BIOLOGICAL CONSIDERATIONS IN MANDIBULAR IMPRESSION CHRISTEENA JOSEPH FIRST

BIOLOGICAL CONSIDERATIONS IN MANDIBULAR IMPRESSION. CHRISTEENA JOSEPH FIRST YR PG Dept. of prosthodontics

CONTENTS �Introduction Definition �Supporting structures � 1. Bone � 2. Mucous membrane �

� Anatomy of limiting structures in mandibular region � Anatomy of supporting structures in mandibular region � Anatomy of relief structures in mandibular region � Muscle attachments � summary � Conclusion � Reference �

INTRODUCTION The fundamental principles involved in the support of mandibular and maxillary dentures are the same. � The denture bases must be extented to cover the maximum area possible without interfering with the health or function of the tissues , whose support is from bone. �

The prosthodontist must have a complete understanding of macroscopic and microscopic anatomy of edentulous mouth of patient. �

ANATOMICAL LANDMARK “ a recognizable anatomic structure used as a point of reference. ” GPT-8 In both maxilla and mandible anatomic landmarks has been divided in-supporting structures -peripheral or limiting structure Principle and technique of complete denture Iwao hayakawa

SUPPORTING STRUCTURES “Those areas of maxillary and mandibular edentulous ridges that are considered best suited to carry the forces of mastication when dentures are in function. ” (GPT-8)

Maxillary and mandibular dentures transfer occlusal loads to these so called supporting structures. � The ultimate support for a denture is provided by the underlying bone which is covered by � mucous membrane. principle and technique of complete denture-iwao hayakawa �

HARD TISSUE The success of complete � denture prosthesis particularly dependent on the degree of stability that the underlying bone can maintain. The structure of alveolar � ridge has a direct relation on stability and retention of completed prosthesis.

� Bone of maxilla and mandible is formed by outer cortical bone and central meduallary cavity filled with red or yellow bone marrow. � The marrow cavity is intercepted throughout its length by reticular network of trabecular (alternatively cancellous or spongy bone). These internal trabeculae act as reinforcement � rods to support outer thicker cortical crust of compact bone. bouchers prosthodontic treatment for edentulous �
 CT membrane Periosteum consists of")
Surrounding every compact bone is osteogenic (bone � forming) CT membrane Periosteum consists of 2 layers. Inner layer - next to bone surface consists of bone � cells their precursors and a rich micro vascular supply. Outer layer - is fibrous layer giving rise to sharpey � fibres. hand book of osteology -s. poddar, ajay bhagat. �

� The requirements of a successful complete denture include; Compatibility with the surrounding oral environment. � Restoration of masticatory efficiency within limits. � Ability to function in harmony during mastication, � speech, respiration and deglutition. Esthetic acceptability. � Preservation of that which remains. � principlesand technique of complete denture- Iwao hayakawa. �

ALVEOLAR BONE Healing of bony sockets after tooth extraction is similar to that of bone � fractures which is: Primary clot formation in the socket. � Organisation of clot by proliferating young CT’s. � Gradual replacement of young CT’s by coarse fibrillar bone. � Reconstruction by resorptive activity on one side and replacement of � immature bone by mature bone on the other and , Epithelialisation and healing of the surface occurring simultaneous with � other reparative processes. syllabus of complete denture -charles m. heartwell �

� During the period of general body growth, the rate of bone formation exceeds the rate of bone resorption. In the adult, the two processes are more nearly balanced. In the aged or in any person with local or systemic disease, the rate of � bone resorption exceeds that of formation. This is only one of the many reasons some dentures appear to be � physiologically tolerated over a period of time and then seem to fail. syllabus of complete dentures-charles m. heartwell �

DIRECTION OF RIDGE RESORPTION The maxilla resorb upward and inward to become progressively smaller because of the inclination of the teeth and the alveolar process. � The opposite is true for the mandible , which inclines outward and progressively wider. � mastering the art of complete denture-halperin , graser, rogoff �

BLOOD SUPPLY The blood supply to bone of maxillae and mandible is derived � principally from medullary and periosteal vessels that form plexuses. When teeth are present, intra-osseous vessels supply pulpal, periodontal and alveolar branches. These various vessels anastomose with periosteal, gingival and other � vessels supplying the surrounding soft tissues. However, in edentulous patient, the pulpal, periodontal and depending on extent of alveolar bone resorption the alveolar branches are lost. syllabus of complete denture-charles m. heartwell. jr �

� The blood to the mandible comes from branches facial, buccal and lingual arteries instead of inferior alveolar artery. The relationship between these and other changes in the blood supply to � RR may influence the biologic responses of denture supporting tissues to preprosthetic surgery and to the success of subsequently fabricated dentures. syllabus of complete denture -charles m. heartwell �

� The following represent some ways the dentist and patient can help make a denture better tolerated by bony support. ; Record tissues in impression at their rest position. � Decrease the number of teeth. � Decrease size of food table. � Develop an occlusion that eliminates, as much as possible horizontal and � torque force. principles and techniques of complete denture-Iwao hayakawa. �

Extend denture base for maximum coverage within � tissue limits. Eat by placing small masses of food over the � posterior teeth where supporting bone is best suited to resist forces. Remove dentures for 8 hour of every 24 hour. � principles and technique of complete denture- Iwao � hayakawa

Oral submucous membrane The bone of upper and lower edentulous jaws, and the oral cavity is lined with a soft tissue that is known as ‘mucous membrane’. Denture bases rest on the mucous membrane, which serve as a cushion between denture base and supporting bone. The mucous membrane composed of : - (i) Mucosa (ii) Sub mucosa syllabus of complete denture – charles m. heartwell
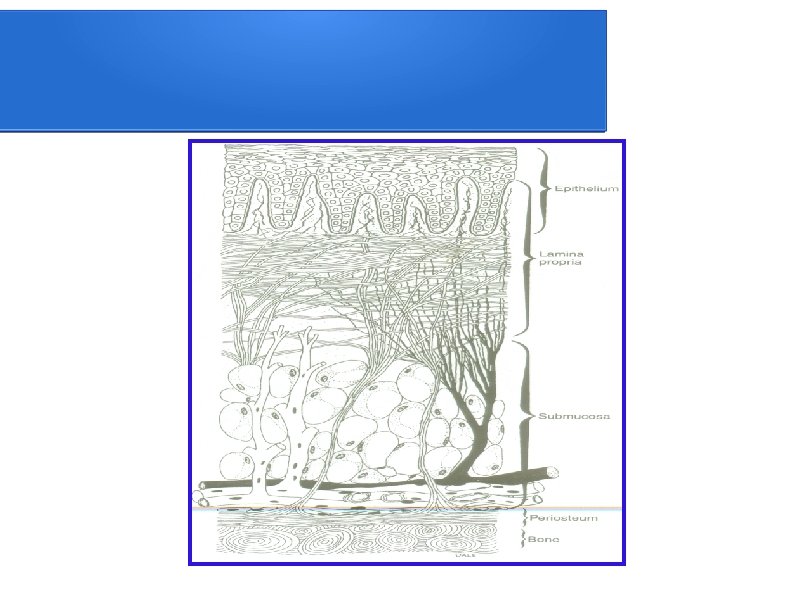

MUCOSA. �Mucosa is formed by stratified squamous epithelial cells. � There is subadjacent narrow layer of connecting tissue to the mucosa, known as lamina propria. Syllabus of complete denture- charles m. heartwell �

SUBMUCOSA � Sub mucosa is formed by connective tissue. Connective tissue varies in character from dense to loose alveolar tissue and also varies considerably in thickness. � It may contain glandular, fat or muscle cells. � Submucosa transmit the blood and nerve supply to the mucosa. � Sub mucosa attaches mucosa to the periosteal covering of the bone. � Syllabus of complete denture-charles m. heartwell �

� The oral mucosa can be divided into three categories depending on its location in the mouth and its function. They are � Masticatory mucosa - which covers the crest of residual ridge, � including residual attached gingiva, firmly adherent to supporting bone. Secondly the hard palate. � orbans textbook of oral histology and embryology- g. s. kumar �

� The masticatory mucosa is characterised by well- keratinised layer on its outermost surface that is subject to changes in thickness depending on whether dentures are worn and on the clinical acceptability of dentures. Lining mucosa - is generally found to cover the mucous membrane in the oral cavity that is the firmly attached to periosteum of the bone. Orban's textbook of histology and embryology-g. s kumar

It forms the covering of lips and cheeks, the � vestibular spaces, the alveololingual sulcus, the soft plate, the ventral surface of tongue, and the unattached gingiva found on slopes of residual ridges. It is devoid of keratinised layer and is freely movable � with the tissues to which it is attached because of its elastic nature of lamina propria. orban's textbook of oral histologyand embryology- � g. s. kumar

The specialized mucosa - covers the dorsal � surface of tongue. The mucosal covering is keratinised and includes specialized papillae on upper surface of tongue. Orban's textbook of oral histology and embryology � -g. s kumar

ANATOMICAL LANDMARKS

LIMITING STRUCTURES Labial frenum Labial vestibule Buccal frenum Buccal vestibule Lingual frenum Alveolingual sulcus Retromolar pads Pterygomandibular raphe SUPPORTING STRUCTURES Buccal shelf area Residual alveolar ridge

RELIEF AREA Mylohyoid ridge Mental formen Genial tubercles Torus mandibularis Textbook of prosthodontics – v. rangarajan

MANDIBULAR SUPPORTING AREAS

RESIDUAL ALVEOLAR RIDGE - covered by keratinized layer and firmly attached to the periosteum - cancellous in nature, does not have a good cortical plate covering it Significance -hence it is a secondary relief area, usually relieved during impression. boucher's prosthodontic

SLOPES OF RESIDUAL ALVEOLAR RIDGE - has thin plate of cortical bone Significance - because walls are steep and at an angle to occlusal forces, it is not suited for primary stress bearing, hence it is secondary stress bearing. syllabus of complete denture-charles m. heartwell

BUCCAL SHELF AREA Buccal shelf area - bounded by anteriorly – buccal frenum posteriorly – retromolar pad medially – crest of alveolar ridge laterally – external oblique ridge Inferior part of buccinator is attached in the buccal shelf area, but does not interfere with the denture because the fibers runs anteroposteriorly.

Significance � buccal shelf area may be very wide and is at right angles to the vertical occlusal forces. For this reason it offers excellent resistance to such forces. � hence considered as primary stress bearing area. � syllabus of complete denture charles m. heartwell. �

RELIEF AREAS OF MANDIBLE

MYLOHYOID RIDGE bony ridge found on lingual side of the mandible - mylohyoid muscle is attached to this ridge - soft tissue usually hides the sharpness of the ridge, which can be found by palpation - anteriorly the muscle attaches close to the inferior border of the mandible and posteriorly it may flush with superior surface of residual ridge. boucher's prosthodontic treatment for edentulous patients

significance - level, inclination and prominence vary widely between patients - thin, sharp mylohyoid ridge can result in soft tissue irritation when denture is placed over it. Surgical correction may be required - height of the lingual flange is determined by the mylohyoid ridge. boucher's prosthodontic treatment of edentulous patients

MENTAL FORAMEN AREA This is of concern when the ridge is extremely resorbed � Foramen is found near or on the ridge crest in premolar region � significance � In such cases it should be relieved � Pressure on mental nerve can cause numbness of the lip. Syllabus of complete denture charles m. heartwell. �

TORUS MANDIBULARIS rounded prominences found in some individuals � located in the region of premolars, midway between soft tissues of the floor of the mouth and crest of the ridge significance -covered by a thin layer of mucous membrane which may be irritated by the denture, it should be relieved when present. Boucher's Prosthetic treatment of �

-large tori should be surgically removed if they interfere with denture seal

GENIAL TUBERCLE These are pair of bony tubercles found anteriorly on the lingual side of the mandible. � Due to resorbtion , it may become increasingly prominent making denture usage difficult � Superiorly , it is attached with genioglossus muscle and there inferior tubercle gives attachment to the geniohyoid muscle. � Boucher's prosthetic treatment for edentulous patients. �

MANDIBULAR LIMITING STRUCTURES

LABIAL FRENUM contains a band of fibrous connective tissue that helps to attach the orbicularis muscle � the frenum is quite sensitive and active � the denture must be fitted carefully to maintain seal without causing soreness �

LABIAL VESTIBULE extends from labial frenum to the buccal frenum � length and thickness of the labial flange vary with amount of tissue that has been lost � There is muscle extending from the residual ridge to the lip, the two depressor anguli oris, so the labial flange can be extended in length and thickness to provide support to the lip. �

The mucous membrane lining the labial vestibule is relatively thin and is classified as lining mucosa � When the patient’s mouth opens wide, the orbicularis oris muscle becomes stretched, narrowing the sulcus. � This would displace the mandibular denture if the flange is unnecessarily thick. hence, impressions will always be narrowest in the anterior labial region �

The extent of � denture flange in this � region often is limited � because of the � muscles that are � inserted close to the � crest of ridge. � The � mentalis muscle is � particularly active in � this region. � Boucher's prosthetic treatment for edentulous patients. �

Significance � It accomdates the labial flange of the dentures � It forms a part of peripheral seal areaa � Boucher's prosthetic treatment for edentulous patients �

BUCCAL FRENUM Is a band of fibrous connective tissue two or more in number � Depressor anguli oris is the muscle which influences the frenum � Hence it is active and sensitive, has to be relieved in � Boucher's prosthetic treatment for edentulous patients �

It is an active frenum as the fibres of the triangularis, zygomaticus and caninus muscles converge here to form a strong but movable base from which the orbicularis oris and buccinator may operate as antogonists. � These fibrous and muscular tissues pull actively across the denture borders, therefore the impression must be functionally trimmed to have the maximum seal and yet not displace the denture when lip is moved. � Boucher's prosthetic treatment for edentulous patients �

BUCCAL VESTIBULE it extends form the buccal frenum posteriorly to the retromolar region �buccinator attaches in the lower side in the molar region in the buccal shelf of the mandible � The extent of buccal vestibule is influenced by the buccinator muscle, which extends from the modiolus anteriorly to the � Boucher's prosthetic treatment for edentulous patients pterygomandibular raphe �

Extension of distobuccal border at the end of buccal vestibule is influenced by masseter muscle activity. � � When the masseter contracts, it’s anterior fibres alters the shape and size of the distobuccal end of lower buccal vestibule by pushing inward against the buccinator muscle. � Boucher's prosthetic treatment for edentulous patients �

. LINGUAL FRENUM � It is a mucosal fold that orginates at � the midline, under the tongue and often terminates at the sublingual salivary caruncles. Fibrous band of tissue that overlies � the centre of genioglossus muscle. It is usually a narrow single band of tissue but may be broad and exist as two or more frenums. Boucher's prosthetic treatment for edentulous patients �

It originates at midline under surface of tongue and often terminates at � the sublingual (salivary) caruncles. it crosses and bisects the sublingual crescent space and attaches to � lingual aspect of mandibular ridge. Often it fans out to find a broad insertion in alveolar mucosa. This structure should be palpated for tension during tray adjustment � procedure. Careful clearance is needed in the denture because the lingual frenum is attached to tongue and inadequate clearance may result in pain or displacement of denture. Boucher's prosthetic treatment for edentulous patients �

Just beneath the lingual frenum genioglossus muscle is found which originates from superior genial tubercles. � It is a powerful and active but fortunately narrow muscle. Anterior fibers of this muscle when tensed raises up from floor of mouth and impinge on lower denture base � Boucher's prosthetic treatment for edentulous patients �

Frenums are basically fibrous connective tissue. � They do not contract or expand like muscles but rather are ligaments. They are accessory limiting structures for tongue, lips, and muscles of cheek. Boucher's prosthetic treatment for edentulous patients �

ALVEOLINGUAL SULCUS It is the space between the residual ridge and tongue. � It extends posteriorly from lingual frenum to retromylohyoid curtain. Part of it is available for the lingual flange of denture. The alveololingual sulcus can be considered in 3 � regions Boucher's prosthetic treatment for edentulous patients �
 � This extends from lingual frenum to where")
1. The anterior region (Premylohyoid fossa) � This extends from lingual frenum to where the mylohyoid ridge curves down below the level of sulcus. This fossa results from the concavity of mandible joining � the convexity of mylohyoid ridge. Lingual border of impression in anterior region make � definite contact with mucous membrane of mouth when tip of tongue touches upper incisors. Boucher's prosthetic treatment for edentulous patients �

2. middle region The part of alveololingual sulcus � extends from premylohyoid fossa to distal end of mylohyoid ridge curving medially from the body of mandible. When mylohyoid muscle and � tongue are relaxed, the muscle

If the lingual flange slopes towards the tongues, the � tongue can rest on top of flange and aid in stability of lower denture on RR it also prevents displacing the denture during tongue movements and swallowing thus maintaining the seal. � The length and width of mylohyoid flange is determined by membranes attachment of tongue to mylohyoid ridge and width of hyoglossus muscle and can only be determined by skilful border molding and � Boucher's prosthetic treatment for edentulous patients impression.

The lingual borders in mylohyoid areas are formed by � contact with mylohyoid muscles in a functional but not extreme contracted or elevated position. The average mylohyoid border is 4 -6 mm below � mylohyoid ridge fair-good ridge-width 2 -3 mm. Boucher's prosthetic treatment for edentulous patients �
 � It extends from end of mylohyoid ridge")
3. The posterior region (Retromylohyoid fossa/space) � It extends from end of mylohyoid ridge to retromylohyoid curtain being bounded on lingual by anterior tonsillar pillar, at the retromylohyoid distal curtain end , by superior constrictor and on buccal by mylohyoid muscle, mandibular ramus and retro

The superior support for retromylohyoid curtain is � provided by superior pharyngeal constrictor. The action of the muscle and the tongue determine the posterior extent of lingual flange. Pouch shaped retromylohyoid space is lined completely � with loosely attached mucosa. There are no supporting structures here since the medial � surface of mandibular body slope obliquely outward from mylohyoid ridge to mandibular border forming

� Distal to mylohyoid muscle the space dips toward and outward to permit formation of retromylohyoid eminence of mandibular denture. Boucher's prosthetic treatment for edentulous patients �

EXTERNAL OBLIQUE RIDGE the EOR does not govern the extension of the buccal flange because the resistance or lack of resistance encountered in this region varies widely � buccal flange may extended to the EOR, or up on to it, or even over it, depending on the location of the mucobuccal fold. �palpation of EOR is a valuable aid or landmark in helping to ascertain the relative amount of resistance or lack of resistance of the border tissues in this �

RETROMOLAR PAD Definition – “a mass of tissue comprised of non-keratinized mucosa located posterior to retromolar papilla and overlying loose glandular connective tissue”. � � GPT-8 � Is a triangular soft pad of tissue at distal end of lower ridge � Must be covered by the denture to perfect the border seal in this region � Boucher's prosthetic treatment for edentulous patients

Its mucosa is composed of a thin, nonkeratinized epithelium, and in addition to loose alveolar tissue. � its submucosa contains; � glandular tissue, � fibers of the buccinator and superior constrictor muscles, � the pterygomandibular raphe, and � terminal part of the tendon of the temporalis muscle. � Boucher's prosthetic treatment for edentulous patients �

action of these muscles limit the extent of the denture and prevents placement of extra pressure on distal part of the retromolar pad � Boucher's prosthetic treatment for edentulous patients �

PTERYGO MANDIBULAR RAPHE � The pterygo mandibular raphe or ligament originates from the pterygoid hamulus of medial pterygoid plate and attaches to distal end of pterygoid ridge. It is partly the origin of buccinator muscle laterally and the superior � constrictor muscle medially. It is quite prominent in some patients and may even require , notch like � clearance in maxilla denture. A simple wide-open digital and visual inspection will usually determine whether clearance is required or not. syllabus of complete denture- charles. m. heartwell �

Tendinuos pterygomandibular raphe extends inferiorly from pterygoid hamulus inserting in the trigonum retromolar and retromolar pad � The raphe is covered by a fold of mucous membrane, plica pterygomandibularis � When mouth is opened widely, the raphe is stretched, causing plica to stand out like string between the pterygoid hamulus and retromolar pad �

Significance: � � Streched raphe lifts the posterior part of retromolar pad, denture that has been extended on to this structure may be dislodged during energitic opening movement of the mandible. � syllabus of complete denture- charles m. heartwell �

� Mental foremen It is located on the lateral surface of body of mandible between the first and second bicuspids about halfway between the lower border of mandible and the alveolar crest. If the loss of RR is extensive, the foramen occupies a more superior position and denture base must be relieved over the foramen to keep the denture base from irritating the mental neurovascular bundle failing which the pressure exerted will cause numbness of lower lip. syllabus of complete denture- charles m. heartwell �

Lingual tuberosity � It is an irregular bony prominence on distal end of mylohyoid line. When this area is excessively prominent or rough it may present an undesirable undercut requiring surgical intervention. Mental spines � They are situated on lingual aspect of mandibular body in midline slightly above the body. . syllabus of complete denture- charles m. heartwell �

These bony elevations are often divided � into a superior and an inferior section and sometimes into right and left prominences. When loss of RR is extensive these spines are more superior position than crest of existing ridge, requiring surgically intervention syllabus of complete denture- charles m. heartwell �

ANTERIOR LINGUAL VESTIBULE �. � mainly influenced by genioglossus, lingual frenum and anterior portion of sublingual gland � lingual frenum is superimposed over genioglossus which is attached to genial tubercles � if ridge is highly resorbed, the genial tubercles are at higher level– little or no vestibular space � The lingual border of the impression in this region should extend down to make definite contact with the mucous membrane floor of mouth, when the tip of the tongue touches the upper incisors.

MIDDLE LINGUAL VESTIBULE OR MYLOHYOID AREA Is the largest area and is mainly influenced by the mylohyoid and by sublingual glands �Sublingual gland lies above the mylohyoid muscle. The gland is raised when the mylohyoid contracts during swallowing � If the denture border is made short to relieve the raised sublingual gland, a space will occur between the denture border and the mucosa when the mylohyoid is at rest and thus the peripheral seal will be lost. � priciples and techniques of complete denture -Iwao � hayakawa.

DISTOLINGUAL VESTIBULE. Space distal to the mylohyoid muscle is referred to as the retromylohyoid fossa anteriorly ----mylohyoid muscle posterlaterally ---superior constrictor posteromedially – palatoglossus medially --- tongue laterally ---pear shaped pad priciples and techniques of complete denture -Iwao � hayakawa.

There is no structure and so it is possible to lengthen the denture border into this space � the ‘s’ shaped curve of mandibular denture results from strong instrinsic a nd extrinsic muscles of tongue which usually place retromylohyoid borders more laterally and toward retromylohyoid fossa as they oppose the weaker superior constrictor muscle �

TONGUE POSITION In normal position, the tongue appears � relaxed and completely fills the lower arch with its apex lightly contacting the lingual of lower teeth. this is important to obtain lingual border seal. If the tongue retrudes while opening the � mouth then it is virtually impossible to get the lingual seal.

MUSCLE ATTACHMENTS. . . .

