Anticoagulants Anticoagulants can be classified as Parenteral anticoagulants

Anticoagulants
 Heparin ii) Low molecular weight")
Anticoagulants can be classified as • Parenteral anticoagulants i) Heparin ii) Low molecular weight heparins - Enoxaparin - dalteparin - tinzaparin - ardeparin - nadroparin -reviparin iii) Synthetic heparin derivatives - fondaparinux
 Thrombin inhibitors Parenteral - lepirudin - aratroban - bivalirudin - danaparoid - desirudin")
iv) Thrombin inhibitors Parenteral - lepirudin - aratroban - bivalirudin - danaparoid - desirudin - drotrecogin - dabigatran & rivaroxiban (oral) • Oral anticoagulants i) Coumarin derivatives - warfarin - acenocumarol ii) Indanedione group - phenindione - anisindione

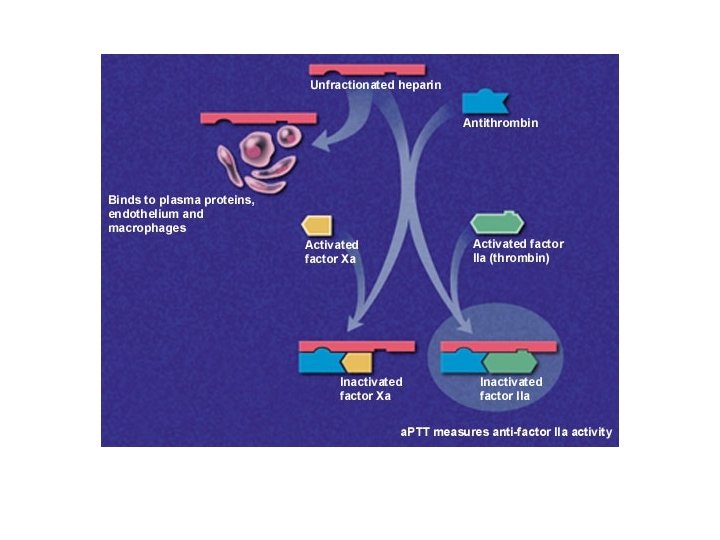
• • • Heparin It is a heterogeneous mixture of sulfated mucopolysaccharides Its anticoagulant activity is attributed to its strong electronegative charge It binds to endothelial cell surfaces Its biologic activity is dependent upon the plasma protease inhibitor (clotting factors) – antithrombin III Anti-thrombin inhibits clotting factor proteases by forming stable complexes with them

• In the absence of heparin these reactions are slow – they are accelerated 1000 times in the presence of heparin • The active heparin molecules bind tightly to antithrombin & cause conformational change in this inhibitor exposes active site for rapid interaction The proteases heparin activated clotting factors

• High molecular weight heparin high affinity for anti-thrombin inhibits coagulation • In higher doses it also inhibits platelet aggregation
 •")
• The duration of action of heparin is short (1 -5 hours) • Hence its dose is so adjusted that the whole blood clotting time is raised to 2 -3 times more than normal or activated thromboplastin time 1. 5 – 2 times • Clotting time ↑↑ 2 -2½ times • Activated thromboplastin time – 1. 5 – 2 times
 intermittent regime 10, 000 units – initially Followed by")
• Given intravenously (IV) intermittent regime 10, 000 units – initially Followed by 5000 -10, 000 units every 4 -6 hours • IV infusion Initially 5000 units in drip tubing Followed by 20, 000 - 30, 000 units daily at the rate of 1000 units/hour • Intramuscular (IM) It is not administered to avoid hematoma formation at injection site

• • • Adverse effects Allergic & anaphylactoid manifestations Bleeding – hemorrhages from peptic ulcer, kidney, hemorrhoids Thrombocytopenia Alopecia Osteoporosis

• • Contraindications Hypersensitivity to drug Active bleeding Active tuberculosis Ulcerative lesion of GIT Hemophilia Thrombocytopenia Infective endocarditis
 It is fractionated heparin with")
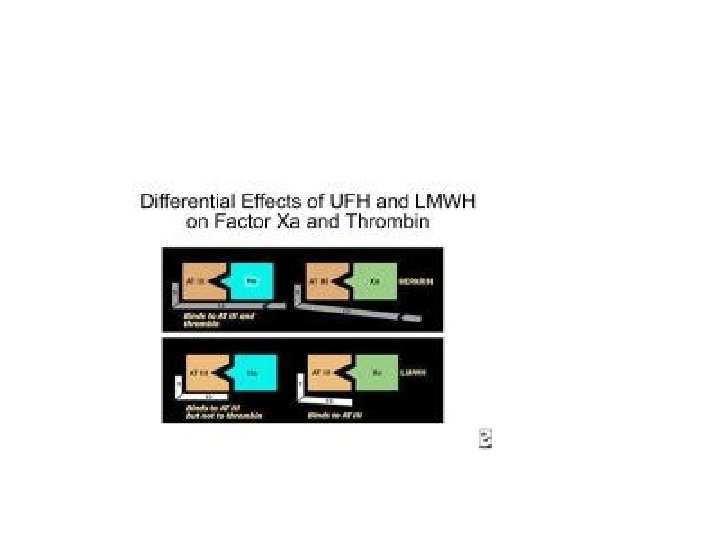
• • • Low molecular weight heparin (LMWH) It is fractionated heparin with a low molecular weight (5000 -40, 000) It has a shorter polymer length & inhibits activated factor X predominantly It has ↓↓ effect on thrombin, platelet function & coagulation in general Thrombocytopenia is ↓↓ frequent Chances of hemorrhage ↓↓
 • ↑↑ bioavailability –variability in")
Advantages of LMWH • Can be given subcutaneously (SC) • ↑↑ bioavailability –variability in response minimized • Equal efficacy • Few bleeding episodes • Longer elimination ½ life - given ↓ frequently once or twice daily • Do not prolong APTT & whole clotting time – response predictable & monitoring not required Dosage & administration • 5000 units SC once or twice daily

