LOW FLOW ANESTHESIA LOW FLOW ANESTHESIA LOW FLOW




 In the mid 50’s, when HAL was brought forth, the")
 Introduction of ISO in the early 1980’s gave way to")
 has been variously defined as an inhalation")
… LFA: Anesthesia delivery, where FGF is below 1. 5 l/min,")




![Brody Formula for Oxygen Uptake VO 2 = 10 x KG [kg] 3/4 [m.](https://slidetodoc.com/presentation_image/00860d82f3728ce777394e0317e0a587/image-13.jpg "Brody Formula for Oxygen Uptake VO 2 = 10 x KG [kg] 3/4 [m.")

![UPTAKE OF NITROUS OXIDE VN 2 O = 1000 t-1/2 [m. L/min] Having 70%](https://slidetodoc.com/presentation_image/00860d82f3728ce777394e0317e0a587/image-15.jpg "UPTAKE OF NITROUS OXIDE VN 2 O = 1000 t-1/2 [m. L/min] Having 70%")


















, including O 2,")























































- Slides: 92
LOW FLOW ANESTHESIA LOW FLOW ANESTHESIA LOW FLOW ANESTHESIA Dr. Paul Zilberman Israel, 2010 paulzi 60@yahoo. com
…or the long way of the oxygen from its discovery till our patients…
JOSEPH PRIESTLEY 1733 -1804 On August 1, 1774, he produced the “dephlogisticated air”, known later as OXYGEN
A SHORT HISTORY Inhalational anesthesia and closed system anesthesia are almost the same age. Almost/closed anesthesia systems have been in use since 1850. At that time the anesthetic agent was cloroform, administrated via a closed system, where KOH was utilized as a CO 2 absorber. However, that kind of CO 2 absorption did not gain acceptance. Later, a quick and effective method of CO 2 absorption was developed when the first soda-lime absorber was introduced in 1917.
A SHORT HISTORY (con’t…) In the mid 50’s, when HAL was brought forth, the use of LFA and closed system anesthesia diminished significantly. This was largely due to the inherent problem of the first generation HAL vaporizers, which was the unreliable delivery of vapor at low FGF.
A SHORT HISTORY (con’t…) Introduction of ISO in the early 1980’s gave way to a renewed interest in LFA and closed circuit anesthesia. It was further enhanced by the fact that anesthetic agents are atmospheric pollutants, especially N 2 O, HAL, ENF, and to some extent ISO. The introduction of new low solubility agents, like DES and SEVO, have initiated a renaissance in the use of LFA, in order to contain costs associated with adapting FGF to patient demand.
A FEW DEFINITIONS… Low Flow Anesthesia (LFA) has been variously defined as an inhalation technique in which a circle system with absorbent is used with a fresh gas inflow of : - less than the patient’s alveolar minute volume - less than 1 -1. 5 l/min - 3 l/min or less - 0. 5 – 2 l/min - less than 4 l/min - 500 – 1000 ml/min - 0. 5 – 1 l/min Closed System Anesthesia is a form of LFA in which the FGF = uptake of anesthetic gases and oxygen by the patient and gas sampling. No gas is vented by the APL valve. Dorsch and Dorsch Understanding Anesthesia Equipment
A FEW DEFINITIONS (con’t)… LFA: Anesthesia delivery, where FGF is below 1. 5 l/min, but maintained slightly above the uptake of the patient. In addition, there is a low flow of excess gas that leaves the circuit through the excess gas valve. Closed Circle Anesthesia: Anesthesia whereby FGF matches patient gas uptake and there is no excess gas leaving the circuit by way of excess gas valve. Minimal Flow Anesthesia: Anesthesia whereby FGF is 0. 5 l/min. www. clinicalwindow. net Ola Stenqvist MD. Ph. D Anest. And Intensive Care Goteborg, Sweden, Sponsored by GE Health Care
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Professor Samuel Brody
The kind of laboratory used by Prof. Brody. It seems that excellent minds can extract a lot from apparently little.