The musculature of denture space is divided into 2 groups � Those muscles which primarily dislocate the denture during activity � Vestibular dislocating muscles � Lingual dislocating muscles � Those muscles that fix the denture by muscular pressure on its secondary supporting surfaces � Vestibular fixing muscles � Lingual fixing muscle � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

VESTIBULAR DISLOCATING MUSCLES Masseter muscle region Masseter muscle contracts, it alters the shape and size of distobuccal end of the lower buccal vestibule � It pushes inwards against the buccinator, hence the distobuccal borders of the mandibular denture must converge rapidly to avoid article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS displacement � �

MENTALIS MUSCLE Origin: � Frontal surface of the mandible between alveolar jugum of lateral incisor and canine eminence. � Extends inferiorly, anteriorly, and medially to fuse in midline with corresponding muscle fibers from the opposite side. � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

SICHER AND TANDLER drew attention to the important fact that the origin of the mentalis is located closer to the crest of the RR than the mucosal reflection in alvelolabial sulcus � Consequently the bottom of the sulcus is lifted when mentalis contracts and their by the depth and space of the oral vestibule can be decreased considerably � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

INCISIVE LABII INFERIORIS MUSCLES ORIGIN: From lower canine jugum runs laterally and extends anteriorly towards the angle The fibers of this muscle become fused with fibers of the orbicularis oris muscle Has same effect as that of mentalis muscle ie. Contraction of this muscle reduces denture space by raising the bottom of the sulcus article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

LINGUAL DISLOCATING MUSCLE Medial pterygoid muscle � Originates from pterygoid fossa, inserted on the medial surface of ramus of mandible � Determines the extension of the denture in lower posterior lingual part of denture space � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

Palatoglossus muscle Posterior lingual part of the denture space is further influenced by palatoglossus running in palatoglossal arch The muscle descends from the soft palate in the arch to enter in to lateral margin of the tongue During deglution, the palatoglossus contracts, by this action the mucosa covering the lower part of muscle is lifted superiorly, anteriorly, medially article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

MYLOHYOID MUSCLES; � Forms the floor of the oral cavity � Originates from mylohyoid line, runs medially to meet and insert in fibrous mylohyoid raphe. Posterior fibers inserts directly on the frontal portion of the body of hyoid bone � The two mylohyoid muscle thus form a berth like structure in which the tongue rests � When both mylohyoid muscle contracts, the floor of oral cavity is lifted and tongue is pressed against the palate, changing the denture space � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

The alvelolingual sulcus will be displaced upwards and posterior part of sulcus will change from almost vertical position to nearly horizontal one �

TENDONS OF GENIOGLOSSUS MUSCLES Short but powerful tendons that run into genioglossus muscle arises from genial spines, located lingually on mandibular symphysis � Peritendinous tissue of the tendon is covered by lingual frenum � When the apex of the tongue is lifted, tendinous fibers as well as lingual frenum will be passively streched and lifted, thus easily being capable of pressing on the borders of the lower denture with a dislocating effect article on dynamic nature of lower dentures JPD-1965, 15 (3)-n � � . brill, dr. odont, g tryde LDS, R. cantor. DDS

LABIAL AND BUCCAL FRENUM Alveololabial sulcus is interrupted in the region of mandibular central incisors by a fold in mucous membrane. , labial frenum � Similarly the alveolobuccal sulcus is interrupted by the buccal frenum in cuspid and bicuspid region � These folds of mucous membrane cover strands of CT fibers that extend from periosteal tissue of the alveolar bone, crosses the vestibular sulcus and blend into submucosa of lower lip and cheeks article on dynamic nature of lower dentures JPD-1965, 15 (3)-n � With slightly resorbed alveolar process, the � � . brill, dr. odont, g tryde LDS, R. cantor. DDS

VESTIBULAR FIXING MUSCLES Buccinator � Has a horseshoe shaped origin � The maxillary part originates from the molar region at the base of the alveolar process and runs posteriorly and inferiorly past the maxillary tuberosity to continue into pterygomandibular raphe � Significance: � The cheeks are pressed against dental arches. When the buccinator muscle is contracted � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

During chewing and swallowing the muscle is rhythmically coordinated with the muscles of mastication � Buccinator assists in positioning food between the teeth and returning food that has escaped into the vestibular sulcus to the occlusal table � Therefore, buccinator is sometimes called as accessory muscle of mastication � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

