N u mb er o f p a


N u mb er o f p a t i en t s Major Hemorrhagic Events (Acute Phase) No significant increase in rate of major hemorrhage 60 NS UFH Enoxaparin 40 NS NS 20 0 ESSENCE n = 3171 TIMI 11 B n = 3910 UFH, unfractionated heparin; NS, not significant TESSMA n = 7081 Antman EM et al. Circulation 1999; 100: 1602 -8

GUSTO V Benefit vs. risk Severe / moderate hemorrhage Abciximab + reteplase Death or re-MI 7. 4% 4. 6% D = 2. 3% P < 0. 001 Reteplase 6 D = 1. 4% P = 0. 001 2. 3% 4 2 0 2 4 6 Percentage of patients GUSTO V Investigators. Lancet. 2001; 357: 1905. 8. 8% 8 10

Low-Molecular-Weight Heparin Advantages Increased anti-Xa to anti-IIa activity inhibits thrombin generation more effectively Induces ↑ release of TFPI vs UFH Not neutralized by platelet factor 4 Less binding to plasma proteins (eg, acute-phase reactant proteins) more consistent anticoagulation Lower rate of HIT vs UFH Lower fibrinogen levels Easy to administer (SC administration) Long history of clinical studies and experience, FDA-approved indications Monitoring typically unnecessary Disadvantages § § Indirect thrombin inhibitor Less reversible Difficult to monitor (no a. PTT or ACT) Renally cleared Long half-life Risk of HIT § § § Hirsh J, et al. Circulation. 2001; 103: 2994 -3018. TFPI = tissue factor pathway inhibitor; UFH = unfractionated heparin; SC = subcutaneous; a. PTT = activated partial thromboplastin time; ACT = activated coagulation time. § § §

