Antihypertensives Anticoagulants and Antidepressants Important Dental Implications Ann

 be able to do after this talk �How")




")

, eventually causes HF")
 �Angiotensin II")









 This endocrine pathway works to maintain blood")
 Effects of Angiotensin II 1. 2. 3.")




 �nifedipine (Procardia) �diltiazem (Cardizem) exception")
 Mechanism: prevents Ang II from binding to")


















 Mechanism: reversible or irreversible inhibitors of monoamine oxidase found in")



 Mechanism of Action: Inhibit reuptake of NE, serotonin and dopamine into")

 �Not approved for depression in children due to suicide risk")

 Agitation")
 Indications: depression, OCD, panic, PTSD, menstrual-related mood disorders, anxiety � Adverse:")
![SNRIs �Serotonin-norepinephrine reuptake inhibitors �Increase [5 -HT] and [NE] in synapses �Indication: depression, chronic](https://slidetodoc.com/presentation_image_h2/7295896a4712b04e918867c91df13220/image-67.jpg "SNRIs �Serotonin-norepinephrine reuptake inhibitors �Increase [5 -HT] and [NE] in synapses �Indication: depression, chronic")
 �atypical antidepressant �exercises its effect by preventing the reuptake of")
 �Don’t take with MAOIs �Scariest")
. __ a. MAOI 2. Bupriopion")




")


- Slides: 78
Antihypertensives, Anticoagulants, and Antidepressants: Important Dental Implications Ann R. Witham, D. V. M.
Learning Objectives: What you will (hopefully) be able to do after this talk �How to perform risk assessment �How to know when to refer �How to manage and prevent complications when treating patients on: �Antihypertensive medications �Anticoagulants �Antidepressants
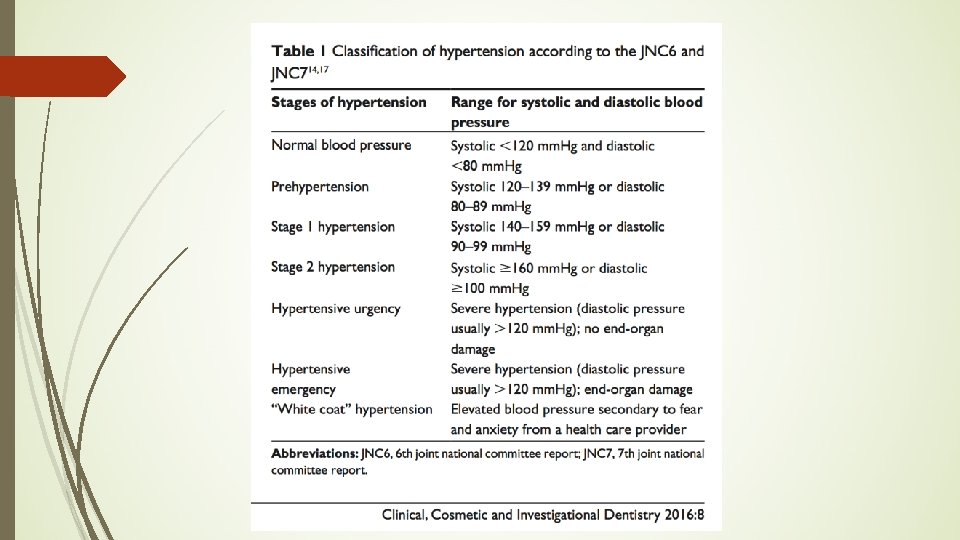
Hypertension: The Silent Killer. Hypertension defined: �Chronic illness, affects > 1 billion worldwide �One of leading risk factors for cardiovascular disease mortality �Systolic BP of 140 mm Hg or diastolic BP ≥ 90 mm Hg �BP readings elevated on at least 2 occasions with or without provocation
Two Main Types of Hypertension �Primary: 90 -95% of all �Secondary: caused by � vascular diseases � Cushing’s syndrome �Sleep apnea, hormonal dysfunction, substance abuse, alcohol consumption, contraceptive use, and chronic kidney disease
Risk Factors for Primary Hypertension? �How many can you name? �Shout out!
