CELIAC DISEASE 01 ABOUT THE DISEASE Celiac Disease

CELIAC DISEASE

01 ABOUT THE DISEASE
 Celiac disease (CD) is one of the")
Celiac Disease ( Gluten. Sensitive Enteropathy ) Celiac disease (CD) is one of the most common genetically related food intolerance disorder, worldwide. The disease primarily affects the small intestine (mainly the proximal small intestine), where it progressively leads to flattening of the small intestinal mucosa.

GENETIC FACTORS INTESTINAL MUCOSA ENVIRONMENTAL FACTORS It is a multifactorial, autoimmune disorder that occurs in genetically susceptible individuals. It is triggered by a well-identified environmental factor (gluten and related prolamins present in wheat, rye, and barley).

The most common period of presentation is between 6 mo and 2 yr of age, but it can occur at any stage in life; a diagnosis is not unusual in people older than 60 years. The disorder does not present until gluten products have been introduced into the diet, and it is a permanent intolerance to gluten. It mostly affects people of northern Europe and their descendants in other parts of the world(eg, England, Ireland, Italy and united states), but it has not been described among the Japanese , who lack the genetic predisposition and environmental exposure to wheat.
 is a common disorder that is estimated to affect about")
PREVALENCE Celiac disease (CD) is a common disorder that is estimated to affect about one percent of the population.

KEY NUMBERS 95% of affected individuals are HLA-DQ 2 and less commonly HLA-DQ 8 positive Prevalence is greater in women. 10 -20%. The risk in 1 st-degree relatives

PATHOLOGY GLUTEN is a group of proteins found in some cereal grains, mainly wheat. Gluten is composed of multiple proteins. Glutenin, the first protein in the gluten-matrix, is digested by enzymes easily, because it is a long protein with a great amount of surface area for the enzymes to attach and degrade However, Gliadin, the other protein, is a densely packed protein with a low surface area to volume ratio, making it difficult for enzymes to encounter. In addition, gliadin protein has a large amount of amino acids that are especially difficult to digest. These difficult to digest amino acids are proline and glutamine.

PATHOLOGY Normally gluten from diet enter small intestine into lamina propria, and get digested in dendritic cells, or it get deamidated by tissue transglutaminase II, then it will be digested in the small intestine. But in celiac disease when gluten get into lamina propria it will(imp) : activate the innate immune system and IL-15 is released. gluten is deamidated or transamidated by Tissue transglutaminase II(imp) which modifies gluten into a form that may stimulate the immune system more effectively. dendritic cells will recognize gluten as a foreign body and presents it is antigen through Major Histocompatibility Complex MHC II , ( mostly HLA-DQ 2 and HLA-DQ 8), this process will present gluten antigen to helper T-cells. T-Helper Cells will produce more cytokines and activate B-Cells, and then plasma cells will produce antibodies to gluten, and those antibodies will bind to tissues or be released to blood stream, and systemic inflammatory response is established against gluten
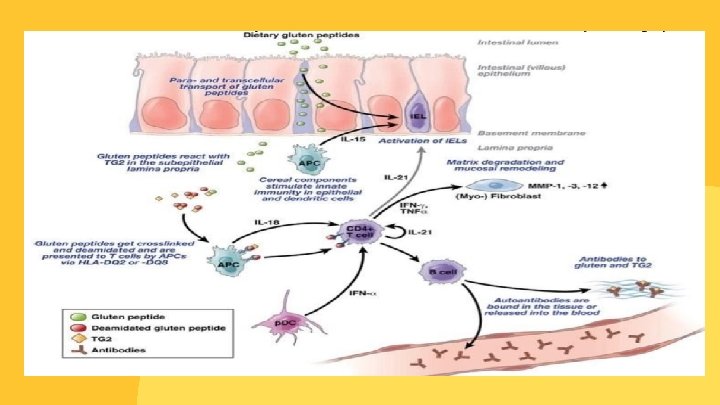

This immune response will lead to villous atrophy , crypt hyperplasia and damage to the surface epithelium in the small bowel(imp)

So the function of small bowel mucosal lining will be disrupted and malabsorption to nutrients, minerals and fat soluble vitamins (K, E, D, A) occur. • The injury is greatest in the proximal small bowel and extends distally for a variable distance , this explain why patients with celiac disease have variable degree of symptoms.