AT AT IIa Hep LMWH UFH C IIa Xa S Direct antithrombin

Clot Burden in ACS patient

Heparin fails to effectively inhibit Clot-bound Thrombin

Bivalirudin inhibits Clot-Bound and Circulating Thrombin

Bivalirudin Does not activate Platelets

Bivalirudin: Unique mechanism of action overcomes the limitation of Heparin
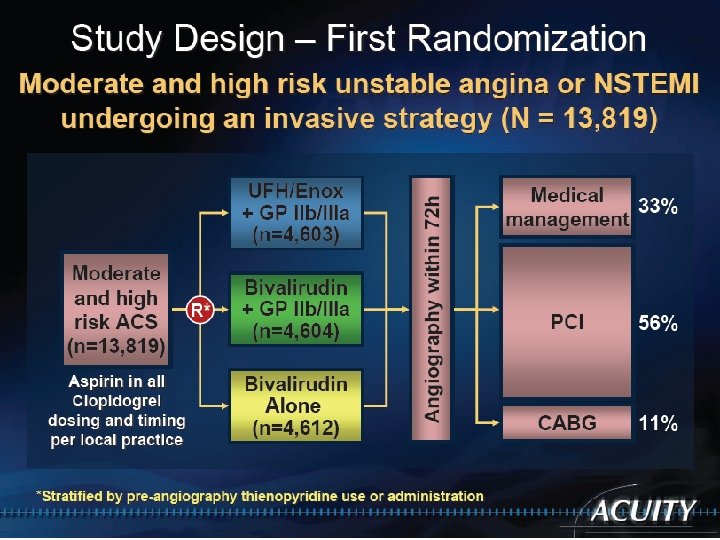
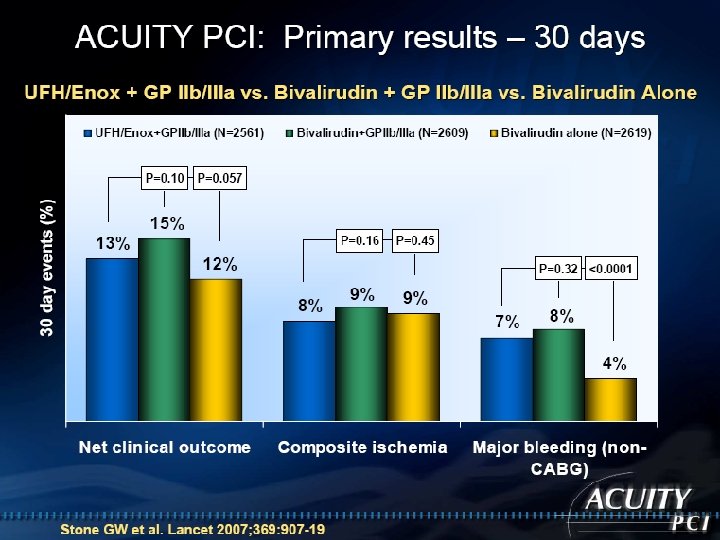
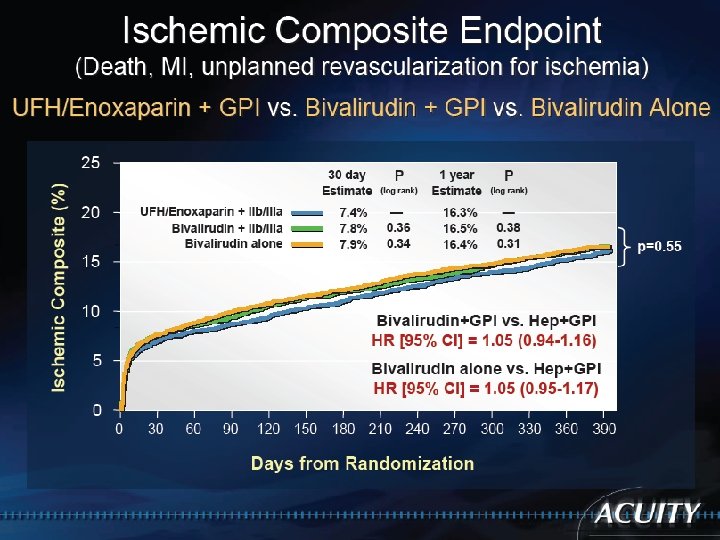
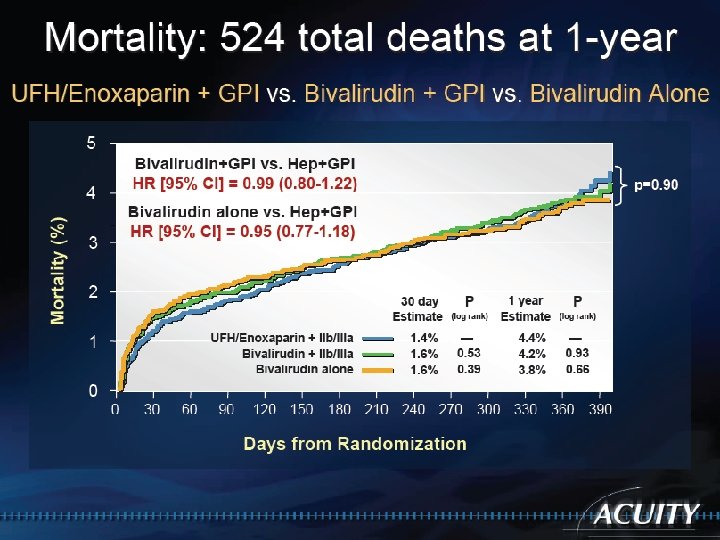
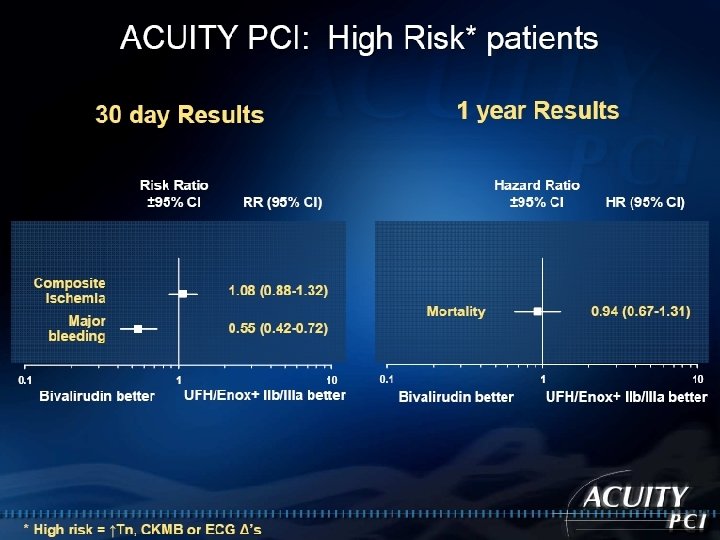

Bivalirudin Advantage Compared to Heparin/Enoxaparin with GP IIb/IIa inhibitors, Bivalirudin monotherapy significantly reduces major bleeding while providing similar ischemic protection, and improves net clinical outcome.