Risk Factors � Diabetes � Low education � Reduced nephron number � Socioeconomic status � Family history � Obesity � Age � Race � Contraceptive use/menopause � Personality traits/depression � Excessive alcohol consumption � Hypovitaminosis D � Dyslipidemia � Tobacco use � High sodium diet � Stress � Physical inactivity
BP = Cardiac Output x Peripheral Resistance BP = (Heart Rate x Stroke Volume) x Peripheral Resistance To alter BP, you must alter either HR, SV, or PR.
Key Regulators of Blood Pressure �Sympathetic nervous system �Renal system related to blood volume �Renin angiotensin aldosterone mechanism Antihypertensive drugs act on one or more of these control mechanisms.
Consequences of Hypertension �Damages vasculature. �Damages major organs ( including kidneys), eventually causes HF �Increased morbidity and mortality
Main Categories of Antihypertensives � Diuretics – �Beta-blockers �Angiotensin-converting enzyme inhibitors (ACEI’s) �Angiotensin II receptor blockers �Calcium channel blockers (CCB’s) �Alpha blockers �Alpha 2 agonists �Vasodilators �Others!!
Diuretics �How do they work? �Increase urine production decrease blood volume decrease stroke volume (SV) decrease blood pressure
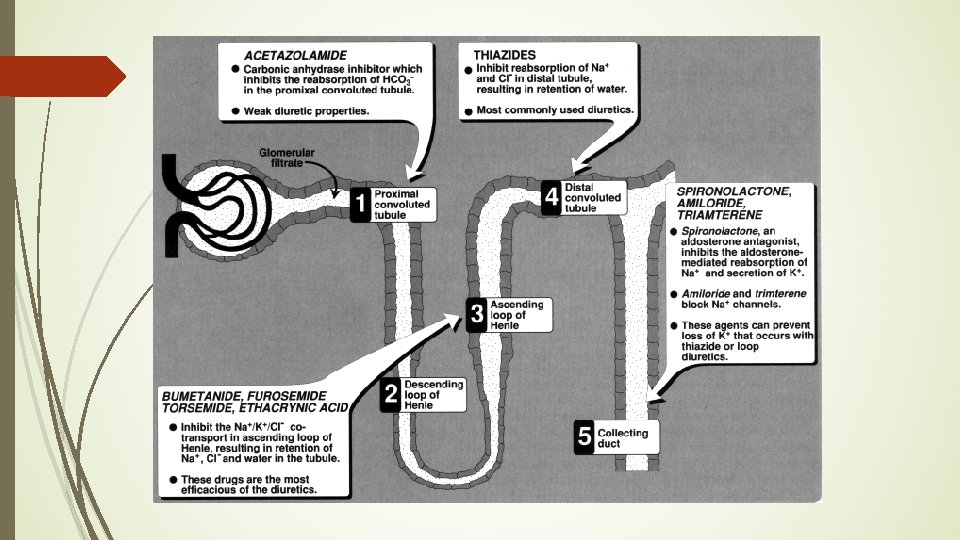
Diuretics �Act by increasing the amount of sodium ions and water that are excreted by the kidneys into the urine �Three major classes of diuretics �Thiazides �Loop diuretics �Combinations
Thiazides: Adverse Effects and Drug Interactions �Hypotension �Hypokalemia (increases chance for arrhythmias, especially with digoxin toxicity) �Hyperglycemia, hyperlipidemia, hypercalcemia �Gout (hyperuricemia): inhibits uric acid secretion �NSAIDs can reduce antihypertensive effect of thiazides �Crossover allergies with sulfa antiinfective drugs possible because thiazides are sulfonamides �Caution with epinephrine in patients taking thiazides and digoxin
Loop Diuretics �Pharmacologic class: loop diuretic �Prevents chloride reabsorption in loop of Henle; greatly increases urine output. �Increases K+, Mg+2, Ca+2 and uric acid excretion �Prototype: furosemide (Lasix) �Indications �Hypertension �Edema
Potassium-Sparing Diuretics � Pharmacological class: K+-sparing diuretic � Used in combination with thiazides � Counteracts the effects of thiazides on potassium loss � Pharmacologic effects: decreases K+ excretion while increases Na+ excretion (increasing urine production) � Prototype: spironolactone (Aldactone) � Combination drugs: � HCTZ with triamterene (Dyrenium) = (Dyazide, Maxzide) � HCTZ with spironolactone (Aldactone) = (Aldactazide) � Indications: �hypertension �hypokalemia
Antiadrenergic Drugs- alpha and beta blockers �Act by inhibiting sympathetic activity �Decrease HR and contractility Decrease cardiac output decrease blood pressure �Sympathetic NS controls blood pressure by �Increasing HR �Vasoconstriction �Increasing contractility of heart �Examples: �Alpha adrenergic blockers �Beta adrenergic blockers
