Visual Consequences of Concussion Dr Jennifer Kungle NeuroOptometrist




 Im. PACT Testing Sports")




















 Can be ground into")


 can vary from opaque (light perception)")





- Slides: 45
Visual Consequences of Concussion Dr. Jennifer Kungle Neuro-Optometrist The Center for Vision Development
Coup Contra-Coup Injury
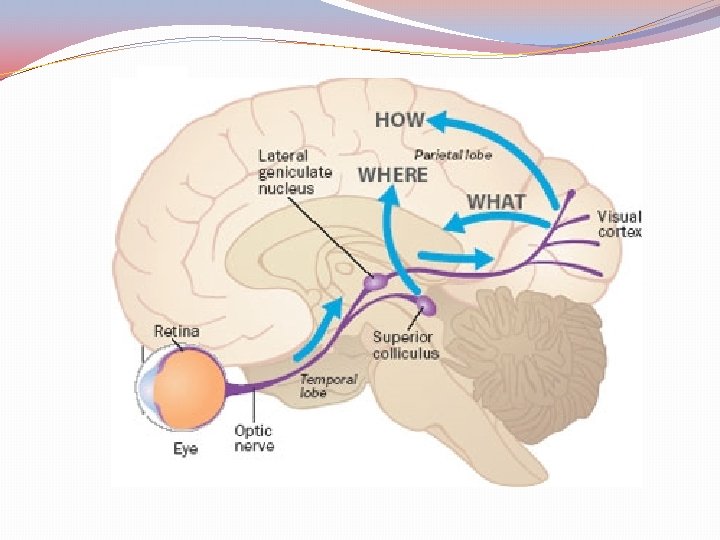
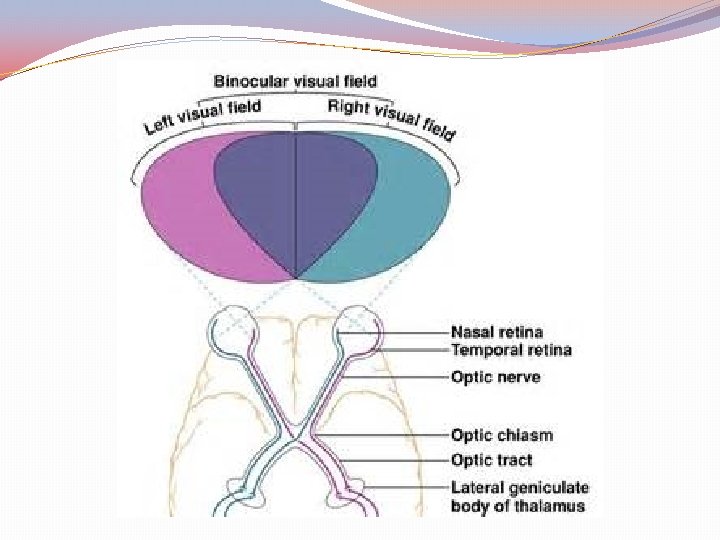
The Visual Pathway
Key Visual Signs/Symptoms Ø Ø Ø Ø Headache Blurry vision Photophobia Double vision Reading problems Decreased processing speed Dizziness/motion sickness Peripheral vision defects ü Nearly 30% of concussed athletes report visual problems during the first week after the injury
Baseline Testing 1. Cognitive Baselines Standardized Assessment of Concussion (SAC) Im. PACT Testing Sports Concussion Assessment Tool, SCAT-2 2. Balance Baseline Computerized Timed Tandem Gate Test 3. Visual Baseline/Remove from Play King Devick Saccadic Test VOMS Right. Eye Neuro Vision
Im. PACT q Immediate Post-Concussion Assessment and Cognitive Testing, developed by UPMC q Neuro-cognitive test that evaluates multiple aspects of memory, attention, brain processing speed, reaction time, and post-concussion symptoms. q Designed for children above 8 years of age. q Baselines should be repeated every two years for >13 yo q Baselines mandated by NFL, NHL and many collegiate and high school teams. Ø Impacttest. com to find providers
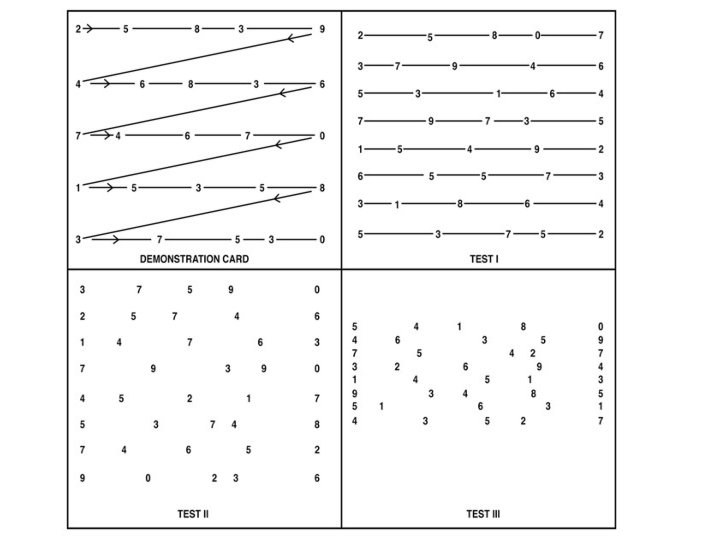
King Devick Saccadic Test
King Devick Saccadic Test q The K-D Test has been widely used through the years as a measure of saccade function primarily as related to reading. q Measures rapid eye movement, visual tracking and related cognitive responses; is a reliable indicator of cognitive problems. q If an injured athlete reads the numbers more slowly after a head impact as compared to baseline testing, he or she is considered to have sustained a concussion.
September 10, 2015, in Concussion q 1419 athletes; 86% specificity detecting concussion Ø King-Devick times 4. 8 seconds slower for concussed athletes vs. 1. 9 seconds faster for nonconcussed Ø Physical exertion sharpens visual processing, often causing non-concussed athletes to perform better than their baseline Critique: does not evaluate other areas of ocular motor function such as pursuits, convergence, or accommodation
