CELIAC DISEASE What is this and what is





 � � � One of the 8 most common Ig. E")
 SENSITIVITY (NCG(W)S) � � � Most difficult to diagnosis as there")





 converts glutamine on Peptides with")












 AND CELIAC DISEASE (CD)")







")








 Larsson")



















- Slides: 63
CELIAC DISEASE: What is this and what is the relation to Diabetes Troy E. Gibbons, M. D. 2 nd Annual Barnstable Brown Diabetes Center Symposium Lexington, Ky. September 2018
CONFLICT OF INTEREST NOTHING TO DECLARE
Upon completion of this activity, participants will be able to: � Select appropriate diagnostic testing for the evaluation of Celiac Disease in patients with diabetes.
WHEAT INDUCED IMMUNE RELATED DISORDERS � � IN THE U. S APPROX 1: 105 IN POPULATION WITHOUT RISK FACTORS MAY HAVE GLUTEN-RELATED DISORDERS* 50% OF CALORIES IN INDUSTRAILIZED AND DEVELOPING COUNTRIES COME FROM WHEAT 2013 PER CAPITA WHEAT FLOUR CONSUMPTION 132. 5 lb. IN THE U. S** LOSS OF WHEAT/GLUTEN TOLERANCE MAY OCCUR AT ANY POINT DUE TO UNKNOWN ENVIRONMENTAL TRIGGERS*** *Lohi S et al Aliment Pharmacol Ther. 2007; 26(9): 1217– 1225. **www. ers. usda. gov/topics/crops/wheats-role-in-the-us-diet. aspx# ***Catassi C, Kryszak D, et al. Natural history of celiac disease autoimmunity in a USA cohort followed since 1974. Ann Med. 2010; 42(7): 530– 538.
IMMUNOLOGICAL DISEASES RELATED TO WHEAT INGESTION � CELIAC DISEASE � WHEAT ALLERGY � NON CELIAC GLUTEN SENSITIVITY
WHEAT ALLERGY (WA) � � � One of the 8 most common Ig. E mediated food allergies 0. 3%-. 5% among children* Results in an immediate or delayed type reaction Skin, gut, respiratory typical targets Food dependent exercise induced anaphylaxis, baker’s asthma *Venter C et al. Prevalence of sensitization reported and objectively assessed food hypersensitivity amongst six-year-old children: a population-basedstudy. Pediatr Allergy Immunol 2006: 17: 356– 63.
NON CELIAC GLUTEN(WHEAT) SENSITIVITY (NCG(W)S) � � � Most difficult to diagnosis as there are no diagnostic test, defined by clinical symptoms when CD and WA are ruled out by negative testing Prevalence between 3%-6%? No confirmatory tests implies there is a lot of self-diagnosing Immune mediated innate immune response Intestinal permeability is intact unlike CD Volta U. et al New understanding of gluten sensitivity. Nat Rev Gastroenterol Hepatol 2012; 9: 295– 299. Sapone A. et al Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med 2012; 10: 13.
CELIAC DISEASE
DEFINITION An immune mediated disorder of the small intestine that is triggered by gluten exposure in genetically susceptible host. The pathogenesis usually involves increased small intestinal permeability.
PREVALANCE OF CD Changed in the last half century � Varies world wide but averages 1% in the U. S. prevalence is about 1 in 133 (. 75%) � Average of diagnosis 45 yrs. � Average time to diagnosis 10 to 12 yrs. � N. I. H estimates 3 million with CD in U. S. most are undiagnosed �
WHAT IS GLUTEN �Complex group of proteins in wheat endosperm (gliadins and glutenins. �Related proteins in rye (Secalin) and barley (Hordeins) will trigger inflammation in people with CD.
WHAT IS GLUTEN � These proteins have repetitive sequences rich in the amino acids proline and glutamine which resist digestion. � Undigested peptides Translocate intestine barrier.