Alpha Adrenergic Blockers �Competitive inhibitors of norepinephrine and epinephrine at alpha adrenergic receptors. �Leads to vasodilation of arteries/arterioles �Decrease PR! �Examples: �prazosin (Minipress) �terazosin (Hytrin) �doxazosin (Cardura)
Beta Adrenergic Blockers � Competitive inhibitors of NE and Epi at beta adrenergic receptors � Leads to decreased HR and decreased contractility of heart � Examples: � propranolol (Inderal) � atenolol (Tenormin) � metoprolol (Lopressor) � esmolol (Brevibloc) � retaxolol (Kerlone) � penbulolol (Levatol) � sotalol (Betapace) � risoprolol (Zebeta)
ACE Inhibitors = Angiotensin Converting Enzyme Inhibitors �Used in persons with normal renal function �Pharmacologic effects: �Inhibits formation of angiotensin II, thus decreasing vasoconstriction = causing vasodilation �Decreases aldosterone secretion decreasing sodium retention and water retention = causing sodium elimination and water elimination, decreasing blood volume and decreasing blood pressure
Blood Pressure Regulation o Renin-Angiotensin System (Renin-Angiotensin-Aldosterone) This endocrine pathway works to maintain blood volume in order to maintain BP. 1. 2. 3. Kidney (JG Apparatus cells) detect decrease in blood volume secrete Renin into blood. Renin, an enzyme, converts circulating Angiotensinogen to Angiotensin I. As Angiotension I circulates in the blood through the lungs, an enzyme on the surface of pulmonary capillary endothelial cells, Angiotensin Converting Enzyme (ACE), converts Angiotensin I to Angiotensin II: an active hormone. Renin Angiotensinogen ACE Angiotensin II
Blood Pressure Regulation o Renin-Angiotensin-Aldosterone System (continued) Effects of Angiotensin II 1. 2. 3. 4. Increased secretion of aldosterone by adrenal cortex. Increased secretion of ADH by posterior pituitary. Increased vasoconstriction (___ PR) Increased thirst center activity. (__ Body fluids __ SV)) RESULTS: Increased reabsorption of Na+ in the DCT & CT of renal tubule. Increased reabsorption of water in the DCT & CT of renal tubule. INCREASES BLOOD VOLUME INCREASED SV HR x SV x PR BP
Angiotensin II causes the secretion/production of which 2 hormones? a. Renin and aldosterone b. Aldosterone and ADH c. Angiotensin I and renin d. Cortisol and insulin e. Estrogen and testosterone
ACE Inhibitors� Side effects � Hypotension � Dry cough � others include loss of taste, rash, jaundice, hyperkalemia, renal damage � Examples: all end in –pril � enalapril (Vasotec) � captopril (Capoten � lisinopril (Zestril) � quinapril (Accupril) � ramipril (Altace) � moexepril (Univasc) � fosinopril (Monopril) � renzapril (Lotensin
Calcium Channel Blockers �Mechanism: inhibits entry of calcium into cells. �Bottom line: Decrease heart rate & contractility and decrease vasoconstriction Decrease CO and PR Decrease blood pressure �Also leads to decreased vasoconstriction �Decreased HR �Decreased contractility
Calcium Channel Blockers: Pharmacologic Effects/ Indications �Coronary and peripheral vasodilation �Decreased HR �Decreased contractility Clinical Indications: HTN arrhythmias angina
