MECHANICAL VENTILATION SHOZAB AHMED Associate Professor Division of

MECHANICAL VENTILATION SHOZAB AHMED Associate Professor Division of Pulmonary/Critical Care/Sleep Medicine

Objectives • Indications of Mechanical Ventilation • Modes of Mechanical Ventilation • • • Assist control (pressure and volume) PRVC Pressure support • Initial and subsequent vent settings • Acute Respiratory Distress Syndrome (ARDS)/Obstructive lung disease/Metabolic acidosis • Monitoring • Discontinuation of Mechanical Ventilation • Optiflow

Indications o Failure to oxygenate o Failure to ventilate o Airway protection / control of airway o Loss of gag/cough reflex e. g. head injury with GCS<8 (to prevent massive aspiration). o Airway obstruction: acute laryngeal edema – e. g. inhalation burn, Ludwig’s angina, epiglottitis. o Anticipated loss of control of the airway: anticipated laryngeal edema– e. g. neck trauma, acute stridor etc. o Increase WOB (RR>35) o Head Injury (to control CO 2) o Surgery or procedures

MODES OF MECHANICAL VENTILATION • Many modes • Depends on multiple variables • how you ventilate the patient
 • Set volume is given")
MODES OF MECHANICAL VENTILATION • Assist Control (volume targeted) • Set volume is given every time the ventilator is triggered (pressure is going to be variable) • • • Every breath (pt or machine triggered) will get the set TV If no triggering tidal volumes will be delivered at the preset respiratory rate Set RR and Tidal volume (MV) Set PEEP and Fi. O 2 (oxygenation) PT may trigger at a faster rate • By generating certain amount of negative insp. Pressure • By decrement in the circuits baseline flow

MODES OF MECHANICAL VENTILATION • Set pressure is given every time the ventilator is triggered (Volume is variable) • • • Every breath (pt or machine triggered) will get the same pressure If no triggering tidal volumes will be delivered at the preset respiratory rate Set RR, and Pressure (MV) Set Fi. O 2 and PEEP (oxygenation) PT may trigger at a faster rate • By generating certain amount of negative insp. Pressure • By decrement in the circuits baseline flow
 • Pressure mode in which a target tidal volume is set")
PRVC (VC plus) • Pressure mode in which a target tidal volume is set and the computer generates the appropriate pressure to reach that tidal volume. • Probably has a place in the ICU, but most commonly used (at least at UNMH) to reduce vent alarms. • Question why the RT suggested it?
 • Set PS, Fio 2,")
MODES OF MECHANICAL VENTILATION • Pressure support ventilation (PSV) • Set PS, Fio 2, PEEP • Patient must be awake to initiate a breath • SBT/Intubated for airway control
 • Depends on the underlying physiology • ARDS •")
VENT SETTINGS (initial and subsequent) • Depends on the underlying physiology • ARDS • Obstructive lung disease • Metabolic acidosis • Remember • TV × RR = MV that determines CO 2 and PH • PEEP and Fio 2 determines oxygenation

ARDS

PATHOPHYSIOLOGY Ware et al, NEJM 2005

HYPOXEMIA IN ARDS • Shunt is due to alveoli that are collapsed and perfused but receive no ventilation


MECHANICAL VENTILATION • ARDS net protocol • Randomized, prospective controlled trial in ARDS to examine the effect of low vs. high tidal volume ( 6 ml/kg IBW vs. 12 ml/kg IBW) • protective lung ventilation using a tidal volume of 6 ml/kg of ideal body weight, high PEEP and permissive hypercapnia had a lower 28 days mortality rate. 31 vs 39. 8%

ARDSnet website

MECHANICAL VENTILATION • Low-tidal-volume ventilation can result in an increase in the partial pressure of carbon dioxide to above the normal range (permissive hypercapnia) • Can be offset somewhat by increasing the respiratory rate

QUESTION • 32 y. o. female with CAP and severe ARDS. You decided to place patient on the AC/VC mode with the following settings • TV-300 6 cc/kg IBW, RR-12, Fio 2 -60%, PEEP-14 • ABG 7. 11/52/68/20 • You want to improve the ventilation. Which of settings on the ventilator you would choose to improve ventilation? • • Increase PEEP and Increase Fi. O 2 Decrease PEEP and Increase Fi. O 2 Increase RR and same TV Decrease RR and decrease TV