Vestibular Ocular Motor Screening VOMS – developed at UPMC Assessments in the following five domains: 1) smooth pursuits 2) horizontal and vertical saccades 3) convergence 4) horizontal and vertical vestibular ocular reflex (VOR) 5) visual motion sensitivity (VMS) Following each VOMS assessment, patients rate on a scale of 0 (none) to 10 (severe) symptoms of: headache, dizziness, nausea and fogginess Takes 5 -10 mins to administer.
Eye Tracking Technology
Ø Ø Ø Circular smooth pursuit Horizontal smooth pursuit Vertical smooth pursuit Horizontal volitional saccades Vertical volitional saccades Ø Sample_Neuro_Report_Feb_2017. pdf
The Duality of the Visual System Focal Vision System What/How Pathway q High-resolution, central vision = identification of objects v Attention v Concentration v Detail-oriented q Conscious q Reactive Ambient Vision System Where Pathway q “Peripheral Vision System” v Localizes our bodies in space v Balance, Movement, Coordination, Posture q Gravity-Specific q Pre-Conscious q Anticipatory q Stimulated by motion
Ambient Processing In the midbrain visual inputs combine and organize sensory information with information from q Vestibular (VIII) q Proprioceptive q Tactile q Kinesthetic After acquiring additional sensory input, nerves travel in a feed-forward mechanistic process to the visual cortex.
Sensorimotor Connection All sensory systems are integrated neurologically. While initially separate, they all join together to integrate sensorimotor information in the brain. q Some patients note that when they take off their glasses they have difficulty hearing q Not only sensory system share information – also the motor process (efferent pathway) is critical in providing a background for the sensory system. ex. Balancing on one foot – much more difficult when eyes are closed.
Ambient Processing The ambient system is responsible for grounding our spatial world through sensorimotor matching. When this system is damaged by injury, grounding is affected and there is a shift towards focalization. = Focal Binding This causes the person to project movement onto stationary objects which are fixated, and they perceive objects to be moving. i. e. print on the page may appear to move
Ambient Processing When in busy, visually stimulating environments, this over focalization and isolation on detail will be overstimulating – causing confusion and spatial distortion.