Calcium Channel Blockers �Examples: “rap” and “dip” �verapamil (Isoptin) �nifedipine (Procardia) �diltiazem (Cardizem) exception �nisoldipine (Sular) �amlodipine (Norvasc) �nicardipine (Cardene) �felodipine (Plendil)
Angiotensin II antagonists e. g. Losartan (COZAAR) Mechanism: prevents Ang II from binding to its receptor Effects - same as ACE inhibitor without the bradykinin effect Adverse effects – same AE’s as ACE inhibitor without the dry cough and angioedema
Match the antihypertensive to its category, just for fun! 1. Lisinopril ______ a. Calcium channel blocker 2. Verapamil ______ b. Potassium sparing diuretic 3. Prazosin ______ c. Loop diuretic 4. Metoprolol ______ d. ACE inhibitor 5. Furosemide ______ e. Beta blocker 6. Spironolactone ______ f. Angiotensin II blocker 7. Hydroclorothiazide ______ g. Alpha-1 blocker 8. Losartan h. Thiazide diuretic ______
Which are the most common ones? ?
Management of Dental Patients Taking Antihypertensive Drugs �Adverse Effects: �Xerostomia �Dysgeusia �Gingival enlargement (Calcium channel blockers) �Orthostatic hypotension �Lichenoid reactions
Drug Interactions of Concern �Common drug interactions with antihypertensives often occur with drugs the dental professional prescribes. � Local anesthetics with or without epinephrine �Conscious sedation of anxious patients �NSAIDS and antifungals are commonly prescribed
Hypertensive Crisis- Emergency �Medication noncompliance is one of most significant factors �Thorough history, always take BP reading. Severe increase >180/120 mm Hg or acute rise after previously normal baseline can be caused by �Neurologic deficits due to stroke �Nausea/vomiting from hypertensive encephalopathy and increased intracranial pressure �Chest discomfort from MI or aortic dissection �Back pain from aortic dissection �Dyspnea from pulmonary edema �Pregnancy hypertension; pre-ecclampsia
Complications associated with use of vasoconstrictors � Epinephrine – hemostatic agent with local anesthetics �Also used in retraction cord to improve overall vision and control hemorrage in taking impressions for crown and bridge � Risks of using epinephrine in hypertensive population �Acute hypertensive or hypotensive episodes, angina pectoris, arrhythmias, and MI �Epi in local anesthetics can affect hemodynamics of a patient. (recent study, 2015) � 1: 80, 000 can affect SBP and DBP as well as heart rate � 1: 100, 000 can exacerbate SBP and heart rate � 1: 200, 000: exacerbate heart rate
Continued, vasoconstrictor complications �Continued: consider concentrations of 1: 200, 000 before tooth extraction to prevent significant hemodynamic changes �Use of impregnated retraction cord has been discouraged in patients with uncontrolled hypertension � 0, 04 mg epi total dose for those with CV disease.
Drug interactions with vasoconstrictors �Epinephrine interacts with some antihypertensive agents �Beta blocker + epi possible hypertension and relex bradycardia �Diuretics produce hypokalemia; with epi can be exacerbated, causing arrhythmia �Epinephrine + cocaine blood pressure spikes and fatal dysrhythmias.