QUESTION • 25 y. o. male with poorly controlled asthma is admitted with asthma exacerbation, got intubated in the ER. His PH was 7. 2 and PCO 2 was 58 hence his RR was increased to 32 • TV 350, RR 32, Fio 2 40% and PEEP of 12 • ABG 7. 11, 62, 92, 20 • What would you do? A. Increase the TV, keep the same RR B. Decrease the RR and keep the same TV C. Decrease the RR, decrease the PEEP D. Increase the RR and increase the TV

OBSTRUCTIVE LUNG DISEASE • COPD and Asthma • High resistance/Compliance not an issue • AC volume targeted: • Low TV, Low RR, Low PEEP, and Fi. O 2
 • You get ABG 30 mins")
MONITORING • ABG (PH, Oxygen, Pa 02/Fio 2) • You get ABG 30 mins after TV or RR change/PEEP and Fio 2 only if sats are not correlating

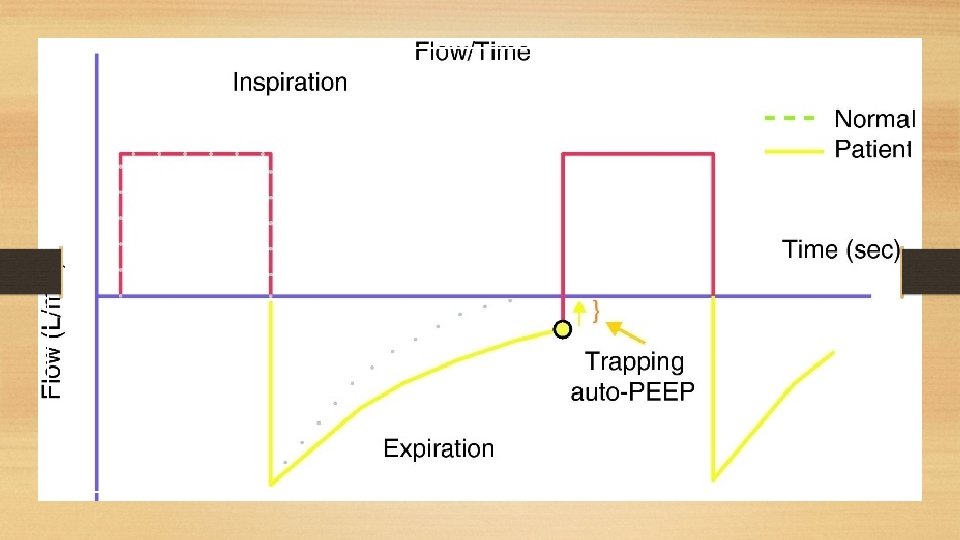
MONITORING • • Peak pressures Plateau pressures Lung compliance Auto-PEEP