LINGUAL FIXING MUSCLE Main bulk of the tongue is made up of straited muscles � Extrinsic and intrinsic group of muscles � Extrinsic M have their origin external to the tongue, but their course terminates within it. Their contraction maintains a certain position of the tongue � Palatoglossus, styloglossus, genioglossus, hyoglossus � Intrinsic M lie completely within the article on dynamic nature of lower dentures JPD-1965, 15 (3)-n tongue and their activities sustain or � � . brill, dr. odont, g tryde LDS, R. cantor. DDS

PASSIVE MUSCLE FIXATION The denture can be fixed by the mass and weight of these structures and through the pressure exerted by the muscle tonus � Inclination of polished surfaces: � -buccal flanges must slope inferiorly and laterally and borders must extended out beneath a fold of the buccinator � -lingual flanges must extend inferiorly and medially below the anterior and lateral parts of the tongue, as far as permitted by range of action of tongue �

LINGUAL SPACES FOR EXTENTIONS FOR RETENTION Sublingual crescent space -is in anterior part of the floor of mouth above the sublingual gland - tissues bounding this space move freely and thus the anterior lingual flange can be extended horizontally whenever the tongue and tissues permit Sublingual fossa -during swallowing the mylohyoid article on dynamic nature of lower dentures JPD-1965, 15 (3)-n raises with the tongue and brings the floor � . brill, dr. odont, g tryde LDS, R. cantor. DDS

- frequently this muscle is shows signs of flabbiness and it is possible to extend the lingual flange of denture for additional retention � Retromylohyoid fossa � -Is below and behind the retromolar pad � -This space provides an excellent place for extending the denture for positive retention especially when extensions into sublingual crescent and sublingual fossa cannot be made. � article on dynamic nature of lower dentures JPD-1965, 15 (3)-n . brill, dr. odont, g tryde LDS, R. cantor. DDS �

NEUTRAL ZONE CD are primarily mechanical devices, but since they function in the oral cavity, they must be fashioned so that they are in harmony with normal neuromuscular function. � All oral functions. � Failure to recognise the cardinal importance of tooth position and flange form and contour often results in dentures which are unstable and unsatisfactory. � When all of the natural teeth have been lost, there exists within the oral cavity a void which is the potential denture space. � Syllabus of complete dentures-charles m. heartwell. �

The neutral zone is that area in the potential denture space where the forces of the tongue pressing outward are neutralized by forces of the cheeks and lips pressing inward � The central thesis of the neutral zone approach to complete dentures is to locate that area in the edentulous mouth where the teeth should be postioned so that the forces exerted by muscles will tend to stabilize the denture rather than unseat it. � Where the alveolar ridge has been lost, denture stability and retention are more dependent on correct position of the teeth and contour of the external surfaces of the dentures. � Syllabus of complete dentures-charles m. heartwe � ll

SUMMARY

CONCLUSION

REFERENCES PROSTHODONIC TREATMENTS FOR IDENTOLOUS PATIENTS -GEORGE. A. ZARB, JUDSON . C. HICKEY, CHARLES. L. BOLENDER [9 TH, 12 TH EDITION] � PRINCIPLES AND TECHNIQUE OF COMPLETE DENTURE. -IWAO HAYAKAWA � ESSENTIALS OF COMPLETE DENTURE PROSTHODONTICS[2 ND EDITION] -SHELDON WINKLER � CLINICAL DENTAL PROSTHETICS[2 ND EDITION]H. R. B FENN, K. P LIDDELOW, A. P. GIMSON � MASTERING THE ART OF COMPLETE DENTUREHALPERIN, GRASER, ROGOFF/PLEKAVICH. �
 � N. BRILL, DR. ODONT,")
THE DYNAMIC NATURE OF LOWER DENTURES JPD 1965; 15(3) � N. BRILL, DR. ODONT, G. TRYDE. � STABILIZING LOWER DENTURES ON UNFAVOURABLE RIDGES JPD 1962; 12. � SIGNIFICANCE OF AGE CHANGES IN HUMAN ALVEOLAR MUCOFOSSA AND BONE CHARLES. I. NEDELMAN, S. D. BERNICK JPG 1978; 39(5) �
- Slides: 105