ARDS Acute Respiratory Distress Syndrome Criteria ACUTE onset



 �Pancreatitis �Blood")


 Chest Radiograph: acute bilateral infiltrates 2) ABGs 3) Measurement of TNF, IL-8,")
 � 6 -12 hours after insult (range of up to 72")
 � Pulmonary edema")


 ventilation of oxygen to the lungs �")

 – Pa.")



 Ventilation �Alveoli filled with air are ventilated. Alveoli that are collapsed or filled")
- Slides: 22
ARDS
Acute Respiratory Distress Syndrome �Criteria: �ACUTE onset of bilateral infiltrates on chest x ray � Within a week of insult � Noncardiogenic pulmonary edema �Low ratio of Pa. O 2: Fi. O 2 � Partial pressure of arterial oxygen to fraction of inspired oxygen � Pa. O 2 = 80 -100 mm. Hg � Fi. O 2 = 0. 21
�Staging: �MILD � 200 mm. Hg > Pa. O 2/Fi. O 2 < 300 mm. Hg �MODERATE � 100 mm. Hg > Pa. O 2/Fi. O 2 < 200 mm. Hg �SEVERE � Pa. O 2 < 100 mm. Hg � Normal ratio is 300 -500 mm. Hg
�Risk Factors: Mortality rate of near 50% �Sepsis �Burns �Trauma �Pneumonia (aspiration) �Pancreatitis �Blood transfusion reaction
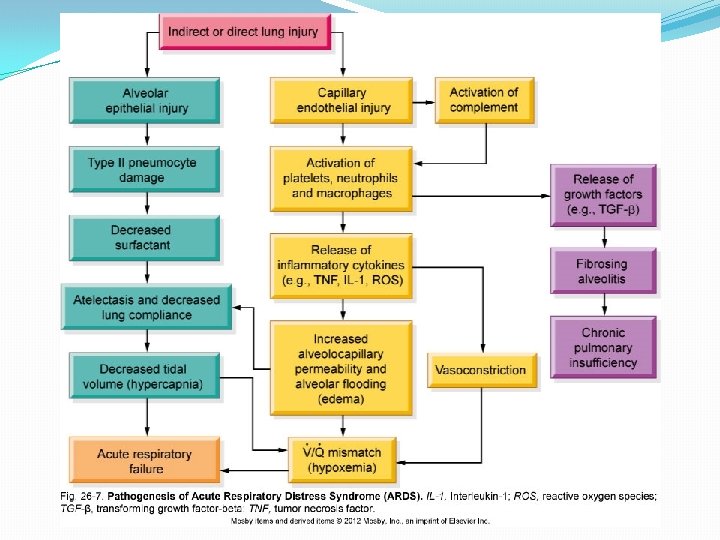
�ARDS �Inflammatory response injures alveolocapillary membrane disrupted gas exchange V/Q mismatch hypoxemia �Inflammatory response injures alveolocapillary membrane increased capillary permeability pulmonary edema
�Direct Cause �Inhalation of noxious substance direct inflammatory response ARDS �Aspiration of acidic stomach contents direct inflammatory response ARDS �Indirect Cause (most common) �Sepsis systemic inflammatory response ARDS �Severe Burn systemic inflammatory response ARDS �Severe Trauma systemic inflammatory response ARDS
Diagnostics 1) Chest Radiograph: acute bilateral infiltrates 2) ABGs 3) Measurement of TNF, IL-8, CBC 3) BNP: <100 pg/m. L (general guideline, not always accurate) -exclusion diagnostic 4) Echocardiogram -exclusion diagnostic 5) Lung Testing -exclusion diagnostic 6) Clinical Symptoms
�Phases: �Exudative (Inflammatory) � 6 -12 hours after insult (range of up to 72 hours) � Neutrophil activation � Release of inflammatory mediators (proteolytic enzymes, free radicals, platelet aggregates) � Pulmonary edema; Pulmonary hemorrhage � Decreased surfactant production � Alveolar collapse � Hypercapnia; Hypoxemia onset
�Proliferative � Commonly within 3 days. (range of 3 -21 days) � Pulmonary edema resolved � Exudate accumulates hyaline membrane � Rapid cellular proliferation � Hypoxemia worsens �Fibrotic � Can occur concurrently with proliferative phase or be delayed to 2 -3 weeks after initial insult � Commonly within 7 days. � Remodeling and Fibrosis occur � Decreased lung compliance � Extreme V/Q mismatch � Respiratory Failure MODS
�Clinical Manifestations: � Early signs � Dyspnea, inspiratory crackles, chest infiltrates on x ray seen within 24 -48 hours �Dyspnea ; hypoxemia onset; poor response to O 2 supplementation �Hyperventilation respiratory alkalosis �Decreased tissue perfusion; metabolic acidosis �Decreased tidal volume labored respirations hypoventilation �Respiratory acidosis; worsening hypoxemia �Hypotension, shock, respiratory failure, MODS, death