Graph relating metabolism to body size “Bioenergetics and growth” 1945
Brody Formula for Oxygen Uptake VO 2 = 10 x KG [kg] 3/4 [m. L/min] Where BW is body weight in kilograms However, for clinical purposes, oxygen consumption can be more easily calculated as: VO 2 = 3. 5 x BW [ml/min]
John W. Severinghaus
UPTAKE OF NITROUS OXIDE VN 2 O = 1000 t-1/2 [m. L/min] Having 70% in N 2 O, with a BW of 70 kg. That gives a – 1 st minute uptake of 1000 m. L - 200 m. L/min uptake after 25 minutes - 140 m. L/min uptake after 50 minutes - 90 m. L/min uptake after 2 hours (120 minutes) Source: Severinghaus JW, The rate of uptake of nitrous oxide in man. J. Clin. Invest 1954
UPTAKE OF INHALATIONAL AGENTS Independent of the agent employed uptake can be calculated using Lowe’s formula: Van= f * MAC * λB/G * Q * t-1/2 [m. L/min] f = factor that defines the inhalation concentration that is sufficient for unresponsive skin incision at ~MAC 1. 3 λB/G = blood/gas partition coefficient Q = cardiac output t = time
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
THE REBREATHING SYSTEMS REBREATHING describes a technique in which nonconsumed gases, contained in the exhaled air are partially or completely re-routed back to the patient during the following inspiration, purified from CO 2 AND admixed with a certain amount of fresh gas.
THE REBREATHING SYSTEMS Semi-open: VF ≥ MV Semi-closed: MV > VF > Uptake Closed: VF = Uptake Where: VF = FGF MV = Minute Ventilation Uptake = Total gas uptake of the patient
THE “CATCH” Using a FGF of 5 LPM and a vaporizer setting of 1%, we give to the patient: 5000 m. L/min x 0. 01 = 50 m. L/min What would be the vaporizer setting if we would use a FGF of 1 LPM for the same 50 m. L to be delivered? 1000 m. L/min X ? = 50 m. L/min ? = ……
? = 0. 05 That means that the vaporizer should be opened to 5%! Sounds bizarre, isn’t it! It really does, because we are not used to it! And yet, mathematics is all what it is about! Under these circumstances the patient receives EXACTLY the same amount of gas, in fact the same amount of MEDICINE! This is called : BIOAVAILABILITY!
All over the world 5 X 1 =
=1 X 5
TECHNICAL ASPECTS In LFA there a few technical requirements. Typically they are rather generic and more or less independent of anesthesia machines used. 1. Circle rebreathing system with CO 2 absorption 2. Accurate flow meters for adjustments of FGF below 1 L/min 3. Gas tight breathing system. Recommended test leakage should be below 150 m. L/min at 30 cm H 2 O test pressure. 4. Ascending bellows, not rising up to the top of the bellows chamber may indicate breathing system leakage. The same is true for other alarms (LOW PRESSURE, spirometry loop).
5. The breathing system should have minimal internal volume and a minimum number of components and connections. 6. Continuous gas monitoring MUST be employed. From the clinical standpoint the measurement of expiratory gas concentrations close to the Y-piece is of crucial importance. That information is essential in controlling the patient’s alveolar gas concentrations, whereas Fi reflect the adequacy of gas concentrations into the breathing circuit. Hey! Does it sound very familiar with our usual anesthesia machine?
“Introduction to low flow anesthesia” ppt. 2004, author unreachable
ADVANTAGES OF THE LFA 1. QUALITY OF PATIENT CARE Anesthetic gases delivered using high FGF are usually dry and cold. Reducing FGF makes gases recirculating in the circle system more humid and warmer. With low FGF the gases repeatedly circulate through the CO 2 absorber. Consequently more heat and humidity is produced through the chemical CO 2 absorption process. Breathing warm and humid gases is beneficial for the patient because they help maintaining body heat, prevent postoperative shivering and airway and bronchial drying during ETT use.
