ANGINA AND MYOCARDIAL INFARCTION Angina pectoris is a


 is termed acute coronary")






 uses a balloon at")











 Infective")
.")









- Slides: 39
ANGINA AND MYOCARDIAL INFARCTION
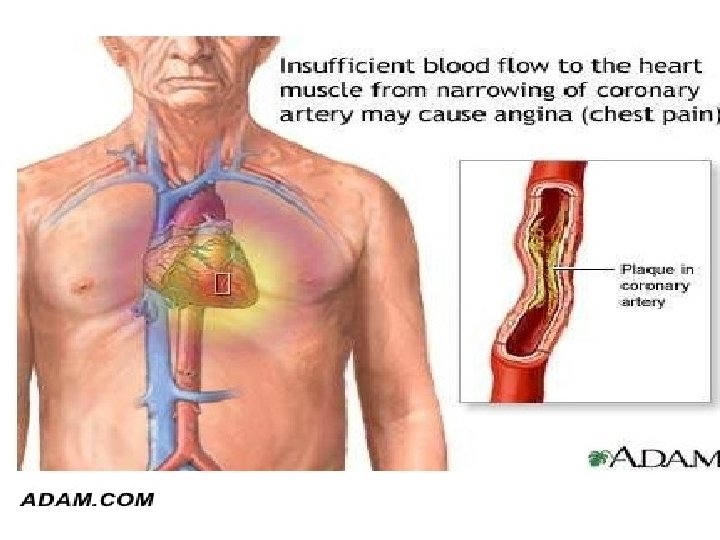
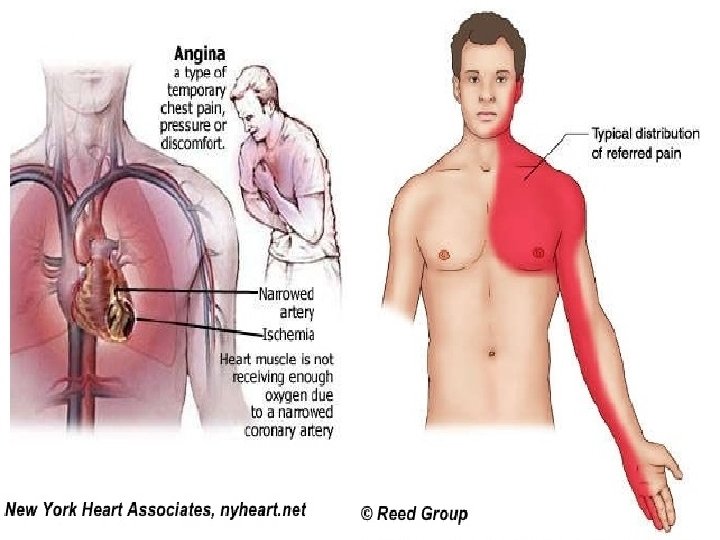
Angina pectoris is a clinical syndrome usually characterized by episodes of pain or pressure in the anterior chest. The cause is usually insufficient coronary blood flow which results in a decreased oxygen supply to meet an increased myocardial demand for oxygen in response to physical exertion or emotional stress.
Key Points The continuum from angina to myocardial infarction (MI) is termed acute coronary syndrome Symptoms of acute coronary syndrome are due to an imbalance between myocardial oxygen supply and demand. Angina pectoris is a warning sign for acute MI. Women and older adults may not always experience symptoms typically associated with angina or MI. The majority of deaths from an MI occur within 1 hr of symptom onset. Early recognition and treatment of acute MI is essential to prevent death. Research shows improved outcomes following an MI in clients treated with aspirin, beta-blockers, and angiotensinconverting enzyme (ACE) inhibitors.
