood pressure could be controlled with medical therapy alone, no trial was able to demonstrate a statistically significant difference in blood pressure between balloon angioplasty and medical therapy. 2. In patients with refractory hypertension to medical therapy, the results of the DRASTIC trial demonstrated that balloon angioplasty was better than medical therapy in respect of more efficient blood pressure control.
PTA vs Stent • • • 85 patients with ostial RAS. Intention-to-treat analysis. Inclusion: – – – • RAS>50% HTN Positive captopril renography OR increase Cr after ACE-I Exclusion: – Renal size < 8 cm – <25% renal function by renography van de Ven et al. Lancet 1999
PTRA versus Stent van de Ven et al. Lancet 1999 Cumulative primary patency (%) Cumulative primary patency 100 Stent 80 60 p < 0. 001 40 20 Angioplasty 0 0 1 2 3 4 5 6 Time after procedure (months) Stent 42 37 37 36 36 35 35 30 PTRA 42 24 23 21 21 12
PTRA versus Stent van de Ven et al. Lancet 1999 Blood pressure Renal function
“The majority of patients with significant RAS and hypertension or renal function loss can be treated medically without the risk of mortality or progression to endstage disease”. Exceptions: Bilateral RAS; RAS in solitary kidney. 2 X mortality risk; 1. 5 X risk of renal failure. Care if renal mass loss OR loss of renal function when ACE inhibitor is used!
Angioplasty and Stent for Renal Arterial Lesions • Multicenter Randomized clinical trial. • Approx 1000 pts will be randomized to optimal medical therapy or to stenting with optimal medical therapy
Revascularization versus Medical Therapy for Renal-Artery Stenosis The ASTRAL Investigators Background Percutaneous revascularization of the renal arteries improves patency in atherosclerotic renovascular disease, yet evidence of a clinical benefit is limited. Methods In a randomized, unblinded trial, we assigned 806 patients with atherosclerotic renovascular disease either to undergo revascularization in addition to receiving medical therapy or to receive medical therapy alone. The primary outcome was renal function, as measured by the reciprocal of the serum creatinine level (a measure that has a linear relationship with creatinine clearance). Secondary outcomes were blood pressure, the time to renal and major cardiovascular events, and mortality. The median follow-up was 34 months. Results During a 5 -year period, the rate of progression of renal impairment (as shown by the slope of the reciprocal of the serum creatinine level) was – 0. 07 x 10– 3 liters per micromole per year in the revascularization group, as compared with – 0. 13 x 10– 3 liters per micromole per year in the medical-therapy group, a difference favoring revascularization of 0. 06 x 10– 3 liters per micromole per year (95% confidence interval [CI], – 0. 002 to 0. 13; P=0. 06). Over the same time, the mean serum creatinine level was 1. 6 µmol per liter (95% CI, – 8. 4 to 5. 2 [0. 02 mg per deciliter; 95% CI, – 0. 10 to 0. 06]) lower in the revascularization group than in the medicaltherapy group. There was no significant between-group difference in systolic blood pressure; the decrease in diastolic blood pressure was smaller in the revascularization group than in the medical-therapy group. The two study groups had similar rates of renal events (hazard ratio in the revascularization group, 0. 97; 95% CI, 0. 67 to 1. 40; P=0. 88), major cardiovascular events (hazard ratio, 0. 94; 95% CI, 0. 75 to 1. 19; P=0. 61), and death (hazard ratio, 0. 90; 95% CI, 0. 69 to 1. 18; P=0. 46). Serious complications associated with revascularization occurred in 23 patients, including 2 deaths and 3 amputations of toes or limbs. Conclusions We found substantial risks but no evidence of a worthwhile clinical benefit from revascularization in patients with atherosclerotic renovascular disease. Volume 361: 1953 -1962 November 2009
Renal Function in Patients with Renal-Artery Stenosis Treated with Revascularization or Medical Therapy Alone The ASTRAL Investigators. N Engl J Med 2009; 361: 1953 -1962
Kaplan-Meier Curves for the Time to the First Renal and Cardiovascular Events The ASTRAL Investigators. N Engl J Med 2009; 361: 1953 -1962
Kaplan-Meier Curves for Overall Survival The ASTRAL Investigators. N Engl J Med 2009; 361: 1953 -1962
Systolic and Diastolic Blood Pressure The ASTRAL Investigators. N Engl J Med 2009; 361: 1953 -1962
Last question: why does renal function may deteriorate after revascularization? 1. Contrast nephropathy. 2. Cholesterol embolization. 3. Exposure of diseased glomeruli to high blood pressure.