WHAT IS GLUTEN � Tissues transaminase 2 (TG 2) converts glutamine on Peptides with the sequence Gln X X Pro to glutamate. � This sequence has high affinity binding to the cell surface proteins of HLA-DQ 2 or DQ 8 � This leads to a gluten specific T-cell response
LUMEN GLUTEN RELATED PEPTIDES CELL TG 2 HLA-DQ 2/8 DE AMIDATED GLUTEN HLA/DEAMINATEDGLUTEN COMPLEX CD 4+ T-CELL RESPONSE CYTOKINE INDUCED INFLAMMATORY CASCADE VILLOUS ATROPHY INFILTRATION OF INFLAMMATORY CELLS CRYPT HYPERPLASIA
PRESENTAION OF CD
PRESENTAION OF CD
COMPLICATIONS OF CD � � � Malnutrition Growth failure Extra intestinal disease Osteoporosis Infertility Gastrointestinal malignancy
DIAGNOSTIC TOOLS FOR CD � CD SPECIFIC ANTIBODY TESTING: � Ig. A ANTIBODIES AGAINST TISSUE TRANGLUTAMINASE (TG 2) � Ig. A ANTIBODIES AGAINST ENDOMYSIUM * (AMA) � ANTIBODIES AGAINST DEAMIDATED GLIDEN PEPTIDE (DGP) � HLA TESTING FOR HLA-DQ 2 AND HLA-DQ 8 � ENDOSCOPY/HISTOLOGY Husby S. J. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. . 2012 Jan; 54(1): 136 -60 Endomycium is the reticulin-like connective tissue around the smooth muscle fibers of monkey esophagus
DIAGNOSTIC TOOLS FOR CD SEROLOGY TESTING FOR CD: � Ig. A levels should be done. � Patient should have recent exposure to gluten. � Presence/absence of immunosupressors. � Ig. G results used only when Ig. A is low. Husby S. J. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. . 2012 Jan; 54(1): 136 -60 Endomycium is the reticulin-like connective tissue around the smooth muscle fibers of monkey esophagus
DIAGNOSTIC TOOLS FOR CD HLA TESTING FOR HLA-DQ 2 AND HLA-DQ 8: � 90 - 95% of population with CD has this HLA allele � 10 – 5% DO NOT! � � HLA-DQ 2 AND HLA-DQ 8 are very common in North America and Europe Only about 3 -4% of population with HAL-DQ 2 AND HLA-DQ 8 will develop CD. Husby S. J. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. . 2012 Jan; 54(1): 136 -60
PRESENTATION GROSS APPEARANCE DOUDENAL MUCOSA WITH CD NORMAL DOUDENAL MUCOSA
PESENTATION HISTOLOGY MUCOSA IN CD NORMAL DOUDENUM
WHO SHOULD BE TESTED FOR CD GROUP 1: CHILDREN WITH UNEXPLANINED SYMPTOMS/SIGNS � � � Episodic diarrhea FTT Wt. loss Growth stunting Delayed puberty Iron deficient anemia Chronic abd. pain Cramping or distension Atypical rashes Fractures with minimal trauma Abnormal LFT GROUP 2: ASYMPTOMINC CHILD WITH INCREASED RISK OF CD � � � Type 1 IDDM Trisomy 21 Turners syn. Autoimmune thyroid disease First degree relative with CD Husby S. J. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. . 2012 Jan; 54(1): 136 -60
THERAPY � � Gluten free diet �Improves GI symptoms in weeks �Histological response �Serological response Problem �Requires life long adherence
ADHERANCE: PROBLEMS � Gluten is everywhere � Some may be sensitive to very small amounts � � Gluten free products may be contaminated unknowingly It may be expensive
TYPE 1 DIABETES (T 1 D) AND CELIAC DISEASE (CD)
RELATION BETWEEN CD AND T 1 D � NATURE OF ASSOCIATION BETWEEN CD AND TID? � PREVALENCE OF CD IN PATIENTS WITH T 1 D? � PREVALENCE OF T 1 D IN PATIENTS WITH CD? � HOW TO MONITOR CD IN T 1 D? � DOES MANAGING CD IMPROVE T 1 D OUTCOME?