What happens with TBI? q In a neurological event such as a TBI, MS, cerebral palsy, autism, CVA, etc. , the balance between the ambient and focal visual processes is often affected. q M-cells have larger diameter axons and are more susceptible to damage. Damage can come from ischemia, space occupying lesions, etc. q m. TBI – concussion – diffuse shearing of axons leads to release of neurotoxins – creates hyper excitability – throws off the ambient system
AMBIENT PROCESSING BECOMES DECOUPLED FROM FOCAL PROCESSING = focal binding unable to process peripheral information q Exophoria/exotropia q Diplopia ü Reduced depth perception/localization ü Unable to match visual to proprioceptive, kinesthetic, vestibular information ü Balance, coordination and movement are compromised ü Are unable to suppress second image
Post Traumatic Vision Syndrome Characteristics: 1. Exotropia/High Exophoria 2. Convergence Insufficiency 3. Accommodative Deficiencies 4. Visual Spatial Distortions 5. Oculomotor Deficits Unstable AMBIENT system
Post Traumatic Vision Syndrome Symptoms 1. Diplopia, possible 2. Objects appear to move 3. Reduced concentration and attention 4. Poor visual memory 5. Glare sensitivity (photophobia) 6. Problems with ü Balance ü Coordination ü Posture
Vision Rehabilitative Therapy 1. 2. 3. 4. 5. 6. 7. Binocular Integration Oculomotor control, speed, accuracy Accommodative flexibility, stamina and endurance Smooth and easy convergence/divergence Peripheral Awareness Visual Motor Coordination Visual Perceptual Spatial Knowledge
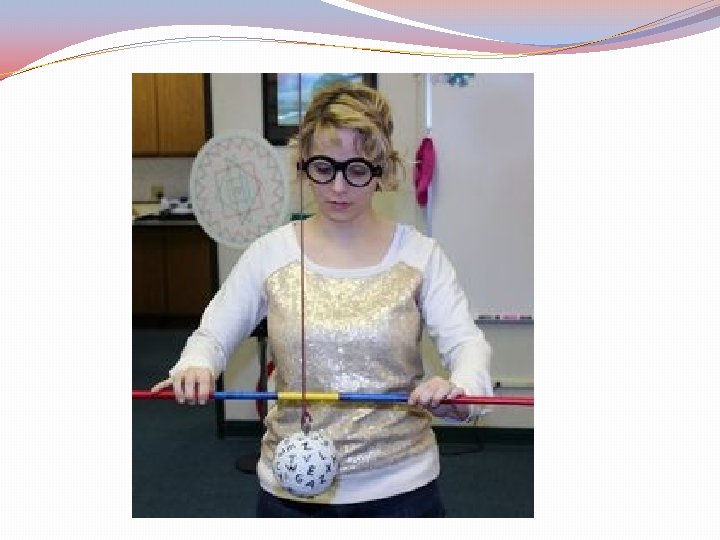
Multi-Matrix Game
Neuro-Optometric Treatment Options 1. Lenses Avoid Multifocals Always consider two pairs of glasses May require additional computer Rx or sun Rx Polarized/Transition Lenses Tints
Neuro-Optometric Treatment Options 2. Compensatory Prisms Fresnel Press-On Prisms (temporary) Can be ground into standard lenses
Fresnel Prism
3. Therapeutic Prism Base In yoked prism helpful in decreasing visual stress; aids divergence; decreases photophobia and eyestrain Yoked prism can be used to realign a patient’s center of gravity and improve overall balance
4. Patches v Cling Patches (Bangerter Occlusion Foils) can vary from opaque (light perception) to varying degrees of translucency Provide varying acuities, i. e. 20/50, 20/200, light perception
Occlusion Options Partial or spot patches can be used as immediate treatment for double vision. Partial patches will allow the patient to maintain peripheral awareness and facilitates their overall coordination and balance. Occlusion Therapy without an assessment is NOT recommended.
Superior Occlusion
Spot Occlusion
Binasal Occluders
THANK YOU! marylandvisiontherapy. com drkungle@marylandvisiontherapy. com Nora. cc COVD. org Oepf. org Neuro-Optometric Rehabilitation Association College of Optometrists in Vision Development Optometric Education Foundation 45