�Treatment: �Mechanical ventilation with PEEP �Supplemental supportive therapies � Vasopressors, fluid resuscitation if appropriate �Possible use of low dose corticosteroids during initial inflammatory phase. Not during later phases. �Treatment of underlying cause � Antibiotics to treat known infection or prophylactically
Gas Transport �Delivery of oxygen � 1) ventilation of oxygen to the lungs � 2) diffusion of oxygen from alveoli to the capillaries � 3) perfusion by arterial blood � 4) diffusion of oxygenated blood from capillaries to cells �Delivery of carbon dioxide � 1) diffusion of carbon dioxide from cells to capillaries � 2) perfusion by venous blood � 3) diffusion of carbon dioxide to alveoli � 4) removal of carbon dioxide during expiration
Oxygen Transport �Alveolocapillary membrane �Ideal medium for oxygen transport �Pressure of oxygen within in alveoli is greater than the pressure within the capillary blood allows for rapid oxygen transport �Oxygen dissolves within the plasma and exerts a pressure (measured as Pa. O 2) �Oxygen moves from the plasma to RBCs and binds with Hgb until Hgb is saturated �Diffusion continues until equilibrium is reached � PAO 2 = Pa. O 2
Alveolar Gas Equation �PAO 2 = Fi. O 2 (Patm-PH 2 O) – Pa. CO 2/R � 0. 21 (760 mm. Hg – 47 mm. Hg) – 40/0. 8 �Sa. O 2 = proportion/percentage of hemoglobin saturated with oxygen 92 -100% �Pa. O 2 = amount of oxygen within the plasma (measured as a pressure/tension) 80 -100 mm. Hg �Pa. CO 2 = amount of carbon dioxide within the plasma (measured as a pressure/tension) 35 -45 mm. Hg
Ventilation and Perfusion �V = Ventilation Q = Perfusion �Dependent on body position �Ventilation exceeds perfusion in the apex �Perfusion exceeds ventilation in the base �More variation between the apex and the base occurs related to perfusion �V/Q ratio is higher in the apex � 0. 8/1 = 0. 8
Ventilation and Perfusion
V/Q Mismatch �An imbalance between blood flow and ventilation �Areas with higher than normal ventilation = high O 2 content and low CO 2 content = V/Q ratio > 0. 8 �Overly ventilated or poorly perfused �Areas with higher than normal perfusion = low O 2 content and high CO 2 content = V/Q ratio < 0. 8 �Inadequately ventilated
�(V) Ventilation �Alveoli filled with air are ventilated. Alveoli that are collapsed or filled with anything besides air are not ventilated. Ventilated alveoli undergo gas exchange; nonventilated do not. �(Q) Perfusion �Alveoli are surrounded by a membrane of capillaries. These capillaries descend from the pulmonary arteries. Capillaries with adequate blood in them are perfused. Perfused capillaries are capable of gas exchange; non-perfused do not.