RISK FACTORS 2 -3% 30% Hyposplenism AUTOIMMUNE THYROIDITIS 5% 10% DOWN SYNDROME Ig. A deficiency MICROSCOPIC COLITIS TYPE 1 DIABETES

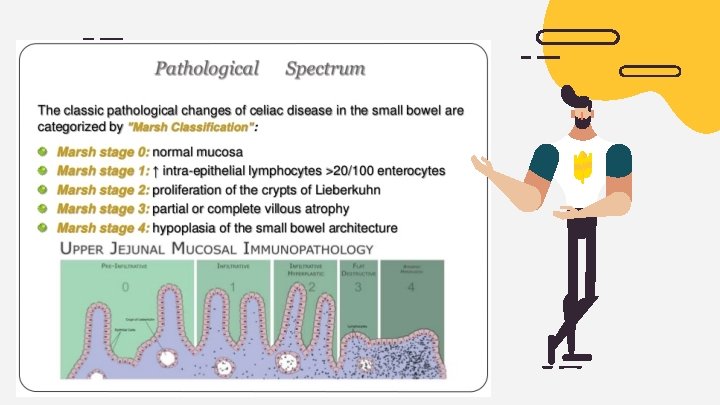
Clinical presentation : 5 possible presentations of celiac disease are recognized, as follows : Typical Atypical Potential latent Silent

• Typical: This presentation is primarily characterized by GI signs and symptoms. • Atypical: GI signs and symptoms are minimal or absent, and various extraintestinal manifestations are present. • Silent: The small intestinal mucosa is damaged, and celiac disease autoimmunity can be detected with serology; however, no symptoms are present. • Potential: Patients have a positive specific autoimmune serology and may or may not be symptomatic, but the mucosa morphology is normal. These individuals have genetic compatibility with celiac disease and fullblown celiac disease may develop at a later stage in some or all of these individuals. careful follow-up without diet therapy is the most appropriate current recommendation. • Latent: Individuals with normal mucosal morphology who “have had a gluten-dependent enteropathy at some point in their life. ” This subset of patients is the rarest of the group.


Typical presentation CHRONIC DIARRHEA bulky, pale, frothy, greasy, foulsmelling stools Anemia and vitamin deficiencies Fat-soluble vitamin deficiency is common. Rickets can be seen in growing children. Hypo-prothrombinemia secondary to vitamin K malabsorption cause easy bleeding Anorexia about 10% of cases explosive watery diarrhea, marked abdominal distension, dehydration, hypotension, and lethargy, often with profound electrolyte abnormalities, including severe hypokalemia Constipation, vomiting, and abdominal pain results from a combination of anorexia, dehydration, muscle weakness, and bulky stools. celiac crisis Failure to thrive Weight loss is most marked in the limbs and buttocks. The abdomen becomes distended

Atypical presentation :
 is “celiac disease of the skin”. It is a chronic skin")
Dermatitis herpetiformis (DH) is “celiac disease of the skin”. It is a chronic skin condition with a characteristic rash with intense itching and burning sensations. About 10 -15% of patients with celiac disease have DH A new unscratched lesion is red, raised, and usually small, with a tiny blister in the center. However, if scratched, crusting appears on the surface. The burning or stinging sensation can be very intense. The most common areas are the elbows, knees, back of the neck, scalp, upper back, and the buttocks. Facial and hair-line lesions are not uncommon. The inside of the mouth is rarely affected. The rash has a symmetric distribution 83% of people with celiac disease undiagnosed or misdiagnosed

DIAGNOSIS Serological blood tests are the first-line investigation required to make a diagnosis of celiac disease also used for screening: 1. Anti-Tissue Transglutaminase (t. TG) antibodies: was initially reported to have a sensitivity (99%) and specificity (>90%) for identifying celiac disease. 2. Antiendomysial antibodies (EMAs): with a sensitivity of 90% and specificity of 99% 3. The antigliadin antibodies (AGA) are in the form of Ig. G and Ig. A. But it is not sensitive nor specific enough for routine use.