Tracheal intubation bypasses the upper airways, thus, eliminating the main effect of the inhaled gases : warming and humidification. In the spontaneously breathing patient the isothermic saturation boundary of the inspiratory mixture (the point where the gases reach 370 C and 100% humidity) is located at the 4 -5 th generation of bronchi. After tracheal intubation, as a consequence of the upper airway bypass, this isothermic point is shifted down about 10 cm in a bronchial region not suited to deal with dry and cold gases and not suited to physiologically condition the respiratory mixture (do you think now about the LMA in a new way? ).
2. ECONOMIC BENEFITS Over 80% of anesthetic gases are wasted when flows of 5 L/min are used. Several studies also prove that the use of low and minimal flow anesthesia techniques can dramatically reduce the (annual) costs of volatile anesthetics. Typically the reduction of FGF from 3 L/min to 1 L/min results in savings of about 50% of the total consumption of any volatile agent. clinicalwindow. net
Total cost of anesthesia depend on complex interactions between anesthesia providers, patients, payers, techno- logy and facility. Money makes the world go round!? These costs comprise direct, indirect and intangible costs. Direct costs, the ones that can be influenced by the anesthesia provider represent 3 -5% of the total healthcare costs in the US. (1993). If we consider the PACU expenses related to the anesthesia process than the costs may go up to 10%. While it is difficult to measure exactly the volatile agent cost (m. L/hour, different producers, vapor/m. L liquid, delivery in excess of uptake) as opposed to IV drugs, a larger survey demonstrated that economies in volatile use going up to 90% can be achieved. Pharmacoeconomics 2000, June 17(6), 585 -590
Definitions of different types of costs Type of cost Definition Costs Irreversible use of a resource Direct costs Costs of the material and labor used for production osts that remain the same no matter many goods or services are produced Costs that change with the number of goods or services that are produced Costs related to the consequences of an event to society or an individual s Costs of pain and suffering as a result of illness or treatment
This is where unused gases ($, €, £, ¥, etc. ), including O 2, N 2 O go…
Copyright 1984 -2011, James H Philip, all rights reserved
3. ENVIRONMENTAL BENEFITS High flow anesthesia inevitably results in pollution of the environment. N 2 O, for example, is a significant “green house gas”, and is estimated to be responsible for about 10% of this effect. Hmmm, not so green after all… Reduced FGF releases a lower amount of anesthetic agents into the environment, resulting in less pollution. All gases delivered from the anesthesia machines are lost to the atmosphere. HAL, ENF, ISO contain chlorine. They are believed to have significant ozone (O 3) depleting potential. The stability of these molecules permits their passage to the stratosphere where increasing UV radiation causes dissocia- tion to liberate free chlorine, which acts as a catalyst in the break down of O 3. This reaction is the major cause of destruc tion of the O 3 layer, especially over the South Pole.
N 2 O is also a catalyst in an analogous reaction. While anesthetists thus have a clear duty to minimize the use (release) of these chemicals, it has to be admitted that our practice’s contribution to the global release is minimal. DES and SEV contain no chlorine and appear to have no greenhouse gas effects.
THE OTHER SIDE OF THE COIN Disadvantages of LFA: 1. Limitations of currently used vaporizers: Modern vaporizers are little different from those used in the ’ 60 s. They are designed for use with high FGF with a consequent requirement for high thermal capacity, temperature compensation and high accu- racy. The use of LFA makes these characteristics unnecessary but it also introduces the problem of delivering an adequate quantity of volatile agent into the breathing system.
2. Accumulation of unwanted gases into the breathing system: If you put little gas into the breathing system, little (or none) will come out. As a result of this failure to flush gases out of the system, any gases introduced which are not taken up by the patient or absorbed chemically will tend to accu mulate. Such gases may be exhaled by the patient, be a contami- nant of the medical gases or result from a reaction with the chemical agents used for CO 2 absorption.