WHY THE RELATION BETWEEN T 1 D AND CD?
GENETIC RELATIONSHIP � � Overlap of susceptibility genes in the HLA class 11 region [ HLA-DRB 1, HLA-DQA 1, HLA-DQB 1] contribute to the coexistence of T 1 D and CD. HLA-DQ 2 [alleles DQA 1805 and DQB 1*02] and HLA-DQ 8 [alleles DQA 1*03: 01 -DQB 1*03: 02 and HLA-DR 4 -DQ 8] have the strongest genetic risk factors for T 1 D and CD (MHC class 11 genes**) ** Class 1 genes variations on MHC also associated T 1 D and CD
MECHANISM � � The trans-membrane glycoproteins may bind peptides from insulin secreting cells or gluten – derived protein. Presentation to the CD 4+ T lymphocytes may be atypical and result in a subsequent inflammatory cascade in the islet cells and intestinal epithelial cells.
WHAT IS THE ROLE OF ENVIROMENTAL FACTORS?
ARE THERE KNOWN TRIGGERS IN THE ENVIRONMENT? � � Prevalence of T 1 D and CD has risen significantly in the last half century. Suggest that genetic risk factors are not the primary cause for the increased prevalence
ARE THERE KNOWN TRIGGERS IN THE ENVIRONMENT? � � Understanding/identifying risk factors has the potential to reduce the prevalence of T 1 D/CD. Large number of studies are ongoing to address relation between environmental factors, CD and T 1 D
Adapted from Verdu EF, Danska JS. Nature Immunologyvolume 19, pages 685– 695 (2018)
ENVIRONMENT : Diet � � Feeding practices or gluten introduction have no influence on T 1 D risk (BABYDIET 2015). Delayed gluten introduction (12 months or greater) has no effect on the risk of islet autoantibodies [AABs] (BABYDIET). Infection at the time of gluten introduction is not a major risk factor. Delayed introduction of bovine milk did not effect prevalence of TID or increase risk of development of islet cell antibodies or antibodies to TG 2. (TRIGR).
ENVIRONMENT : Intestinal microbiome/products � � C/S delivery did not increase risk of infants developing IABs born to diabetic parents but when T 1 D does develop it progresses more rapidly (BABYDIAB). There may an association between TID and low gut microbial diversity
ENVIRONMENT : Infection � � Studies suggests that viral exposure can induce islet autoimmunity. Enteroviral infections may be a risk factor based on epidemiological evidence and observation of enterovirus proteins and RNA in the islet of people with T 1 D* Op de Beeck et al. Nat. Rev. Endocrinol. 12, 263 -273 (2016)
IS CD PHENOTYPICALLY THE SAME AS CD/T 1 D? � � CD in T 1 D/CD may be phenotypically less severe than CD alone (Touska a et. al. ) T 1 D/CD may have increase prevalence of other autoimmune diseases (especially Thyroid) compared to CD alone. Tsouka A et. al. JPGN 2015; 61: 297 -302
RELATION BETWEEN CD AND T 1 D � NATURE OF ASSOCIATION BETWEEN CD AND TID? � PREVALENCE OF CD IN PATIENTS WITH T 1 D? � PREVALENCE OF T 1 D IN PATIENTS WITH CD? � HOW TO MONITOR CD IN T 1 D? � DOES MANAGING CD IMPROVE T 1 D OUTCOME?
PREVALENCE BETWEEN TID AND CD IN THE GENERAL POPULATION � > 26, ooo patients with type T 1 D � Bx. confirmed CD 6% world wide (4. 8% North America) � Heterogeneity was large (1. 6% to 12. 3%) � Prevalence lower in adults with T 1 D and higher in children with T 1 D � The underlying prevalence in the general population had no relationship to the prevalence of CD in individuals with T 1 D in that country. Elfstrom et al. aliment Pharmacol Ther 2014; 40: 1123 -1132
PREVALENCE BETWEEN TID AND CD IN THE GENERAL POPULATION Conclusion: 1 in 20 patients with T 1 D have biopsy proven CD.