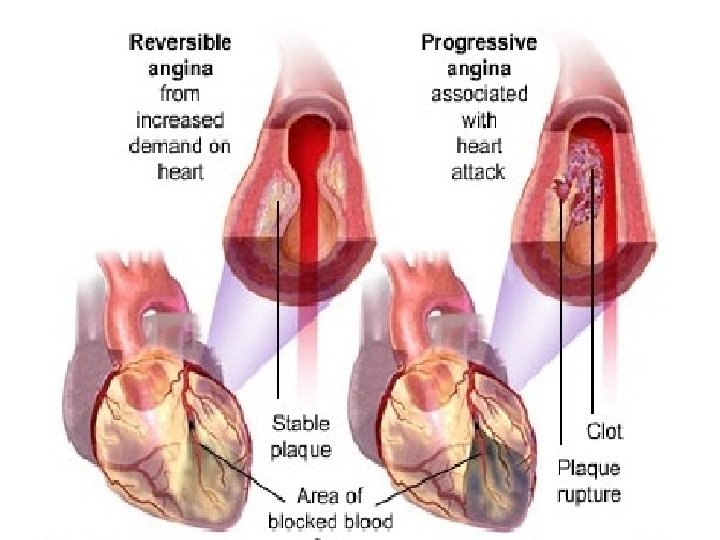
Key Points When blood flow to the heart is compromised, ischemia causes chest pain. Anginal pain is often described as a tight squeezing, heavy pressure, or constricting feeling in the chest. The pain may radiate to the jaw, neck, or arm. The three types of angina are: � Stable angina (exertional angina) occurs with exercise or emotional stress and is relieved by rest or nitroglycerin. � Unstable angina (preinfarction angina) occurs with exercise or emotional stress, but it increases in occurrence, severity, and duration over time. � Variant angina (Prinzmetal’s angina) is due to coronary artery spasm, often occurring at rest.
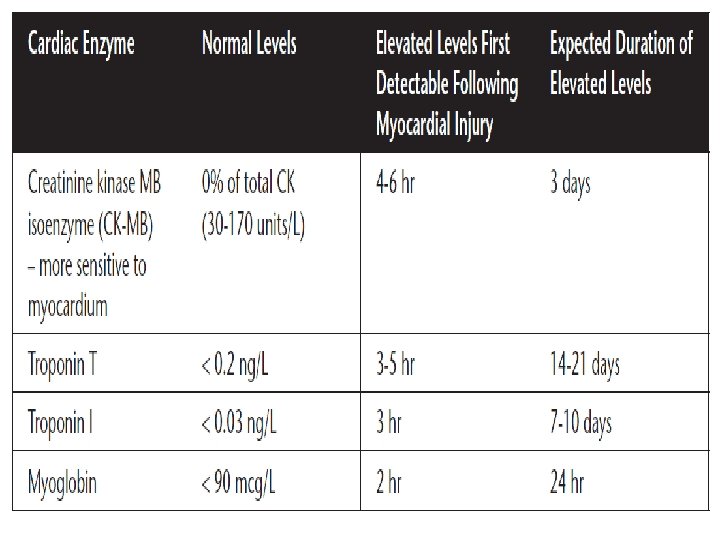
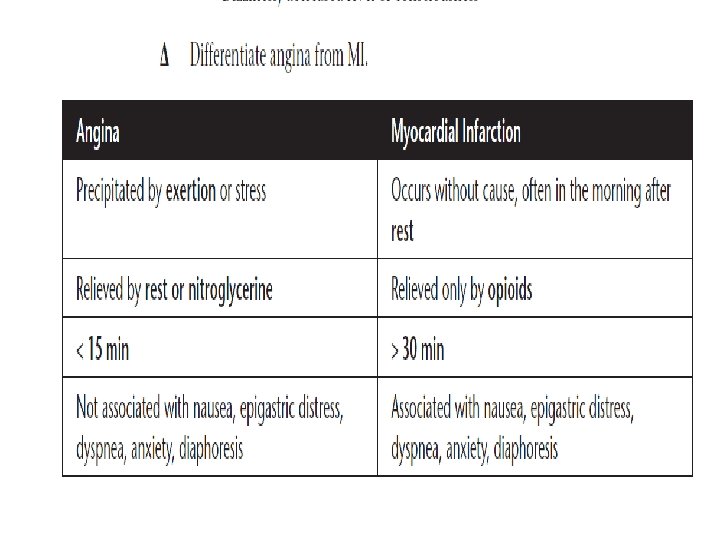
Key Points Pain unrelieved by rest or nitroglycerine and lasting for more than 15 min differentiates MI from angina. An abrupt interruption of oxygen to the heart muscle produces myocardial ischemia. Ischemia may lead to tissue necrosis (infarction) if blood supply and oxygen are not restored. Ischemia is reversible; infarction results in permanent damage. When the cardiac muscle suffers ischemic injury, cardiac enzymes are released into the bloodstream, providing specific markers of MI.
