IHD By Shankar Angina pectoris Angina pectoris is

IHD By Shankar

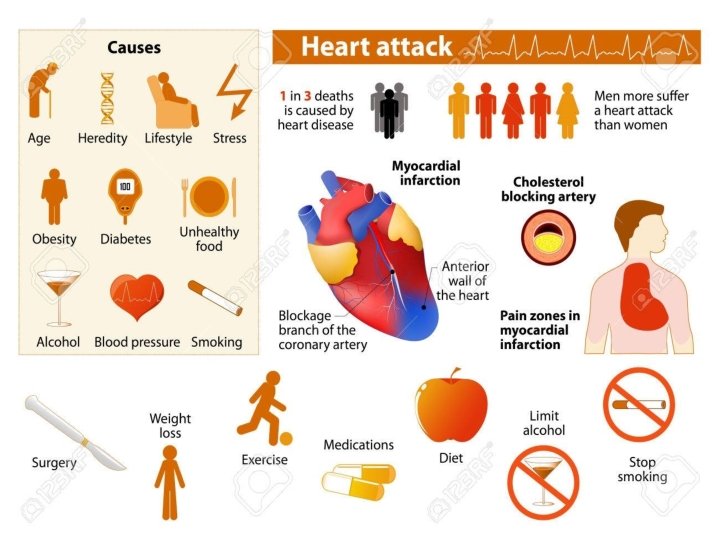
Angina pectoris • Angina pectoris is a clinical syndrome usually characterized by episodes or paroxysms of pain or pressure in the anterior chest. • The cause is usually insufficient coronary blood flow.

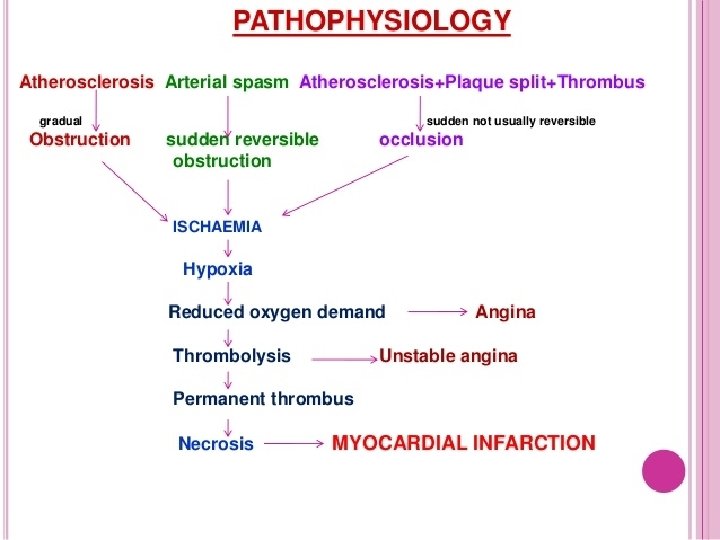
Mechanism

TYPES OF ANGINA • Stable angina: predictable and consistent pain that occurs on exertion and is relieved by rest. • Unstable angina (also called pre infarction angina or crescendo angina): symptoms occur more frequently and last longer than stable angina. The threshold for pain is lower, and pain may occur at rest.

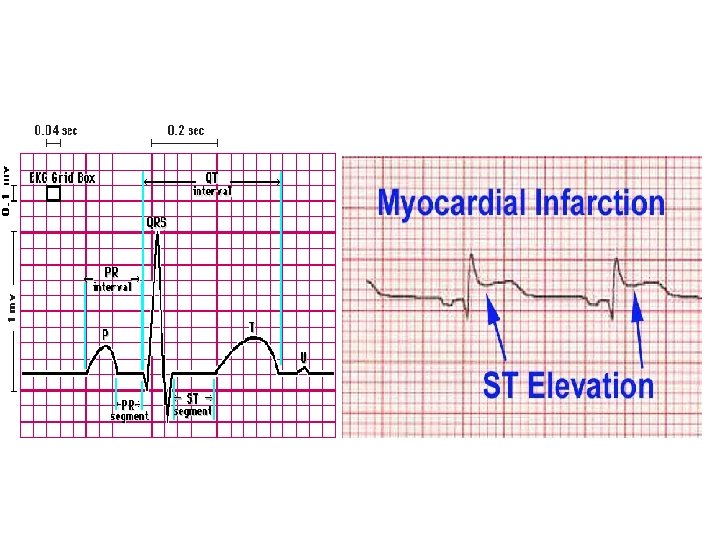
• Intractable or refractory angina: severe incapacitating chest pain. • Variant angina (also called Prinzmetal’s angina): pain at rest with reversible STsegment elevation; thought to be caused by coronary artery vasospasm

