Anesthesia Considerations in Thoracic Trauma Patients 2009 11











")
 •")
































- Slides: 48
Anesthesia Considerations in Thoracic Trauma Patients 張婉玲 醫師 嘉義長庚醫院 麻醉科 2009. 11. 21.
Introduction • Mortality from chest injuries is around 10% • The majority of patients with thoracic trauma can be managed conservatively • Require thoracotomy: ® Blunt trauma: 10 % ® Penetrating trauma: 15 %~ 30 %
Initial Management Plan • Airway maintenance with cervical spine protection • Breathing: ventilation and oxygenation • Circulation with hemorrhage control
Initial Assessment Ø Primary Survey: –AIRWAY • Always assume a cervical spine injury exists until proven • Jaw-thrust maneuver
Initial Assessment • ALWAYS ASSUME FULL STOMACH PRECAUTIONS---RAPID SEQUENCE INTUBATION
• Indications for intubation: –Airway obstruction –Pa. O 2 < 80 mm. Hg or Sp. O 2 < 90% with O 2 –Shock with SBP < 90 mm. Hg –Severe head injury or unconscious (GCS <9) –Anticipated surgery with multisystem injury
Initial Assessment • Awake intubation: local, topical superior laryngeal nerve blocks • Awake fiberoptic: may be too bloody • Awake cricothyrotomy/tracheostomy • Know your difficult airway algorithm!
Initial Assessment • BREATHING – 100 % O 2 –Always verify correct position of ETT.
Initial Assessment • Circulation –Control hemorrhage first! –Crystalloids vs. colloids vs. blood products?
Secondary survey • After primary survey complete, attempt to complete a head-to-toe assessment
Preop assessment • Cardiac: S/S shock, EKG changes • Respiratory: Breath sounds, crepitus, respiratory patterns/distress, CXR • Neurologic: GCS, LOC; assume C-spine injury until ruled out Lateral C-spine Xray, palpate neck • Renal: monitor urine output, amount and color
Preop assessment • Gastrointestional: FULL STOMACH!!!! • Endocrine: release of stress hormones (catecholaminesand glucose) • Hematologic: hypovolemicshock; coagulopathies
Laboratory/diagnostic tests • CBC, electrolytes, urinalysis, PT/PTT, lactate, baseline ABG (as condition permits) • CXR, lateral C-spine, CT/MRI • 12 lead EKG • FAST: focused abdominal sonography for trauma
