Celiac Disease and lactose Intolerance in North Indian



















 Controls (n= 110) Boys 90 (58.")
 Controls (n= 110) Boys Mean ±")


 children with celiac disease recovered from lactose intolerance after")
 levels in lactose intolerant and tolerant celiac patients Lactose Intolerant")



 had lactose intolerance 2 children had only minor symptoms attributable to lactose")
")

 patients after 6 months 9")






- Slides: 42
Celiac Disease and lactose Intolerance in North Indian Children Prof Satyavati Rana Department of Super Specialty of Gastroenterology, Post Graduate Institute of Medical Education & Research, Chandigarh, 160012, India
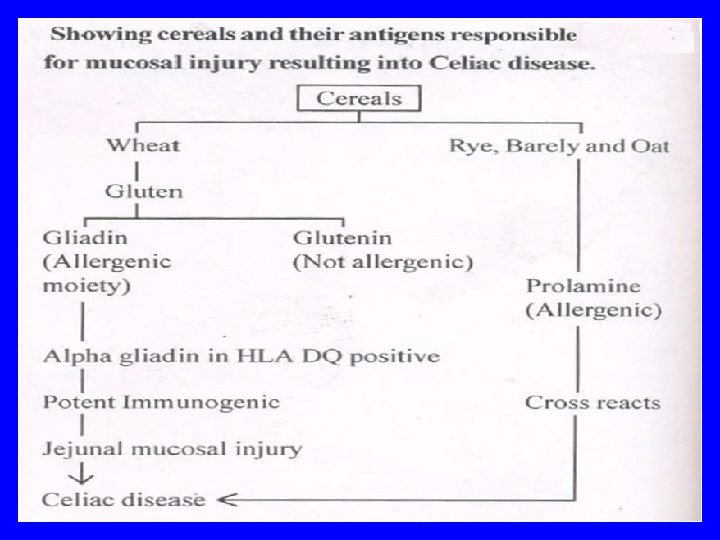
Introduction • Celiac disease is intestinal inflammatory disease that is triggered in genetically susceptible individuals by dietary gluten protein found in wheat, barley & rye • It is believed to be present in up to 1 in 100 of population
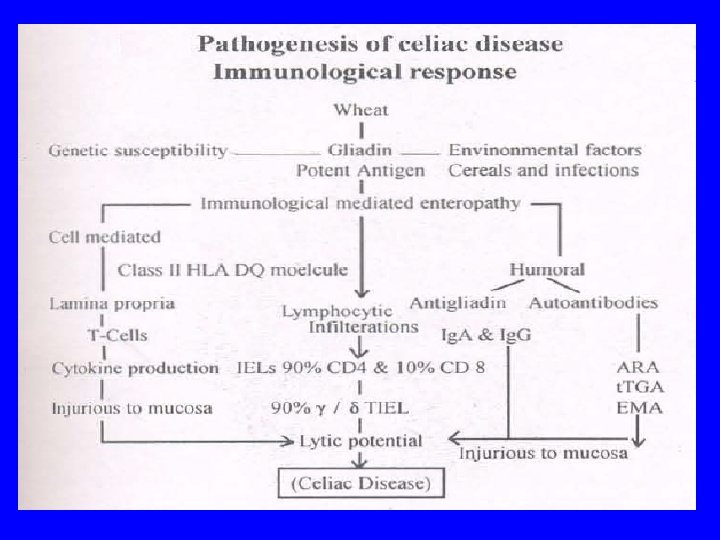
Factors involved in pathogenesis of celiac disease Saturni et al, 2010
Prevalence of celiac disease in Asia–Pacific region Cummins et al. , 2009
Tack et al, 2010
Yachha & Podder , 2007
Yachha & Podder , 2007
• Celiac disease often goes unrecognised & is consequently under-diagnosed • Only 10– 15% of people with condition are thought to be clinically diagnosed • It may be asymptomatic or symptomatic with severe malabsorption Ice Berg Model for Celiac Disease
Pathogenesis of Celiac Disease
• Main damage in Celiac disease occurs in small intestine which is characterized by -- intraepithelial lymphocytosis -- crypt hyperplasia -- villous atrophy
• In celiac disease, villi become shortened or even completely flattened This may result in decrease in brush border enzymes • Brush border enzymes include lactase which helps to digest lactose found in milk
H 2 gas produced is measured by LHBT
• Hence, newly diagnosed patients with celiac disease may discover that they are lactose intolerant • This type of lactose intolerance is called “secondary lactose intolerance” • It is temporary form that develops as result of celiac disease & may resolve as intestine heals
Aim of the study To elucidate lactose intolerance in children with celiac disease
Methodology 155 celiac disease children & 110 age & sex matched healthy controls with no GI symptoms were enrolled Informed consent was obtained Patients taking antibiotics within four weeks prior to test were excluded Children with serum t. TGA levels >10 U/ml were taken as +ve
Lactose Hydrogen breath test Patients were instructed to eat low fiber diet 3 days before test & come fasting for test 25 g lactose dissolved in 250 ml water was given orally after taking fasting breath H 2 concentration (Rana et al 1995)
H 2 concentration was measured in end expiratory breath of subjects at baseline & Rise ≥ 20 ppm over fasting value in 2 consecutive readings was considered as lactose intolerance after every 30 minutes up to 4 hrs by SC Microlyser from Quintron, USA
Gases released were detected by Breath analyzer
Interpretation of Lactose hydrogen breath test Lactose H 2 BT -ve for lactose malabsorption Lactose H 2 BT +ve for lactose malabsorption
Results Sex Distribution of Subjects Patients (n= 155) Controls (n= 110) Boys 90 (58. 06%) 65 (59. 09%) Girls 65 (41. 94%) 45 (40. 91 %) No significant difference was observed in sex distribution of patients
Age Distribution of Subjects Sex Patients (n= 155) Controls (n= 110) Boys Mean ± SD 6. 4 ± 3. 1 6. 7 ± 2. 9 (Range yrs) (5 -12) (4 -12) Mean ± SD Girls 7. 3 ± 2. 7 6. 9 ± 3. 2 (Range yrs) (5 -11) (5 -10) Mean ± SD of age among celiac disease boys and girls was comparable