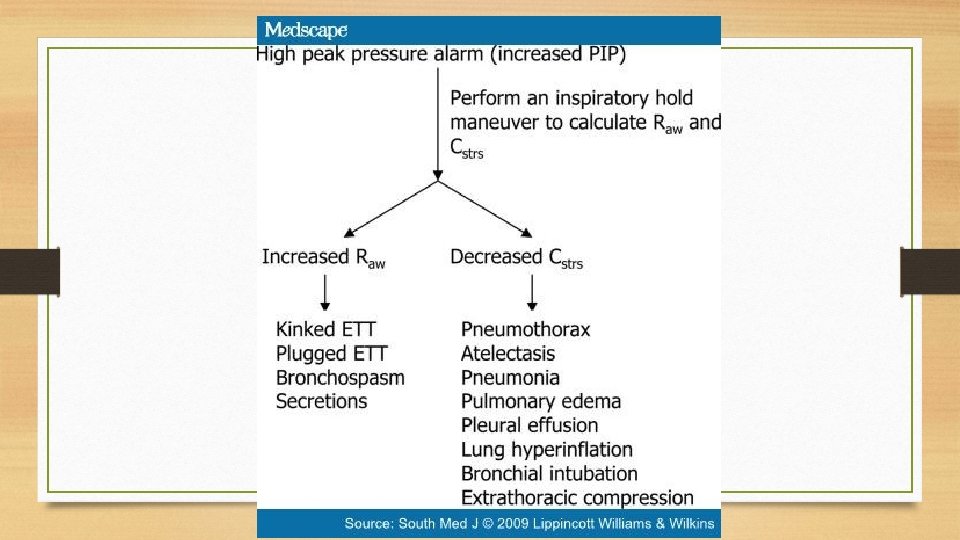
QUESTION • PT with CAP and ARDS intubated, on AC/VC mode. Respiratory therapist informed you that the patient peak pressure has been alarming. Peak pressures are 55, were 30 before. Pt plateau pressure are now 48, 22 before. Which of the following is likely to be causing the increase in the Peak and Plateau pressures? A. B. C. D. Pneumothorax Kink in the vent circuit Pt biting on the tube Increased secretions
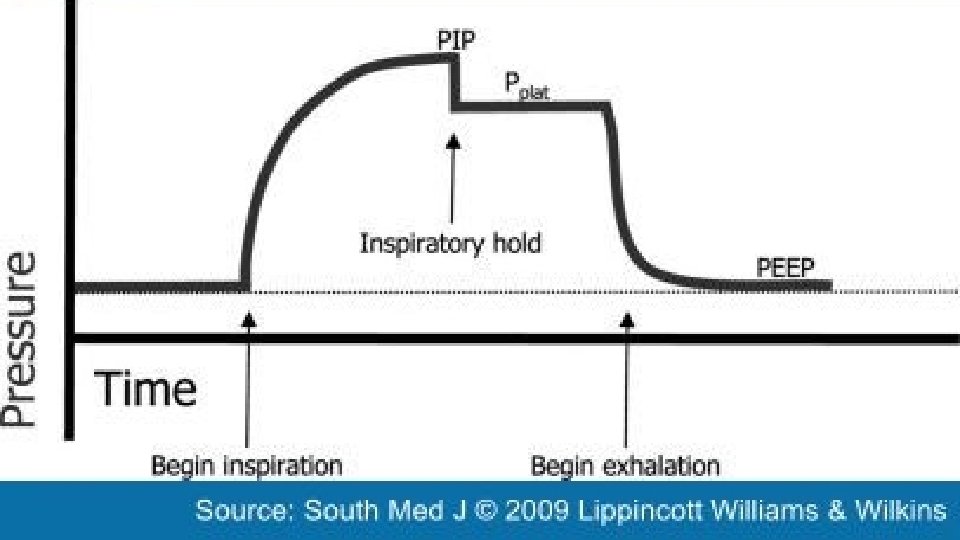

PEAK PRESSURE • Maximal airway pressure recorded at the end of inspiration during PPV in a relaxed patient • Total pressure needed • Resistance (ETT, ventilator circuit, airway) • Elastic recoil of lungs and chest wall

MONITORING • Plateau Pressure: • • • Calculation of the static compliance of the respiratory system Inspiratory hold Airway opening pressure increase from PEEP to PIP Flow is then stopped, thus eliminating airway resistive pressure Airway opening pressure drops from PIP to Pplat Gradient btw PIP and Pplat allows calculation of airway resistance

DISCONTINUATION OF MECHANICAL VENTILATION • • • Can the patient protect their airway? Can the patient produce an adequate cough for secretion management? Is the process that caused them to be intubated resolved? Will they need to compensate for ongoing metabolic acidosis? All patients without contraindications (ARDS, paralytics, severe TBI, etc) should undergo daily spontaneous awakening (SAT) and spontaneous breathing trials (SBT ) • Criteria for extubation: Rapid Shallow Breathing Index < 100 (RR / TV in L), no significant change in hemodynamics with SBT, neuro exam is adequate, if concern for airway edema check for cuff leak • SAT/SBT protocol

OPTIFLOW • Non- invasive • Decrease Dead Space/Generate Positive pressure • You set the Fio 2 and flow. Start at 100% Fio 2 and max flow 60 L/min • Comfortable

QUESTION • 32 y. o. female with no significant PMH, admitted with CAP, got intubated in the ER. She is on AC/VC mode with TV of 6 cc/kg/IBW, RR of 35. Fio 2 of 100% and PEEP of 14 ABG reveals • PH – 7. 21, PCO 2 – 55, Pa. O 2 – 65, HCO 3 – 18 • At this time you would • A. Increase the TV • B. Decrease the PEEP • C. Decrease the RR • D. Do nothing at this time

SUMMARY • • • Consider the underlying physiology when setting up the vent LTV ventilation for ARDS Keep plateaus less than 30 Allow permissive hypercapnia in ARDS Don’t forget SATs/SBTs Early discontinuation of mechanical ventilation is the goal

• QUESTIONS? ?
- Slides: 33