• Silent ischemia: ischemia (such objective as evidence of electrocardiographic changes with a stress test), but patient reports no symptoms • Decubitus angina : Occurs on lying down • Nocturnal angina : Occurs at night and may waken the patient from sleep


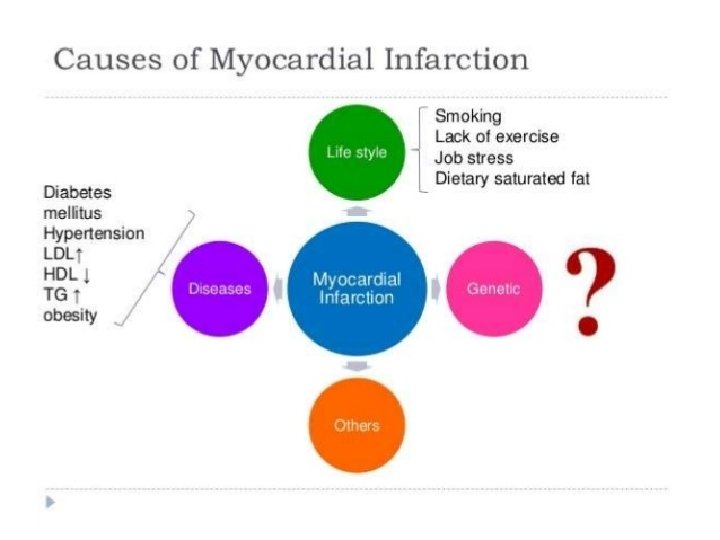
MI • Myocardial infarction refers to the dynamic process in which one or more regions of the heart experience a severe prolonged decrease in oxygen supply because of insufficient coronary blood flow, subsequently necrosis or death to myocardial tissue.
- Transmural infarcts extend through the whole thickness of the heart")
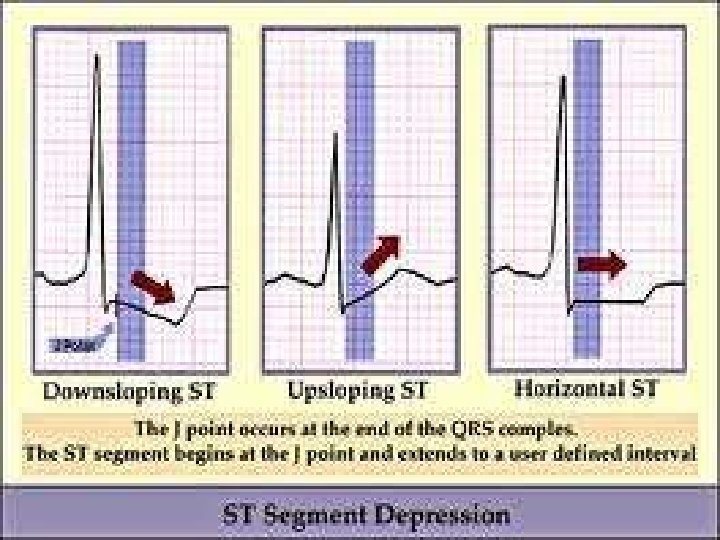
Types • STEMI (transmural)- Transmural infarcts extend through the whole thickness of the heart muscle and are usually a result of complete occlusion of the area's blood supply. In addition, on ECG, ST elevation and Q waves are seen. • NSTEMI(subendocardial) - involving a small area in the subendocardial wall of the left ventricle, ventricular septum, or papillary muscles. The subendocardial area is particularly susceptible to ischemia]. In addition, ST depression is seen on ECG.
 Type 1 (primary coronary event) Type 2 (secondary")
Types Type 3 (ST elevation ) Type 1 (primary coronary event) Type 2 (secondary ischemia) Type 4 (assosiated with coronary angioplasty) Type 5 (associated with CABG)

Degrees of MI • ZONE OF ISHCHEMIA: Region of heart muscle surrounding the injury which is ischemic and viable not endaged until extension of infarction occurs(abnormal Q wave) • ZONE OF INJURY: Region of muscle surrounding the area of necrosis, inflammed and injured but still visible if adequate oxygenation can be restored • Zone of Necrosis: Death of heart muscle caused by extensive and complete oxygen deprivation, irreversible damage

S/S of

Diagnostic evaluation History collection & Physical examination Cardiac enzymes Electrocardiograms & Echocardiograms Stress Tests Nuclear Imaging & Angiography

Stress test
 • Beta adrenergic blockers(ATENOLOL)")
Pharmacological therapy ANTI ANGINAL MEDICATIONS like • Nitrates(nitroglycerine, slidenafil, tadalafil) • Beta adrenergic blockers(ATENOLOL) • Calcium channel blockers(NEFIDIPINE) • Ace inhibitors(CAPTOPRIL) • Statins: it also known as HMG-Co. A inhibitors(atorvastatin, fluvastatin Etc) • Imipramine for analgesia