Substances exhaled by the patient: - Alcohol - Acetone - CO - CH 4 Therefore the use of LFA is contraindicated in patients who are intoxicated, in uncompensated diabetic states or who are suffering from CO intoxication.
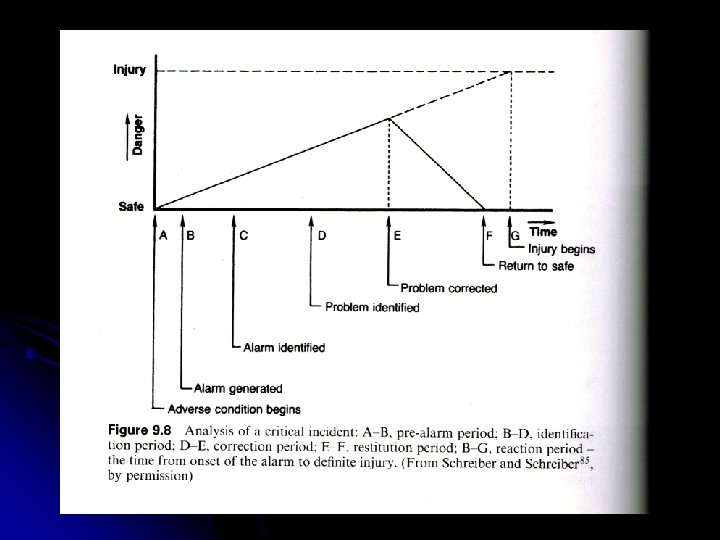
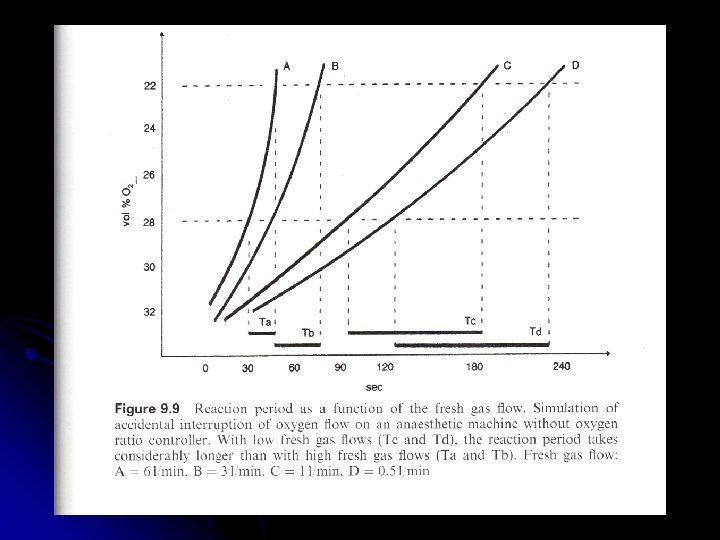
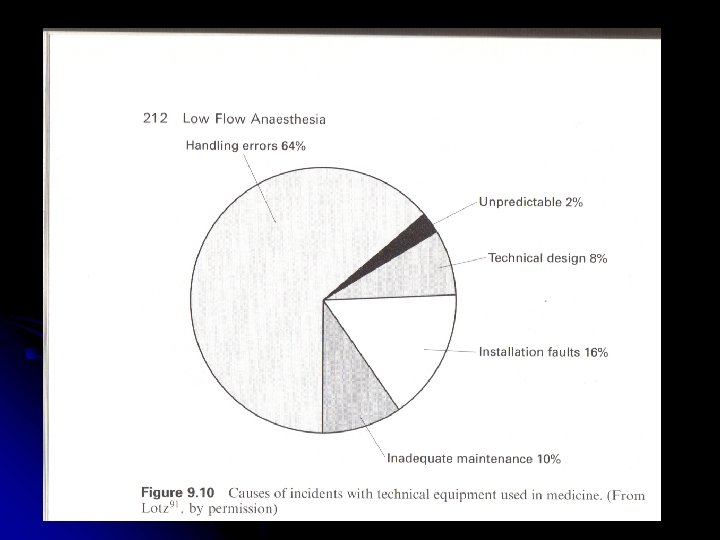
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Specific safety features of anesthetic techniques with reduced FGF 1. Improved equipment maintenance ong time constant: sometimes the “good is imbedded in the bad”! 3. Improved knowledge of theory and practice of inhalational anesthesia.