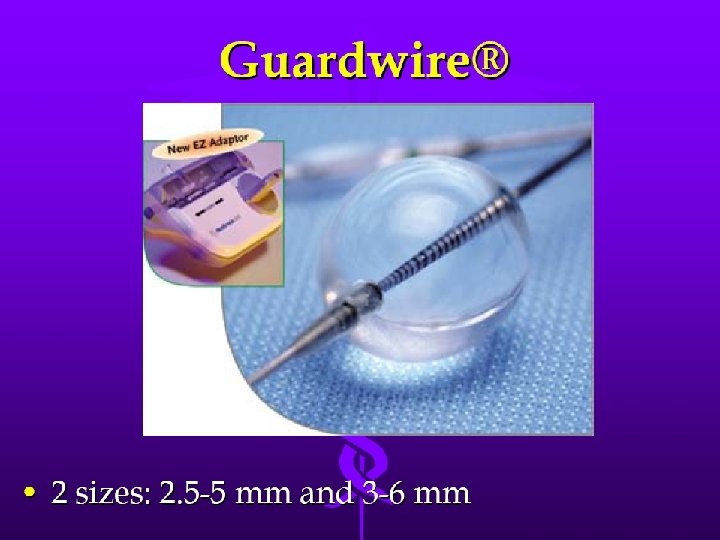
Is there any role for distal protection? • 65 hypertensive patients with significant RAS were stented with distal protection. • 2 protection devices were used: – Guardwire: 2 sizes [2. 5 -5 mm and 3 -6 mm] – Filterwire: 3. 5 -5. 5 mm] • Henry et al. Cath and cardio interv 2003
Results • ASA and plavix for 4 weeks. • Follow up: average 22 months; DSA if restenosis suspected by US. • Cr improved or stabilized in ALL patients. • The patients with moderate to severe renal impairment benefited the most. • Blood pressure control in all.
Distal protection devices • Visible debris in filter in all cases. • Atheromatous plaques, necrotic cores, thrombi, macrophages.
Indications for revascularization of RAS 1. Hypertensive control. 1. Reasonable likelihood of cure. 1. 2. 3. Onset before age 30. Recent onset after age 60. FMD. 2. Hypertension is “refractory” to medical treatment with at least 3 different class drugs including 1 diuretic. 3. “Accelerated” hypertension. 4. “Malignant” hypertension [end-organ damage: LV hypertrophy, CHF, visual or neurological disturbance, grade III-IV retinopathy]. 5. Non compliant patient.
Indications 2. Renal salvage 1. Unexplained worsening of renal function. 2. Loss of renal mass during anti-hypertensive therapy. 3. Impairment of renal function secondary to hypertensive treatment particularly to ACE inhibitor. 4. Progression of RAS under surveillance. 3. Cardiac Disturbance syndrome 1. Flash pulmonary edema. 2. Unstable angina. 3. Worsening of CHF.
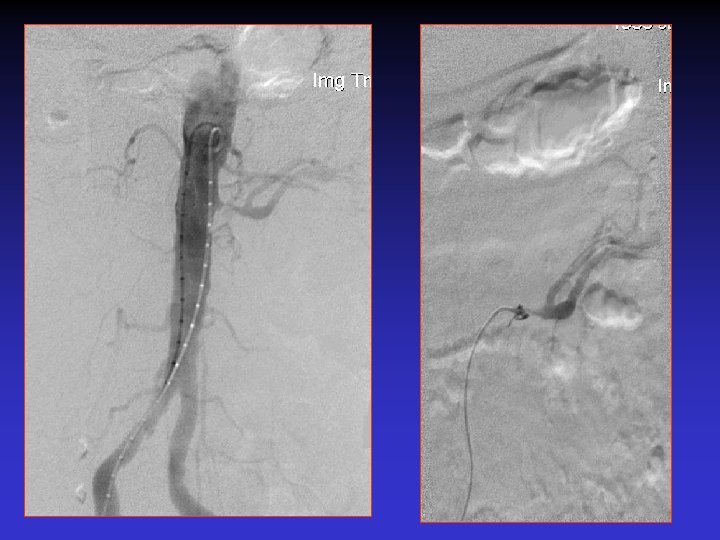
Case #1 S/p EVAR new onset of HTN
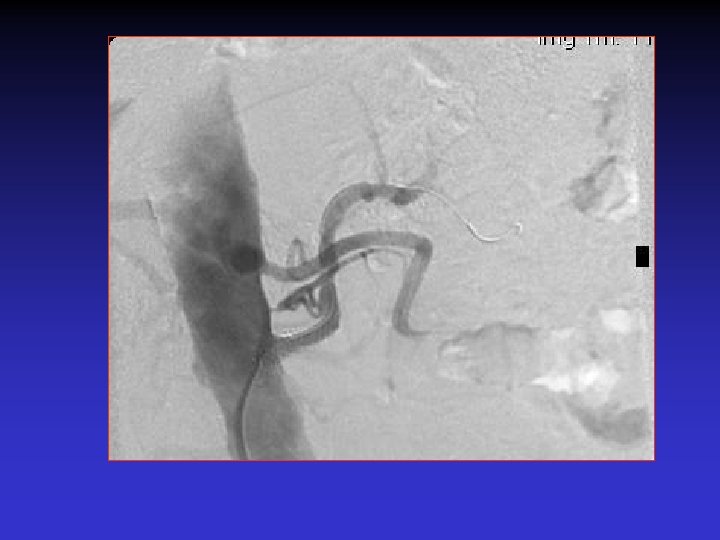
Case # 2 • 50 -year-old male with solitary kidney. • Smoker. • Refractory HTN. • Cr: 3. 8 mg/dl
• B/P: 160/80 mm. Hg • Cr: 1. 8 mg/dl
The patient was re-admitted 18 months later with Cr: 2. 8 mg/dl, and BP: 180/90 mm. Hg.
Conclusions • Incidental RAS is not an indication for revascularization. • Hypertensive patients with RAS may benefit from revascularization if HTN is “refractory” to medical treatment. • Revascularization is indicated in hypertensive patients with RAS if renal mass loss or renal function decline is observed during hypertensive treatment.