Lactose intolerance in patients & controls *p < 0. 05 patients vs. controls (n = 155) (63. 6%) (36. 4%) (31. 6%) (68. 4%) * (n = 110)
*p = 0. 0059 males vs females * 46. 2% 24. 5% 53. 8% 75. 5% %age of lactose intolerance Lactose intolerance in male & female patients
• 10/69 (14. 4%) children with celiac disease recovered from lactose intolerance after GFD for 5 -6 months Lactose intolerance will be reassessed in these patients after 1 year
Tissue transglutaminase (tt. GA) levels in lactose intolerant and tolerant celiac patients Lactose Intolerant tt. GA (U/ml) 112. 86 ± 108. 02 Range 100 -298 Lactose Tolerant 129. 39± 100. 3 65 -300 No significant difference was observed in tt. GA levels of lactose intolerant and tolerant celiac patients
History of GI symptoms in lactose intolerant and tolerant celiac patients Lactose Intolerant Lactose Tolerant Diarrhea 47/106 (44. 3%) 23/49 (46. 9%) Constipation 44/106 (41. 5%) 21/49 (42. 8%) Flatulance/ Abdominal Pain 49/106 (46. 2%) 20/49 (40. 8%) No significant difference was observed in GI symptoms of lactose intolerant & tolerant celiac patients
VILLOUS ATROPHY LACTASE DEFICIENCY LACTOSE INTOLERANCE LACTOSE TOLERANT GLUTEN FREE DIET
Some Studies related to Celiac disease and Lactose intolerance
4/24 (17%) had lactose intolerance 2 children had only minor symptoms attributable to lactose 2 (8. 5%) required lactose-free diet before showing satisfactory weight gain Of these, one was an infant of 5 months who improved on lactosefree diet containing gluten She probably had 'secondary disaccharidase deficiency with symptoms', of presumed infective origin Mc. NEISH & Sweet , 1968 Glasgow
Study included 54 pts (15 males/39 females; mean age 37. 8 ± 7 yrs) from southern Italy 50 blood donors from similar population, matched for sex & age were enrolled as controls 24% of pts showed +ivity of celiac disease antibodies compared to 2% in controls (p < 0. 001) Histologic samples showed villous atrophy confirming celiac disease, while in controls duodenal biopsies were normal High prevalence of celiac disease was observed in pts with +ve LHBT compared to healthy controls Ojetti et al, 2005
Evaluate effect of gluten -free diet on lactose malabsorption using LHBT and relationship with normalization of duodenal biopsies in celiac patients • 15 pts (11 F, 4 M; mean age 35. 8± 6) affected by CD with +ve LBT and -ve glucose breath test were enrolled after 6 months by LBT All were started on GFD & were re-evaluated after 12 months by LBT and endoscopy with biopsies
LBT normalization was observed in 1 /15 (6. 7%) patients after 6 months 9 /14 (64. 2%) after 12 months Duodenal biopsies showed normal villi in 8 patients partial villous atrophy in 5 total atrophy in 2
Study shows that large proportion of CD patients experience regression of lactose malabsorption after GFD This may be related to normalization of brush border with an improvement of lactase enzyme activity
LBT should be performed after 12 months in CD patients on gluten-free diet in order to assess persistence/ disappearance of lactose malabsorption, thus avoiding an unnecessary lactose-free diet Ojetti et al, 2008
Conclusion This study indicates that lactose intolerance is common among children with celiac disease which can be one of the causes for gastrointestinal symptoms
Study going on. . Children with celiac disease were kept on gluten free diet Patients who were lactose intolerant are being followed up at 6 months of gluten free diet Lactose hydrogen breath test is being done to measure lactose intolerance Results yet to be analyzed
Thank you…
Celiac disease & LI - summary