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
SO, HOW DO WE DO “IT”? PRACTICALLY!
HOW TO ADJUST FGF AT DIFFERENT PHASES OF LFA Premedication, pre-oxygenation and induction of sleep are performed according to the usual practice. Concerning adjustment of FGF anesthesia can be divided into 3 phases: 1. Initial HIGH flow 2. Low flow 3. Recovery
1. Initial HIGH flow phase At the beginning of anesthesia high FGF of 5 -6 LPM is necessary to wash out nitrogen (N 2) from the patients body tissues. High initial flow facilitates the filling of the breathing system with the desired gas composition which in turn influences patient uptake and distribution of the anesthetic agents. (Remember the formulas in the beginning? The patient takes , after all, what he/she needs, provided the provider is providing enough!)
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
2. Low flow phase After the high flow phase of 5 -15 min, or when the target gas concentrations has been achieved FGF can be reduced at the desired low flow level. The lower the FGF the greater the difference between the vaporizer setting and inspired concentration of the anesthetic agent in the breathing circuit will be. With low FGF, time to reach the desired concentration in the inspiratory gas will be prolonged. Hence, monitoring of oxygen and anesthetic agent concentration is essential and necessary in LFA.
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
If the flow provided is too small for the patient’s needs the bellow will gradually go down, down. . .
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Reproduced with permission from “Low Flow Anesthesia with Draeger machines” by Prof. J. A. Baum
Low Fresh Gas Flow Oxygen and Agent Considerations JAMES H. Philip MEE MD CCE Anaesthesiologist and Director of Bioengineering Department of Anaesthesiology, Perioperative and Pain Medicine Brigham and Woman’s Hospital Medical Liaison for Anesthesia Department of Anaesthesia Harvard Medical School Author of Gas. Man® and President of Med. Man Simulations Inc. , a charitable Organization distributing gas man http: //gasmanweb. com The following X slides have been added with the author’s permission
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
Copyright 1984 -2011, James H Philip, all rights reserved
3. Recovery phase At the end of anesthesia high FGF, usually 100% O 2, is necessary, to facilitate the washout of the anesthetic agent from the patient and to remove the agent to the scavenging system.
SOME COMMENTS… Today, LFA is such a safe and simple procedure that there are no reasons not to use it routinely. It can be even argued that the use of unnecessary FGF should be regarded as inappropriate. However, it is still possible to find anesthesia departments where LFA is not used in special situations (prone position, thoracic surgery) or simply not at all. The most common misconception about is that it cannot be used in spontaneous breathing patients or with those having an LMA. There is, however, no rationale for such a view. The LMA has been shown to be effective both in pediatric and adult LFA. www. clinicalwindow. net
The majority of anesthesiologists, during their clinical practice usually avoid working with FGF < 1 LPM due to their cultural and practical beliefs including: - requirement of in depth knowledge on gas laws and physics applied to clinical anesthesia (oof, learn again? ) - pharmacokinetic and pharmacodynamic features of haloge nated agents used until the mid 90’s - lack of accuracy, expense and limited performance of anes thesia machines utilized in anesthesia up to the end of the 90’s. In 1994, in the United States, 90% of anesthesiologists utilized 2 -5 l/min of FFG and only 12% of physicians used an FFG infe rior to 1 l/min.
The recent introduction on the market of low solubility halogena- ted agents and the technological development of high- performing anesthesia ventilators, supplied with feed-back control systems and high precision monitoring systems, make LFA/CSA safe and feasible on a daily basis. This occurrence represents a great advantage as far as clinical practice, cultural, environmental, pharmacological, technological and cost savings concerns.