Bleeding Issues �Elevated BP can cause excessive bleeding �In patients who are on anticoagulants, if INR (international normalized ratio) value is <4, no need to stop anticoagulant therapy before minor surgery. �For aspirin or other antiplatelet drugs like clopidogrel, continue with procedure even if minor surgery �Various hemostatic agents can be used in the above cases
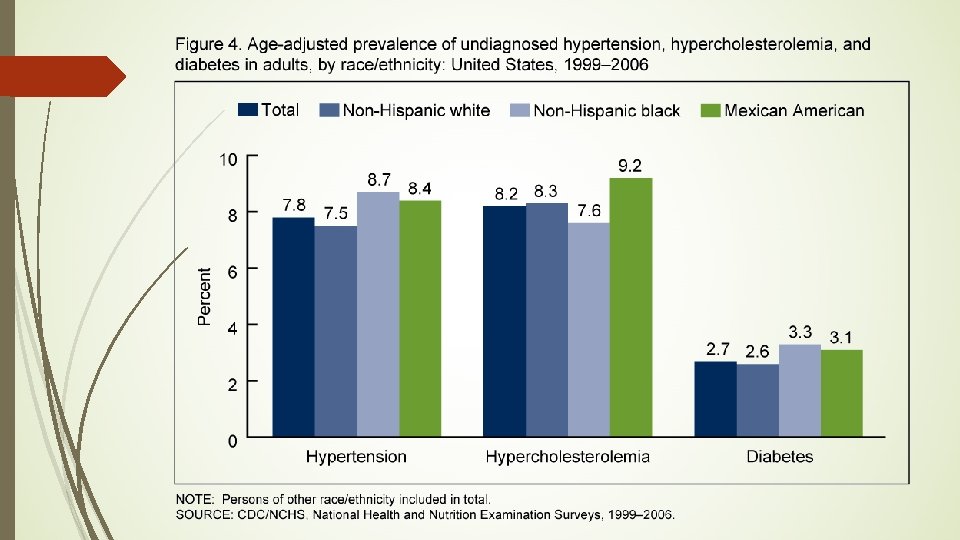
Racial/Ethnicity disparity-associated hypertension �Prevalence of hypertension in African Americans is highest in the world, 41. 4% of hypertensive patients. �Cause? �Access to care, poor diagnoses �Poor treatment/medication noncompliance �Socioeconomic status �Still it’s duty of health care provider to aid in prevention and education of hypertension
Your client’s BP is 181/120. This person is experiencing: a. Stage I hypertension b. Stage II hypertension c. Pre-hypertension d. Normal blood pressure e. Hypertensive crisis f. ”White coat” hypertension
Break
Pharmacology of Antidepressants: Clinical Considerations
Introductory information on antidepressant use �Widespread use: 21% of the 1, 800 patient dental records reviewed showed antidepressant use. (Josephe et al, 2003). Watch for increased evidence of oral lesions! �Used in patients of all ages! �Used to treat many psychiatric diseases (depression, affective disease, insomnia, anxiety, panic syndrome, bipolar) �Used to treat other medical conditions like rheumatoid arthritis, dietary disorders, fibromyalgia, migraine, trigeminal neuralgia, premenstrual tension (Keene et all, 2003)