Key Points MIs are classified based on: � The affected area of the heart (anterior, anterolateral). � The depth of involvement (transmural versus nontransmural). � The EKG changes produced (Q wave, non-Q wave). Non-Q-wave MIs are more common in older adults, women, and clients with diabetes. � Now: Instead, acute coronary syndromes are classified as unstable angina, non-ST elevation MI and ST elevation MI.
Risk Factors for Angina and MI Male gender Hypertension Smoking history Increased age Hyperlipidemia Metabolic disorders: Diabetes mellitus, hyperthyroidism Methamphetamine or cocaine use Stress: Occupational, physical exercise, sexual activity Obesity Lack of exercise Hx of cardiac disease
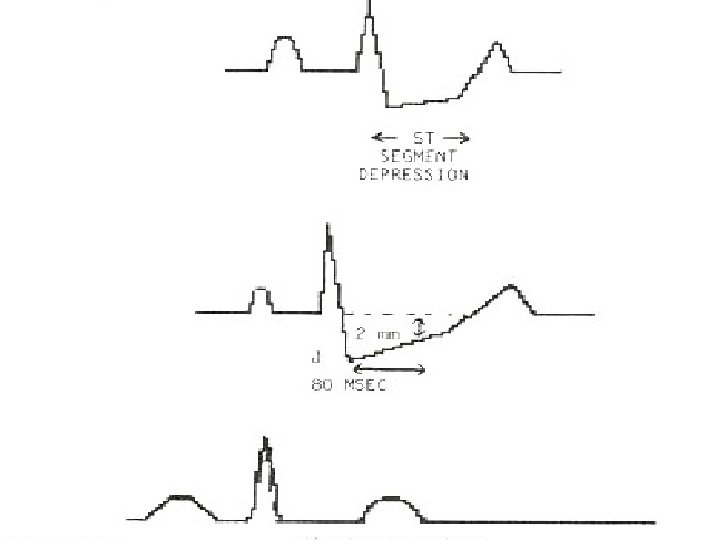
Diagnostic Procedures and Nursing Interventions ECG: Check for changes on serial ECGs. Angina: ST depression and/or T-wave inversion (ischemia) � MI: T-wave inversion (ischemia), ST-segment elevation (injury), and an abnormal Q wave (necrosis) � Clients with non-ST elevation MIs have other indicators. ST segment depression that resolves with relief of chest pain � New development of left bundle branch block � T-wave inversion in all chest leads � Serial Cardiac Enzymes: Typical pattern of elevation and decrease back to baseline occurs with MI. Cardiac catheterization reveals the exact location of coronary artery obstructions and the degree of ischemia and necrosis.
12
Therapeutic Procedures and Nursing Interventions Percutaneous transluminal coronary angioplasty (PTCA) uses a balloon at the tip of a catheter guided under fluoroscopy to press plaque against the vessel wall and to dilates the obstructed coronary artery to increase/restore tissue perfusion. Stents may be placed to maintain patency. Following a PTCA, monitor for bleeding (heparin), acute vessel closure (emergency coronary artery bypass graft), and dysrhythmias (reperfusion). Coronary artery bypass graft (CABG) surgery restores myocardial tissue perfusion by the addition of grafts bypassing the obstructed coronary arteries.