INJURIES TO IDENTIFY DURING PRE-OPERATIVE ASSESSMENT
AIRWAY INJURY/OBSTRUCTION • Intrathoracic tracheobronchial injuries are less common than upper airway injuries. • High mortality. • A definitive airway can usually be secured using a fiber-optic bronchoscope
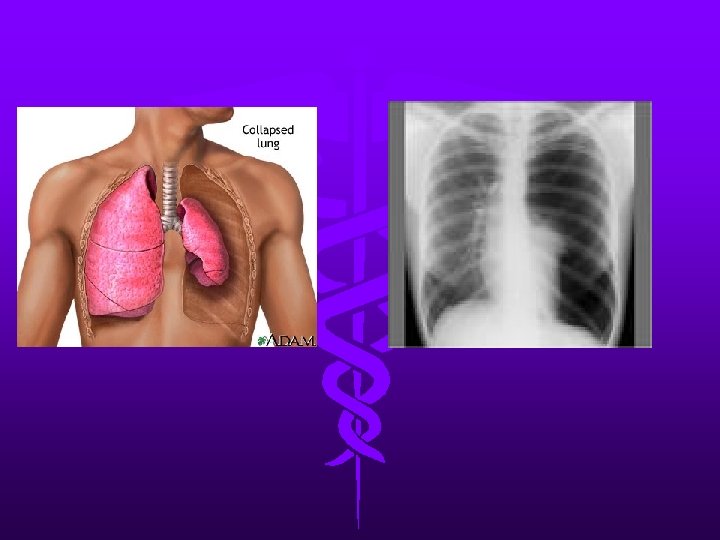
Pneumothorax • Accumulation of air between parietal and visceral pleura • Results in severe V/Q mismatch and hypoxia • S/S: –chest wall hyperresonant to percussion –Breath sounds decreased or absent unilaterally –Subcutaneous emphysema –CXR confirms
Tension pneumothorax • Diagnosis of tension pneumothorax is clinical rather than radiological - Absent breath sounds - Hyper-resonant percussion - No chest movement - Tracheal deviation to the injured side - Distended neck veins (may not be seen if the patient is hypovolaemic). - Severe dyspnoea, tachycardia and hypotension
Tension pneumothorax • Immediate chest decompression is required. • During anaesthesia ü In pressure controlled modes: ↓ tidal volume ü In volume controlled modes: ↑ peak airway pressure
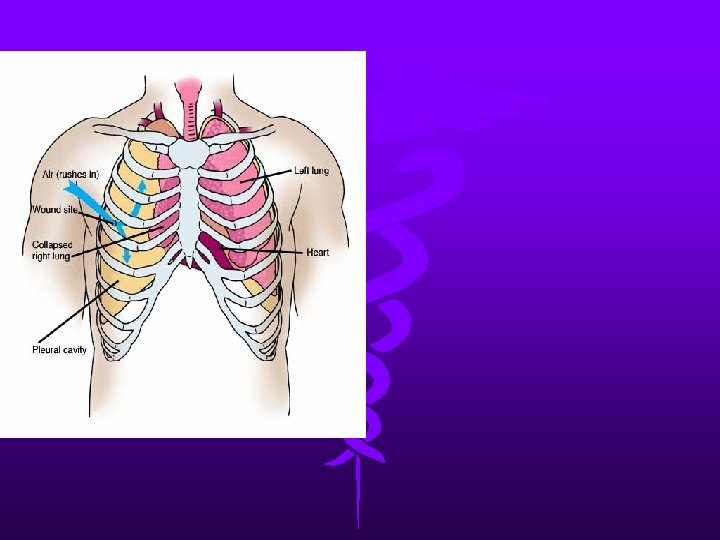
OPEN PNEUMOTHORAX • >2/3 rd the diameter of the trachea. • This results in paradoxical breathing with collapse of the lung on the affected side during inspiration. • This results in increased intra-pulmonary shunt, decreased venous return and progressive hypoxaemia and hypercapnia. • Administration of oxygen, covering the wound and chest drain insertion.
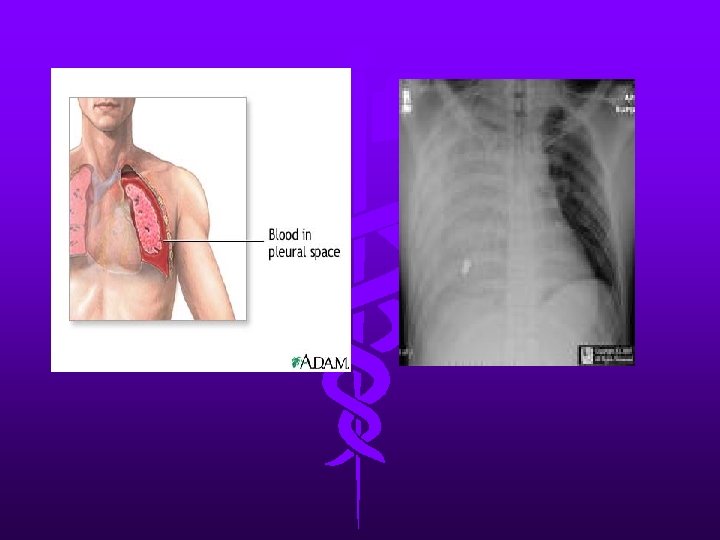
Hemothorax • Can be caused from bleeding of intercostal vessels, pulmonary arteries or veins, avulsion of mediastinal vessels or penetrating cardiac injury. • Differentiated from pneumothorax by dullness to percussion with absent breath sounds
Hemothorax • The choice and dose of anaesthetic induction agent is determined by the severity of the shock and any preexisting medical co-morbidity • Fluid load before chest tube placement • Thoracotomy may be needed if drainage is more than 250 mls per hour, or the patient’s physiological status continues to deteriorate despite fluid replacement.