AT C IIa S Hep UFH AT IIa Xa LMWH Direct antithrombin AT Xa Pentasaccharide

Fondaparinux: A Synthetic Factor Xa Inhibitor Intrinsic pathway Extrinsic pathway Antithrombin AT AT Fondaparinux AT Xa Xa II IIa THROMBIN Fibrinogen Adapted with permission from Turpie AGG et al. N Engl J Med. 2001; 344 : 619. Fibrin clot

Key Steps in Coagulation Pathway Intrinsic pathway Extrinsic pathway IXa 1 VIIIa Xa PL Ca 2+ X Inhibition of one molecule of factor Xa can inhibit the generation of 50 molecules of thrombin 2 Xa Va II Ca 2+ PL IIa 50 Fibrinogen Clot 1. Rosenberg RD, Aird WC. N Engl J Med 1999; 340(20): 1555– 64. 2. Wessler S, Yin ET. Thrombo Diath Haemorrh 1974; 32(1): 71– 8.
")
Fondaparinux: A Synthetic Inhibitor of Factor Xa Once daily administration Rapid onset (Cmax/2=25 min) Half life: 15 -18 h. Effects reversible with administration of activated Factor VII (Novoseven®) No liver metabolism Renal clearance No protein binding (other than AT) No reported cases of HIT No dose adjustment necessary in elderly Herbert JM et al. Cardiovasc Drug Rev. 1997; 15: 1. van Boeckel CAA et al. Angew Chem, Int Ed Engl. 1993; 32: 1671. · · · · ·

OASIS-6: Randomized, Double Blind 12, 000 Patients with STEMI < 12 h of symptom onset Inclusion: ST 2 mm prec leads or 1 mm limb leads Exclusion: Contra-ind. for anticoagulant, INR>1. 8, pregnancy, ICH<12 mo. Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late) Stratification UFH not indicated Randomization Fondaparinux 2. 5 mg Placebo UFH indicated Randomization Fondaparinux 2. 5 mg UFH JAMA 2006; 295: 1519 -30

0. 12 Primary Efficacy Outcome Death/MI at 30 Days 0. 06 0. 08 Fondaparinux 0. 02 0. 04 HR 0. 86 95% CI 0. 77 -0. 96 P=0. 008 0. 0 Cumulative Hazard 0. 10 UFH/Placebo 0 3 6 9 12 15 Days 18 21 24 27 30 The OASIS-6 Trial Group. JAMA 2006; 295: 1519 -30

0. 02 0. 04 0. 06 0. 08 0. 10 0. 12 UFH/Placebo Fondaparinux HR 0. 88 95% CI 0. 79 -0. 99 P=0. 029 0. 0 Cumulative Hazard Death or MI 3 or 6 months 0 18 36 54 72 90 108 Days 126 144 162 180 The OASIS-6 Trial Group. JAMA 2006; 295: 1519 -30

Primary: Efficacy: Death, MI, refractory ischemia 9 day • Safety: Major bleeds Risk benefit: Death, MI, refractory ischemia, major bleeds Secondary: Above & each component (especially deaths) at 30 & 180 d • Hypothesis: First test non-inferiority, then test superiority •

Death at 6 Months 0. 04 Fondaparinux 0. 02 HR 0. 89 95% CI 0. 79 -0. 99 p=0. 037 0. 0 Cumulative Hazard 0. 06 Enoxaparin 0 20 40 60 80 100 Days 120 140 160 180

0. 12 Death or MI: 6 Months 0. 06 0. 08 Fondaparinux 0. 02 0. 04 HR 0. 91 95% CI 0. 84 -0. 99 p=0. 036 0. 0 Cumulative Hazard 0. 10 Enoxaparin 0 20 40 60 80 100 Days 120 140 160 180

0. 06 Major Bleeding: 6 Months 0. 04 0. 03 Fondaparinux 0. 01 0. 02 HR 0. 72 95% CI 0. 63 -0. 82 p<<0. 00001 0. 0 Cumulative Hazard 0. 05 Enoxaparin 0 20 40 60 80 Days 100 120 140 160 180

Death, MI, RI or Major Bleeding at 6 Months 0. 10 Fondaparinux 0. 05 HR 0. 87 95% CI 0. 81 -0. 93 p<<0. 00001 0. 0 Cumulative Hazard 0. 15 Enoxaparin 0 20 40 60 80 100 Days 120 140 160 180

Fondaparinux Advantages SC administration Potential exists for ― outpatient management Once-daily administration Predictable anticoagulant response Fixed dose No antigenicity Potentially no need for serologic parameters Does not cross the placenta HIT antibodies do not crossreact Decreased bleeding complications vs UFH or LMWH Disadvantages • • • Difficult to monitor (no a. PTT • or ACT) Long half-life • Catheter thrombosis during • PCI • • • Simoons ML, et al. J Am Coll Cardiol. 2004; 43: 2183 -2190. Yusuf S, et al. N Engl J Med. 2066; 354: 1464 -1476.
- Slides: 38