Clinical Depression – sometimes confused with other causes Major depression, situational depression � postpartum depression, premenstrual dysphoric syndrome, seasonal affective disorder �side effects of some drugs (glucocorticoids, levodopa, oral contraceptives) mimic depression �B-vitamin deficiencies, thyroid disorders, Alzheimer’s disease may be misdiagnosed as depression �alcoholism and drug abuse may be misdiagnosed as depression or can be contributing factors to the development of depression
Depression
Antidepressants �BLACK BOX WARNING: increased risk of suicide at the beginning of treatment, especially in children
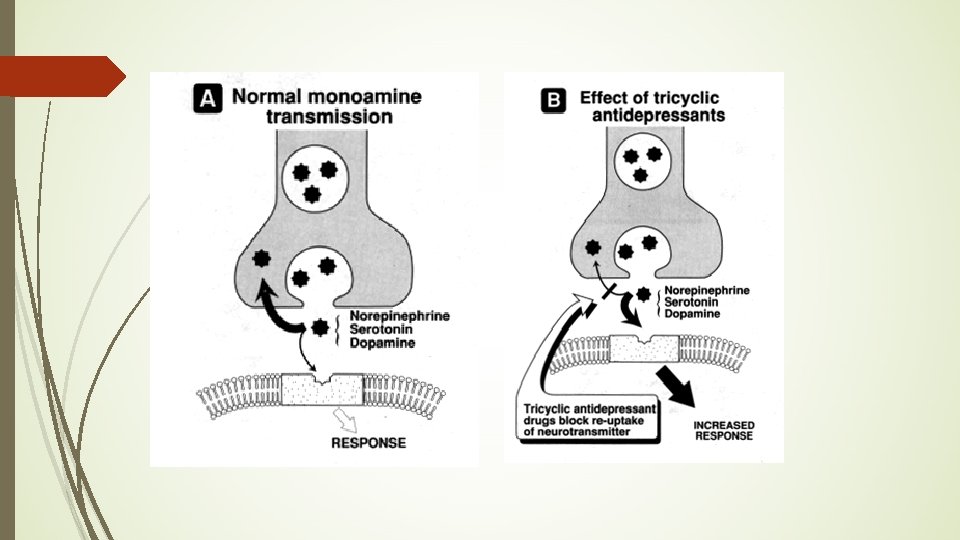
Antidepressants THEORY of Mechanism of Action: work by increasing the concentration of neurotransmitters (serotonin, norepinephrine, and/or dopamine) in CNS synapses Monoamine oxidase inhibitors (MAOIs) Tricyclic antidepressants (TCAs) Selective serotonin reuptake inhibitors (SSRIs) Atypicals
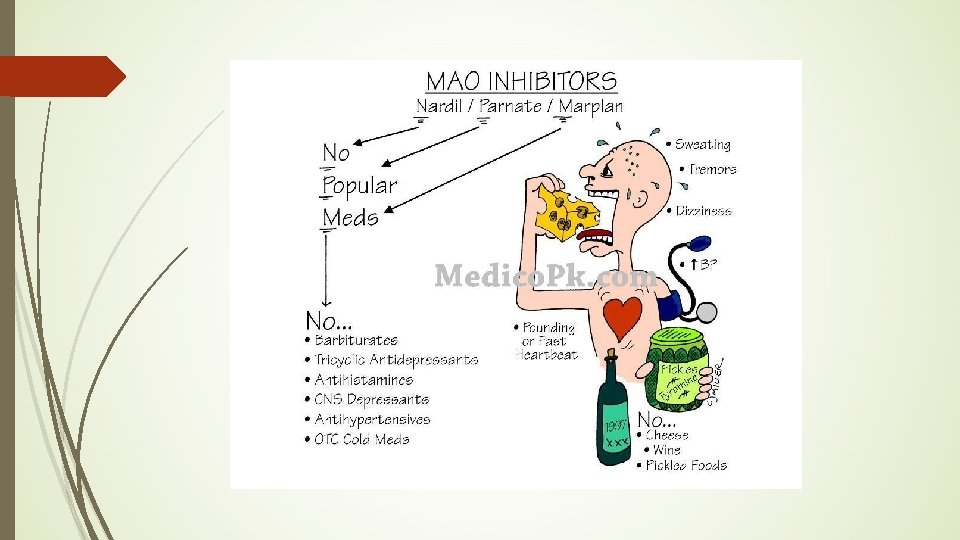
MAO Inhibitors �phenelzine (Nardil) Mechanism: reversible or irreversible inhibitors of monoamine oxidase found in presynaptic neuronal endings - leads to accumulation of NE, dopamine, and serotonin) in presynaptic endings that leak out and increase interaction with receptors - Elevates mood due to increased neurotransmitters -MAO is an intracellular enzyme Other examples: tranylcypromine, moclobemide and selegiline.