Flail chest • Results from two or more ribs fracture in two or more places • Accompanied by hemothorax or pulmonary contusion • Patients with 3 or more rib fractures have greater likelihood of hepatic or splenicinjury
Flail chest • S/S –Paradoxical chest wall movement • Treatment –O 2 –Pain control
Cardiac tamponade • Life-threatening emergency • Bleeding into pericardial space, which restricts cardiac filling during diastole and creates a low cardiac output state • Initial symptoms - Dyspnea – Orthopnea – tachycardia
Cardiac tamponade • Classic symptoms –Beck’s triad neck vein distention, hypotension, muffled heart sounds –Pulsus paradoxus: > 10 mm. Hg decrease in blood pressure during spontaneous inspiration • May not be evident in hypovolemia
Cardiac tamponade • Echocardiography provides the definitive diagnosis.
ANAESTHESIA FOR RESUSCITATIVE THORACOTOMY • Penetrating cardiac injury may rapidly lead to cardiac arrest. • Induction of anaesthesia may lead to a dramatic loss of blood pressure and care should be taken with the choice of induction agent.
AORTIC DISRUPTION • A wide mediastinum on chest X-ray may be the only indication that the injury has occurred • Spiral contrast CT is now performed more frequently than angiography
TRACHEOBRONCHIAL INJURY • high mortality • In blunt trauma the majority of injuries occur within a 2 – 3 cm of the carina • Signs include haemoptysis, subcutaneous emphysema and persisting pneumothorax or broncho-pleural fistula following chest drain insertion.
TRACHEOBRONCHIAL INJURY • Low tidal volume, permissive hypercapnia ventilatory strategies are required until surgical intervention has occurred. • Once intubated fibre optic bronchoscopy is needed to identify the site of the leak.
OESOPHAGEAL DISRUPTION • very rare • most frequently occurring in the lower oesophagus
DIAPHRAGMATIC RUPTURE • most commonly after blunt abdominal trauma. • Usually on the left side. • Classically the stomach, nasogastric tube or colon is noted to be in the left side of the chest on chest X-ray.
Pulmonary contusion • Intra-alveolar hemorrhage and edema resulting from sudden increase in intraalveolar pressure and rupture of alveolar-capillary interface • Difficult to diagnosis
ARDS • Later pulmonary complication • Attributed to direct thoracic injury, sepsis, aspiration, head injury, massive transfusion, oxygen toxicity, and fat embolism • Mortality rate reaching 50%
INTRA-OPERATIVE LUNG PROTECTIVE STRATEGIES • LUNG PROTECTIVE VENTILATION ü tidal volume 6 - 8 mls/kg ü trans alveolar pressure is kept below 35 cm of water (plateau airway pressure of 35 - 45 cm of water).
INTRA-OPERATIVE LUNG PROTECTIVE STRATEGIES • INTRA-OPERATIVE LUNG RECRUITMENT ü Extrinsic PEEP ü a single large tidal breath and holding end inspiration for 20 seconds
Myocardial contusion • Associated with blunt trauma • Contusion most often right ventricle since lies directly posterior to sternum • S/S –Dysrhythmias: heart block to Vfib; ST segment elevation –Elevated CPK-MB; ? Troponin elevation –CHF –Anginal pain which may or may not respond to nitrates
Anesthetic management • The general principles of trauma anesthesia such as oxygenation, restoration of circulating volume, correction of hypothermia and coagulopathy.
Anesthetic management Ø Induction • Standard monitors • Preoxygenation • direct laryngoscopy + RSI • Invasive monitors as indicated
Induction agents • Thiopental 3 -4 mg/kg; reduce doses in unstable patients • Ketamine 0. 5 -1 mg/kg; useful for burn and hypovolemic patients; avoid with head injuried • Etomidate 0. 1 -0. 3 mg/kg; reduce doses with hypovolemia • Propofol 1 -2 mg/kg in stable patients; reduce doses in hypovolemia
Muscle relaxants • Succinylcholine: 1 -2 mg/kg; useful for RSI • Rocuronium: 1 mg/kg
ONE LUNG ANAESTHESIA • Double-lumen tubes are often difficult to insert during rapid sequence intubation and are commonlyassociated with malposition.
Maintenance • Low-dose volatile agent with fentanyl and nondepolarizing muscle relaxant is usually suitable. • Avoid Nitrous oxide. • Bispectral index monitor
Conclusion • Blunt or penetrating thoracic injuries present a particular challenge as a result of complex, dynamic and lifethreatening injuries • The roles of the anesthesiologist and anesthetist are critical.