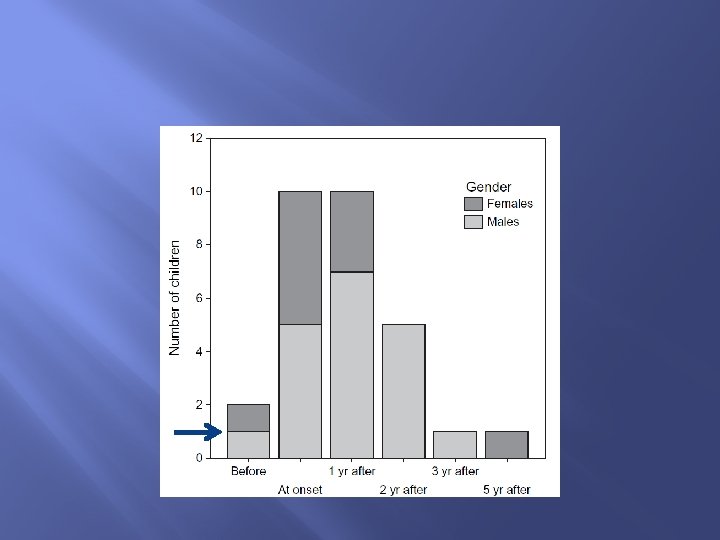
PREVALENCE BETWEEN TID AND CD: SCREENING IN CHILDREN � � � Pediatric study, 300 participants followed for 5 years. Low prevalence of symptomatic CD at diagnosis (0. 7%) Increasing prevalence of silent CD during 5 year follow up to a prevalence of 10% Larsson et al. Ped Diabetes 2008 : 9 (part 11): 354 -359
PREVALENCE BETWEEN TID AND CD: SCREENING Time between TID and CD (yrs. ) Larsson et al. Ped Diabetes 2008 9 (part 11): 354 -359
PREVALENCE BETWEEN TID AND CD: SCREENING CONCLUSION: PEDIATRIC PATIENT WITH T 1 D SHOULD BE SCREENED FOR CD: • At the onset of diagnosis. • Annually for the first 2 years. • Patients with clinical symptoms should be screen regardless.
RELATION BETWEEN CD AND T 1 D � NATURE OF ASSOCIATION BETWEEN CD AND TID? � PREVALENCE OF CD IN PATIENTS WITH T 1 D? � PREVALENCE OF T 1 D IN PATIENTS WITH CD? � HOW TO MONITOR CD IN T 1 D? � DOES MANAGING CD IMPROVE T 1 D OUTCOME?
� � Longitudinal retrospective study from 1989 to 2011 1215 CD cases and 6075 matched references Looked at TID and thyroid disease Noted: � Increased risk of subsequent TID but this was not statistically significant (HR 2. 5 [95% CI 0. 94 -6. 66]) Canova et al. J Pediatr 2016; 174: 146 -52.
CONCLULSION Be aware of an association of patients with CD who may develop T 1 D but screening is not necessary
RELATION BETWEEN CD AND T 1 D � NATURE OF ASSOCIATION BETWEEN CD AND TID? � PREVALENCE BETWEEN T 1 D AND CD? � PREVALENCE BETWEEN CD AND T 1 D? � HOW TO MONITOR CD IN T 1 D? � DOES MANAGING CD IMPROVE T 1 D OUTCOME?