Assessment Angina is usually a result of atherosclerotic heart disease and is associated with a significant obstruction of a major coronary artery. Factors affecting anginal pain are physical exertion, exposure to cold, eating a heavy meal, or stress or any emotion- provoking situation that increases blood pressure, heart rate, and myocardial workload.
Assess/Monitor Vital signs every 15 min until stable, then every hour Serial ECG, continuous ST segment monitoring Location, severity, quality, and duration of pain Continuously monitor cardiac rhythm Oxygen saturation levels Hourly urine output – greater than 30 m. L/ hr indicates renal perfusion Laboratory data: Cardiac enzymes, electrolytes, ABGs
NANDA Nursing Diagnoses Ineffective cardiac tissue perfusion secondary to CAD as evidenced by chest pain or other prodromal symptoms Death anxiety Decreased cardiac output Acute pain Anxiety/fear Activity intolerance Deficient knowledge about underlying disease and methods for avoiding complications Noncompliance, ineffective management of therapeutic regimen related to failure to accept necessary lifestyle changes
Nursing Interventions The objective is to decrease O 2 demand of myocardium and to increase O 2 supply Administer oxygen (4 to 6 L), as prescribed. Obtain and maintain IV access. Promote energy conservation Administer medications as prescribed. � Vasodilators; Nitroglycerin is the medication of choice. � Analgesics reduce pain (Morphine is the medication of choice). � Beta-blockers (propranolol )have antidysrhythmic and antihypertensive � Thrombolytic agents can be effective in dissolving thrombi if administered the first 6 hr following an MI. � Antiplatelet; Aspirin is the medication of choice. � Anticoagulants � Glycoprotein IIB/IIIA inhibitors (thrombolytic agents) prevent the binding of fibrogen and thus block platelet aggregation.
Teach the client to avoid straining, strenuous exercise, or emotional stress when possible. Client education regarding response to chest pain: Stop activity and rest. Place nitroglycerin tablet under tongue to dissolve (quick absorption). Repeat every 5 min if the pain is not relieved. Call 101 if the pain is not relieved in 15 min. Prepare the client for diagnostic examinations as prescribed and revascularization procedures (angiography, angioplasty, CABG). Encourage lifestyle modifications to lower incidence of recurrence: smoking cessation, limiting saturated fat/cholesterol, weight management, and blood pressure control. Make appropriate referrals (for example, dietician).
Complications and Nursing Implications Acute MI is a complication of angina not relieved by rest or nitroglycerin. Cardiogenic shock is a serious complication of pump failure, commonly following an MI of 40% or more of the left ventricle. It is Class IV heart failure (tachycardia, hypotension , inadequate urinary output (less than 30 m. L/hr), altered level of consciousness, respiratory distress (crackles, tachypnea), cool, clammy skin, decreased peripheral pulses, and chest pain. Intervention: O 2, ET, morphine IV and/or nitroglycerin , vasopressors IV and/or positive inotropes Other possible emergency interventions include use of an intraaortic balloon pump and/or emergency CABG Ischemic mitral regurgitation due to myocardial ischemia may be evidenced by the development of new cardiac murmur. Dysrhythmias due to myocardial hypoperfusion require vigilant continuous cardiac monitoring. Ventricular aneurysms/rupture due to myocardial necrosis may present as sudden chest pain, dysrhythmias, and severe hypotension.
Prevention 23 Self care action plan changing habits. Ø Ø Stop smoking Increase level of exercise Cut down on fatty foods Eat more oats, which decrease cholesterol
24 Ø Lose wt if u DR. thinks you are overweight. Ø Make sure your BP is not high by regular check Ø Consider another method of contraceptive if you take pill
26
VALVULAR HEART DISEASE
Key points Valvular heart disease may have congenital or acquired causes. Valves on the left side are most commonly affected due to higher pressures. Valvular disease is classified as: � � Stenosis – narrowed opening that impedes blood moving forward. Insufficiency – improper closure – some blood flows backward (regurgitation). Congenital valvular disease may affect all four valves and cause either stenosis or insufficiency. Acquired valvular disease is classified as one of three types: � � � Degenerative disease – due to damage over time from mechanical stress; mostly results from hypertension. Rheumatic disease – gradual fibrotic changes, calcification of valve cusps. The mitral valve is most commonly affected. Infective endocarditis – infectious organisms destroy the valve. Streptococcal infections are a common cause.