MAO Inhibitors � Treats depression when other drug classes are ineffective Adverse effects: Orthostatic hypertension, headache, insomnia, diarrhea Drug-drug and Drug-Food interactions! -Hypertensive crisis w/other antidepressants (life-threatening “serotonin syndrome”) -Hypertensive crisis w/sympathomimetics -Hypertensive crisis w/food containing tyramine (avocados, bananas, cheese, raisins, beer and wine, liver, salami, hot dogs, sausage, soy sauce, others) can lead to MI and CVA
MAO Inhibitors: more concerns!!! Serotonin Syndrome: hyperthermia, rigidity, autnomic instability, agitation, delirium, and coma. MAOIs take at least 14 days to be safely eliminated before interacting drugs can be administered
MAO Inhibitors: Even MORE Adverse reactions continued: Hypotension w/antihypertensives Hypoglycemia w/insulin or antidiabetics Others Depression may make compliance difficult! MAOIs can take 4 to 8 weeks to see effects
Tricyclic antidepressants (TCAs) Mechanism of Action: Inhibit reuptake of NE, serotonin and dopamine into neuronal presynaptic endings increasing neuronal action potentials/activity Indication: Major depression OCD, panic Result: Elevated mood Onset is slow - two to three weeks Can lead to compliance problems
Tricyclic antidepressants �Less dangerous and have fewer adverse reactions than MAOIs �Adverse Reactions: �Orthostatic hypotension �Cardiac dysrhythmias (rare) �Sedation on initial treatments �Anticholinergic effects (dry mouth, blurred vision, etc. ) �Drug-Drug: Do not administer with MAOIs � Special considerations: may unmask mania, narrow therapeutic index
TCA drugs �imipramine (Tofranil) �Not approved for depression in children due to suicide risk �Highly metabolized by liver: watch for drug -drug interactions with drugs that affect liver metabolism and drugs that are also highly metabolized. Also, idiosyncratic metabolism rates can affect plasma levels. �Other examples =Amitriptyline, clomipramine and nortriptyline
SSRIs Mechanism: Selective inhibition of reuptake of serotonin by the presynaptic neuron -Serotonin (5 -HT) is involved in sleep cycles, pain perception, and emotional states Result: elevated mood First choice drug for treating depression due to scarcity of adverse reactions Therapeutic effect - similar to TCAs Uses - additional uses over TCAs, e. g. obsessivecompulsive disorder
SSRIs Adverse effects: Nausea, headache, weight gain Insomnia Sexual dysfunction (up to 70%) Agitation No cardio toxicity, fewer anticholinergic effects Response observed in less time than TCAs Drug-drug interactions: do not administer with MAOIs, TCAs, or lithium May effect digoxin and warfarin concentrations Patients should avoid alcohol
SSRI �sertraline (Zoloft) Indications: depression, OCD, panic, PTSD, menstrual-related mood disorders, anxiety � Adverse: see list for class �dry mouth �Not approved for pediatric use, except OCD �Others drugs in class: citalopram (Celexa), fluoxetine (Prozac), fluvoxamine (Luvox), paroxetine (Paxil)
SNRIs �Serotonin-norepinephrine reuptake inhibitors �Increase [5 -HT] and [NE] in synapses �Indication: depression, chronic pain (fibromyalgia) �May be added to SSRI therapy �Venlafaxine (Effexor), duloxetine (Cymbalta), mirtazapine (Remeron), trazodone and nefazodone �mirtazapine (Remeron)- can cause oral ulcers, early stage of bone marrow suppression!