As with any other anaesthetic technique, LFA has its relative and absolute contraindications, and anaesthetists have to know the risks and limitations of this method. The potential risks associated with low-flow anaesthesia are accidental hypoxia, hypercapnia, inadequate depth of anaesthesia and the accumulation of potentially toxic trace gases. A basic knowledge of the uptake and distribution of anaesthe- tic gases and appropriate patient monitoring such as pulse oxymetry, capnometry, inspired oxygen monitoring and anaesthetic gas analysis are required for safely delivering general anaesthesia with low fresh gas flows. The extent of patient monitoring, however, is similar to that for any other anaesthetic technique. Sounds familiar again?
Awareness during anesthesia “It can’t be! You should be sleeping!”
The end? Not quite…A few answers from… FINLAND, Dr. Riku Aantaa MD, DMed. Sci former President of the Finnish Society of Anesthesiologists “…I have the understanding (we even did a survey some 5 years ago) that low flow (FGF 0. 5 -1. 5 LPM) is standard care throughout my country”.
USA, Dr. Jerrold Lerman MD, Clinical Professor of Anesthesia Women and Children's Hospital of Buffalo, SUNY at Buffalo, and University of Rochester, New York “I use flows about 1 -1. 5 LPM”
NORWAY, Dr. Per Meinich President The Norwegian Society of Anaesthesiology “…has approximately 50 surgical hospitals, and with the exception of some small, private clinics, they all perform gas anesthesia. Each hospital decides on which machines they want to use, and each hospital has its own guidelines. To my knowledge, all hospital which utilize gas anesthesia do so in close loop, low flow systems”.
SOUTH KOREA, Dr. Hong Seuk Yang : MD, Department of Anesthesiology and Pain Medicine, Asan Medical Center, College of Medicine, University of Ulsan “Low flow anesthesia technique is more popular in Korea from 5 years ago, after the introduction of SEVO and DES. Flow rate is maintained at 2 LPM (O 2: N 2 O 1: 1). Usually we don’t decrease the flow rate below 2 LPM”
CANADA, Dr. Glenn Mc. Guire Department of Anesthesia Toronto Western Hospital “The circuit is checked at the beginning of the day for leaks (leak must be under 180 m. L/min). I use DES with N 2 O and O 2 at a total flow of 1 LPM for both mechanical ventilation and spontaneous breathing. Years ago anesthetists used to turn up the flows for spontaneous breathing. This is an outdated concept and is no longer practical. Of course, with spontaneous breathing I always use CPAP”
UNITED KINGDOM, Dr. Andrew Mc. Hutchon MB Ch. B FRCA, Anesthesia & Intensive Care. Northumbria Healthcare , UK. In my hospital we have a very strict approach to gas economy. The reason for no recent publications is that virtually all the information we need is already known. Anyone who uses high flows is wasting money and polluting the environment without any benefit to patients. If we need more information we should ask the question: " what happens to inhalational agents in the upper atmosphere? ” A similar question for TIVA, “what substances do the manufacturers of Propofol and Remifentanil release into the environment? ” If the anesthetist understands the kinetics of his system, the patient gets a good anesthetic with enough agent.
ITALY, Dr. Amato del Monte: Dr. Amato De Monte Director of Anaesthesia & I. C. U. Department Azienda Ospedaliero Universitaria S. M. Misericordia – Udine “The breaking method to introduce closed system anesthesia in my hospital was the implementation of our anesthesia machines with the ZEUS…This fact obliged my colleagues to face the topic. I can’t give [you] an answer of the penetration [of LFA] in Italy. Anyway, the majority of a small group, 400 anesthesiologists, interviewed with the simple question considered low flow a FGF of 3 LPM”.
If you want to be Like the guy in the figure All the time he trigger… It’s up to you
Or enjoy a cozy sleep While the machine does gently “beep”…
In a simple way, we can say… The LFA is the mathematical art of volatile anesthesia…
Questions anyone?