Synthetic heparin derivatives Fondaparinux • It is a synthetic pentasaccharide • It causes antithrombin III mediated selective inhibition of factor Xa neutralization of factor Xa ↓↓ thrombin formation • It does not inhibit thrombin by itself due to its shorter polymer length

• • It is administered SC once daily Bioavailability is 100% Half life is 17 -21 hours It has ↓↓ antiplatelet action ↓↓ thrombocytopenia Uses: • Preferred for thromboprophylaxis of hip or knee surgery • Therapy of pulmonary embolism
 Majority of them act by")
• • Thrombin inhibitors Parenteral (hirudin, bivalirudin, argatroban) Majority of them act by binding directly to thrombin & minimizing its effects in the coagulation cascade They do not bind to AT III or to plasma proteins Uses As an alternative to heparin - percutaneous coronary angioplasty - deep vein thrombosis treatment & prevention postoperatively Thrombotic events associated with heparin induced thrombocytopenia

Oral thrombin inhibitors Dabigatran, rivaroxiban • These drugs have become a major discovery in prevention of venous thromboembolism in patients undergoing knee or replacement surgery • They do not require routine coagulation monitoring • They have been found to be as effective & safe as LMWH • They may replace warfarin in future as it has - narrow therapeutic window - dosage adjustments required - potential for drug interactions

Oral anti-coagulants • Coumarin derivatives - warfarin • Warfarin & its analogues act by inhibiting vitamin K reductase as warfarin is similar in structure to vitamin K • It inhibits the synthesis of clotting factors II, VII, IX &X • They interfere with γ carboxylation of glutamic acid residues in clotting factors II, VII, IX and X
 vitamin K reductase Θ warfarin vitamin")
vitamin K reductase Θ warfarin vitamin K (quinone) vitamin K reductase Θ warfarin vitamin K hydroquinone (cofactor in ү carboxylation of clotting factors) (II, VII, IX & X)

• The action of warfarin starts after a delay of 8 -12 hours as it depends on the degradation rate of the coagulation factors already in circulation • Larger initial doses of 0. 75 mgm/kg hasten the anti-coagulation effect Kinetics • It is administered as Na salt • Has 100% bioavailability • Over 99% bound to plasma albumin – small volume of distribution • Has long ½ life – 46 hours

• • Actions Anticoagulant effect Has no anticoagulant effect in vitro unlike heparin Therapeutic action depends on its ability to prolong prothrombin time by suppressing the synthesis of prothrombin, factors VII, IX & X by the liver by competitive inhibition of carboxylation of glutamic acid by vitamin K Coumarin therapy is controlled by estimating prothrombin time of blood Bleeding time unaltered

Drug interactions • A large number of drugs interact with warfarin • They either ↑↑ its activity hemorrhage or ↓↓ its activity therapeutic failure

• • • ADRs Bleeding – most frequent manifestation as hematuria Epistaxis, bleeding gums, echymoses, hemoptysis also noted Hemorrhage induced by warfarin can be reversed by large doses of vitamin K which enables liver to synthesize the clotting factors Fetal toxicity Teratogenic effect Crosses placenta fatal hemorrhage in fetus Cutaneous gangrene Petechiae painful echymoses necrosis/gangrene Dose – warfarin available as 5 mgm tab once daily

Therapeutic uses of anticoagulants • They do not dissolve the clot already formed • They prevent thrombus - extension - recurrence - embolic complications by ↓↓ rate of thrombin formation • Heparin used initially for rapid action • Oral anticoagulants usually started concurrently • Heparin stopped after 6 -7 days when oral anticoagulants take full therapeutic effect

• Uses - prevention & treatment of deep vein thrombosis & pulmonary embolism - myocardial infarction - unstable angina - rheumatic heart disease - cerebrovascular diseases

• • Contraindications Active bleeding Active tuberculosis Ulcerative lesion of GIT Hemophilia Thrombocytopenia Infective endocarditis Pregnancy

- Slides: 28