Others: �Bupropion (Zyban, Wellbutrin) �atypical antidepressant �exercises its effect by preventing the reuptake of noradrenalin and dopamine at the synaptic gap, thus facilitating neural transmission
Which antidepressant group? �Oldest antidepressant: �Highest therapeutic index (safest) �Don’t take with MAOIs �Scariest side effects and drug interactions �Can also be used for smoking cessation �Don’t have a wine and cheese party with this one:
Match the drug with its category! 1. Paroxetine (Paxil). __ a. MAOI 2. Bupriopion (Wellbutrin) __ b. SNRI 3. Duloxetine (Cymbalta) __ c. TCA 4. Imiprimane (Tofranil) __ d. SSRI 5. Phenelzine (Nardil) __ e. Atypical
People who take psychotropic drugs: �Experience lethargy, fatigue and lack of motor control and memory that may impair the individual’s ability to practice a good oral hygiene technique (Mc. Clain et al. , 1991). �Many antidepressants have the side effects of dry mouth, diminished salivary flow speed and/or alteration in saliva composition
Other effects on salivary glands can produce: �Sialoadenitis �Gingivitis �Dysgeusia �Glossitis �Tongue edema and discoloration �Stomatitis
Interesting Studies �Major tooth losses occur due to: �lack of interest in oral hygiene �preference for carbohydrates (probably because of the reduction of serotonin in the SNC) �preference for sweetened foods because of alterations in the sense of taste (dysgeusia) due to: �diminishment of saliva release �high lactobacillus counts
Additional interesting studies on antidepressant use: �High risk of developing periodontal disease because: �neglected oral hygiene �increased smoking and altered immune response from xerostomia leads to increased bacterial colonization, causing collapse of the peridontium.
Other clinical manifestations of SSRI’s and atypical antidepressants �Movement disorders like: �Bruxism (tooth grinding) can aggravate periodontal status. �Caused by increased extrapyramidal serotonin levels, inhibiting the dopaminergic pathways that control the movements.
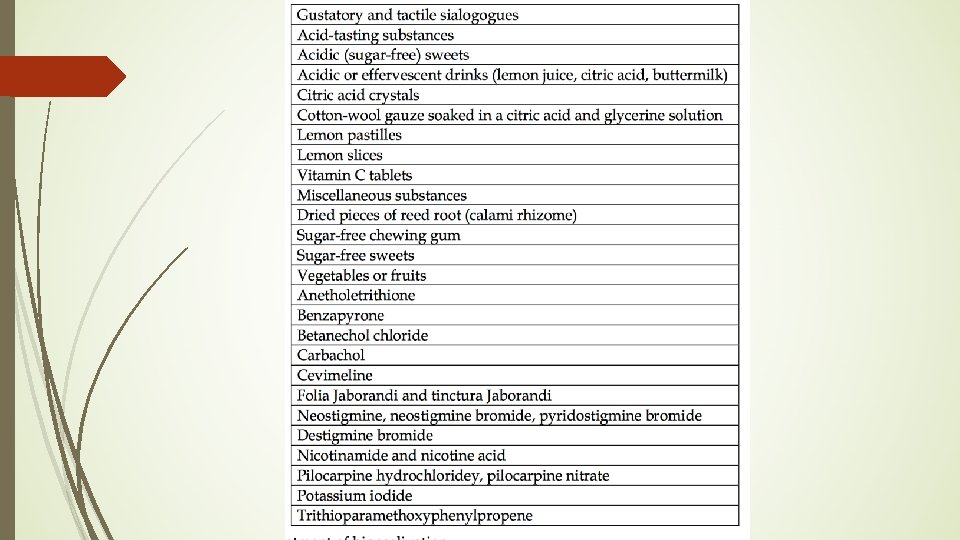
Treatments for Hyposalivation Pilocarpine, which stimulates muscarinic cholinergic receptors Salivary replacement therapies, as well as use of salivary, masticatory and pharmacological stimulants.
References page 1. Dental management in patients with hypertension: challenges and solutions, Southerland, Gill, Gangula, Halpern et al; Clinical, Cosmetic and Investigational Dentistry 2016: 8 p. 111 -120 2. Antidepressants: Side Effects in the Mouth. www. intechopen. com 3. Witham, A. Personal Power. Point slides from Pharm for DH, 2017 4. Haveles, Elena B. , Applied Pharmacology for the Dental Hygienist, 7 th edition