MONITORING RESPONSE TO GLUTEN FREE DIET � SEROLOGY � DIET EVALUATION � ENDOSCOPY WITH BIOPSY
MONITORING RESPONSE: SEROLOGY TESTING AND TREATMENT RESPONSE; IS IT GOOD? � In adult studies we know: � Poor correlation between serology normalization and dietary transgressions � Anti-endomysial markers are poor markers of ongoing mucosal injury � Serum Ig. A TTG class antibodies also poorly correlated with mucosal healing in adults � The recommendation in adults is assessing mucosal recovery is best done by histological evaluation. * *Haines et al. Aliment. Pharmacol. Ther. 2008; 28: 1042 -66
MONITORING RESPONSE: SEROLOGY TESTING AND TREATMENT RESPONSE IN THE CHILD; IS IT GOOD? � � � CD in children however may be phenotypically different. On a gluten free diet most children have mucosal healing in 1 year compared to adults (2 years). Children with autoimmune disease (T 1 D) more likely to have elevated TTG Ig. A in the presence of normal mucosa. * * Sardy et al. Clin Chim Acta 2007 ; 376 : 126 – 35
MONITORING RESPONSE: SEROLOGY TESTING AND TREATMENT RESPONSE; IS IT GOOD? � Bannister et al (Australia). � Prospective longitudinal study on 150 children (all inclusive). � Compared endoscopic mucosal healing at 12 months with TTG Ig. A and anti-deamidated gliadin peptide [Ig. G] (DGP) serology. Bannister et al. Am J Gastroenterol 2014; 109: 1478– 1483; .
SEROLOGY TESTING AND TREATMENT RESPONSE; IS IT GOOD CONCLUSION: • Many positive antibody test in the presence of healed intestinal mucosa suggest weak positive predictive value. • Especially so with TTG Ig. A. • Combined negative serology of TTG Ig. A and DGP very high negative predictive value (98%).
MONITORING RESPONSE: VALIDATED DIETARY QUESTIONNAIRE � � Dietary evaluation by a highly skilled nutritionist remains the standard to monitor for a gluten free diet. Offering alternatives to gluten containing food that are : Palatable Micronutrient appropriate.
MONITORING RESPONSE: VALIDATED DIETARY QUESTIONNAIRE � � Intentional and unintentional gluten exposure is problematic particular in the patient without symptoms of CD. Dietary evaluation will involve: �Review of a 3 day diet diary �Food ingredient review �Clinical review
RELATION BETWEEN CD AND T 1 D � NATURE OF ASSOCIATION BETWEEN CD AND TID? � PREVALENCE OF CD IN PATIENTS WITH T 1 D? � PREVALENCE OF T 1 D IN PATIENTS WITH CD? � HOW TO MONITOR CD IN T 1 D? � DOES MANAGING CD IMPROVE T 1 D OUTCOME?
HOW IMPORTANT IS MANAGING CD IN PATIENTS WITH T 1 D � � � Both diseases have long-term serious sequel on their own. Quality of Life (QAL) issues are important. QAL of life studies in adults and pediatrics show reduced QAL if on a GFD and patient was asymptomatic for CD QAL improves if patient was symptomatic for CD.
HOW IMPORTANT IS MANAGING CD IN PATIENTS WITH T 1 D � Metabolic control � Bone mineralization � Microvascular complications
HOW IMPORTANT IS MANAGING CD IN PATIENTS WITH T 1 D � � Metabolic control: �Adults; no difference in Hb. A 1 c on GFD �Pediatrics; equivocal with no change, decrease and even increase* in Hb. A 1 C on GFD Impaired bone mineralization: �Pediatric and adults may have reduced bone mineral density (BMD) with CD and T 1 D compared to T 1 D alone** *Sun et al Diabet Med 2009; 26 1250 -4 **Lunt H et al, Diabetes Care 2001; 24: 791 -2 ** Diniz-Santos DR et al. Dig Dis Sci 2008; 53: 1240– 5
HOW IMPORTANT IS MANAGING CD IN PATIENTS WITH T 1 D � Microvascular complications: �Adult; Increased prevalence of renal disease and retinopathy in adults with CD and T 1 D compared to T 1 D* �Pediatrics; lower protective high density lipoprotein (HDL) in children with CD and T 1 D compared to T 1 D** *Leeds et al. Diabetic Care. 2011: 34, (2158 -2163) ** Warncke K et al Pediatric Diabetes 2016: 17: 191 -198
RELATION BETWEEN CD AND T 1 D � NATURE OF ASSOCIATION BETWEEN CD AND TID? � PREVALENCE OF CD IN PATIENTS WITH T 1 D? � PREVALENCE OF T 1 D IN PATIENTS WITH CD? � HOW TO MONITOR CD IN T 1 D? � DOES MANAGING CD IMPROVE T 1 D OUTCOME?
END