MI Medications given to treat a heart attack include: • Aspirin: Aspirin reduces blood clotting, thus helping maintain blood flow through a narrowed artery. • Thrombolytics: These drugs, also called clotbusters, help dissolve a blood clot that's blocking blood flow to your heart. • Superaspirins: These include medications, such as clopidogrel (Plavix) aggregation inhibitors. and others, called platelet
 • PCTA")
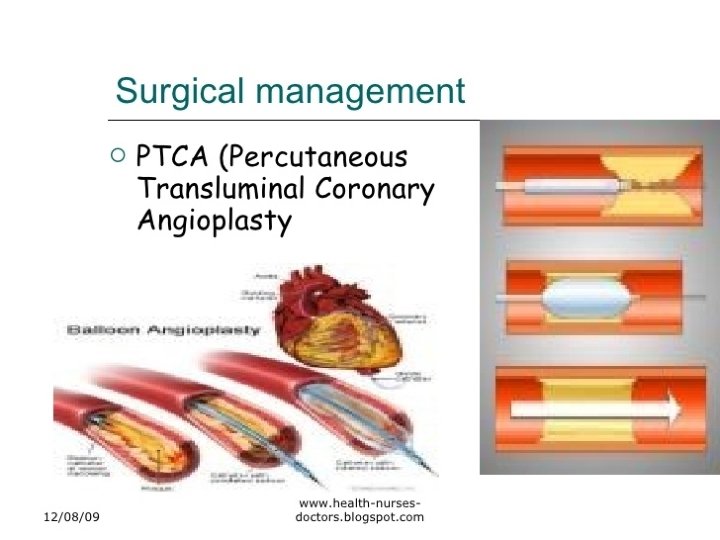
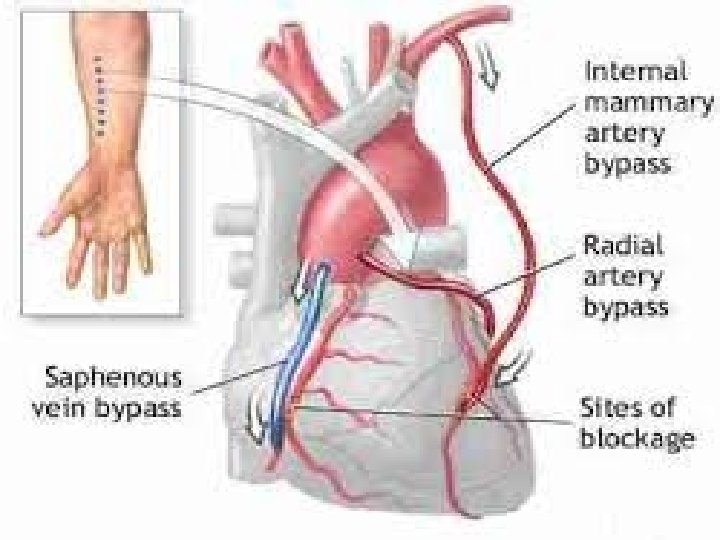
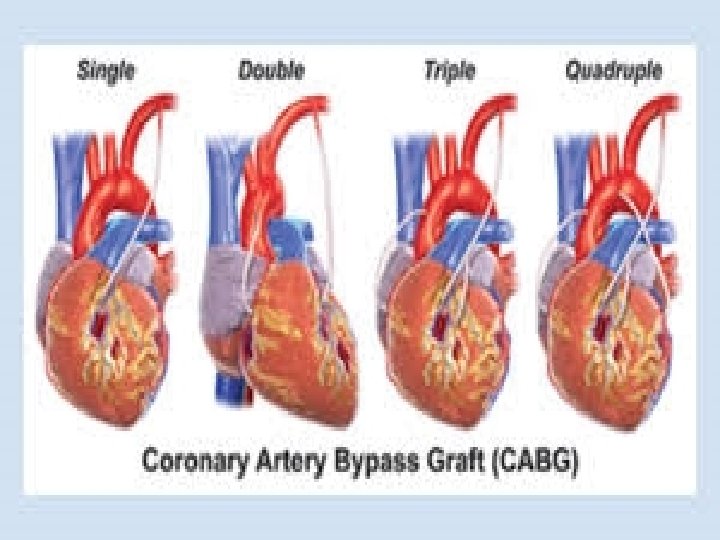
Surgical intervention • ANGIOPLASTY • STENTS • CORONARY ARTERY BYPASS GRAFTING(CABG) • PCTA

Life style modification Lifestyle changes that may be useful in coronary disease include: • Weight control • Smoking cessation • Exercise • Healthy diet

Stents

CABG

Cardiopulmonary bypass

Difference
- Slides: 32