Risk Factors for Valvular Heart Disease Hypertension Rheumatic fever (mitral stenosis and insufficiency) Infective endocarditis Congenital malformations Marfan syndrome
Diagnostic Procedures and Nursing Interventions Chest x-ray (chamber enlargement, pulmonary congestion, and valve calcification). 12 -lead electrocardiogram (ECG) shows chamber hypertrophy. Echoco (US) show s chamber size, hypertrophy, specific valve dysfunction, ejection function, and amount of regurgitant flow. Exercise tolerance testing (stress echo); impact of the valve problem on functioning during stress. Angiography reveals chamber pressures, ejection fraction, regurgitation, and pressure gradients
Therapeutic Procedures and Nursing Interventions Percutaneous balloon valvuloplasty may open the stenotic aortic or mitral valves. A catheter is inserted through the femoral artery and advanced to the heart. A balloon is inflated at the stenotic lesion to open the fused commissures and improve leaflet mobility. Surgical management includes valve repair, chordae tendineae reconstruction and prosthetic valve replacement. Prosthetic valves may be mechanical or tissue. Mechanical valves last longer but require anticoagulation. Tissue valves last 10 to 15 years.
Assessments Monitor for signs and symptoms. Left-sided valve damage results in dyspnea, fatigue, increased pulmonary artery pressure, and decreased cardiac output. Right-sided valve damage results in dyspnea, fatigue, increased right atrial pressure, peripheral edema, jugular vein distention, and hepatomegaly
Mitral stenosis Mitral insufficiency Aortic stenosis Aortic insufficiency Palpitations Proximal nocturnal Dyspnea Angina Hemoptysis Orthopnea Angina S 3 Hoarseness Palpitations Syncope Diastolic murmur Dysphagia S 3 and/or S 4 Decreased SVR Widened pulse pressure Jugular vein distention Crackles in lungs S 3 and/or S 4 Orthopnea Systolic murmur Cough Atrial fibrillation Narrowed pulse pressure Diastolic murmur Atrial fibrillation
Tricuspid stenosis Tricuspid insufficiency Atrial dysrhythmias Conduction delays Diastolic murmur Supraventricul ar tachycardia Decreased cardiac output Systolic murmur Pulmonic stenosis Cyanosis Systolic murmur Pulmonic insufficiency Diastolic murmur
Assess/Monitor Oxygen status Vital signs Cardiac rhythm Hemodynamics Heart and lung sounds Exercise tolerance
NANDA Nursing Diagnoses Decreased cardiac output Impaired gas exchange Activity intolerance Acute pain
Nursing Interventions Administer O 2 as prescribed to improve myocardial oxygenation. Maintain fluid and sodium restriction. Administer medications as prescribed. � Diuretics to decrease preload. � Antihypertensive agents (beta-blockers, calcium-channel blockers, ACE � Inotropic agents to increase contractility – digoxin (Lanoxin), dobutamine. � Anticoagulation therapy for clients with mechanical valve replacement Assist the client to conserve energy and decrease myocardial oxygen consumption. Post-surgery care is similar to coronary artery bypass surgery (care for sternal incision, activity limits for 6 weeks, report fever).
Nursing Interventions Client Education � Prophylactic antibiotics are recommended prior to dental work, surgery, or other invasive procedures. � Encourage the client to follow the prescribed exercise program. � Encourage adherence to dietary restrictions; consider nutritional consultation. � Teach the client energy conservation.
Complications and Nursing Implications Heart failure is the inability of the heart to maintain adequate circulation to meet tissue needs for oxygen and nutrients. Ineffective valves result in heart failure. Monitoring a client’s heart failure class (I to IV) is often the gauge for surgical intervention for valvular problems.