DIAGNOSIS Genetic screening tests is not currently recommended , because the most common alleles found in celiac disease (HLA-DQ 2 and HLADQ 8) are common in general population , so their presence do not mean that they have the disease. but Negative findings for HLA- DQ 2 and HLA-DQ 8 can essentially rule out current or future celiac disease in patients for whom other tests, including biopsy, do not provide a clear diagnostic result.

It's important to be tested for celiac disease before trying a gluten-free diet. Eliminating gluten from your diet might make the results of blood tests appear normal.

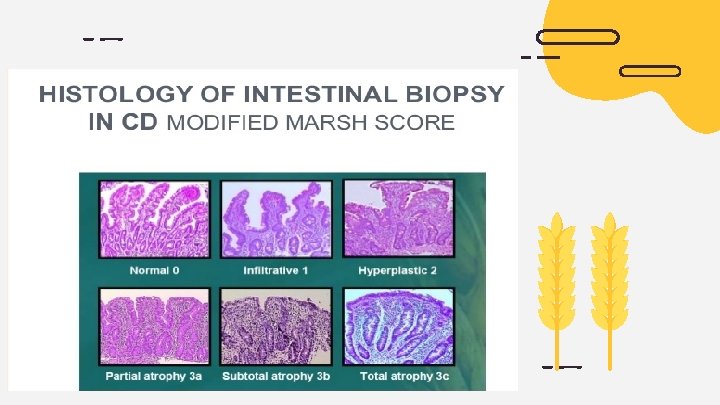
Endoscopy The gold standard for diagnosing celiac disease is biopsy. multiple biopsies are taken during esophagogastroduodenoscopy (EGD) , Obtaining at least 4 biopsy samples from the distal duodenum and 1 or 2 from the bulb ishighly recommended because mucosal changes in celiac disease may be patchy. This test uses a long tube with a tiny camera that's put into your mouth and passed down your throat (upper endoscopy). The camera enables your doctor to view your small intestine and take a small tissue sample (biopsy) to analyze for damage to the villi.

Other laboratory studies should be performed to rule out complications , including : 01 02 Cbc Calcium 04 05 Vit. D LIVER FUNCTION 03 Phosphate 06 IRON

TREATMENT A strict, lifelong gluten-free diet is the only way to manage celiac disease. Besides wheat, foods that contain gluten include: Barley Bulgur Durum Farina Graham flour Malt Rye Semolina Spelt (a form of wheat) Triticale

TREATMENT Many basic foods are allowed in a gluten-free diet, including: • • Eggs Fresh meats, fish and poultry that aren't breaded, batter-coated or marinated Fruits Lentils Most dairy products, unless they make your symptoms worse Nuts Potatoes Vegetables

Vitamin and mineral supplements If your anemia or nutritional deficiencies are severe, your doctor or dietitian might recommend that you take supplements, including: ü ü ü ü Copper Folate Iron Vitamin B-12 Vitamin D Vitamin K Zinc Vitamins and supplements are usually taken in pill form. If your digestive tract has trouble absorbing vitamins, your doctor might give them by injection.

Medications to control intestinal inflammation If your small intestine is severely damaged or you have refractory celiac disease, your doctor might recommend steroids to control inflammation. Steroids can ease severe signs and symptoms of celiac disease while the intestine heals. Other drugs, such as azathioprine (Azasan, Imuran) or budesonide (Entocort EC, Uceris), might be used

PROGNOSIS: The prognosis is excellent; the disorder is fully reversible if trigger foods are avoided.

THANKS! CREDITS: This presentation template was created by Slidesgo, including icons by Flaticon, and infographics & images by Freepik
- Slides: 32