Understanding Psychological Assessments Making a referral and understanding











 truth/scientific")
 Parenting competency and what would be")
 Court may order a person to go out and")





 Dear Dr. Strange, Please accept")
 or a nurse with specific training")

 Dear Dr. Banner, Please accept this")



 Dear Dr. Fate, Please accept this")
 Usually conducted by")


 Dear Dr. Mid-Nite, Please accept")

")
 Dear Dr. Druid, Please")

 Dear Dr. Xavier, Please accept")





 Intellectual disability diagnosis requires IQ below 70 (some use")



 6 to 16 years old")


 5 to 94 years old Can")



 Minnesota Multiphasic Personality Inventory-Adolescent (MMPI-A) Millon")

 Beck Anxiety")












- Slides: 68
Understanding Psychological Assessments Making a referral and understanding the results Espen Klausen, Ph. D. , Licensed Psychologist with Fond du Lac County Department of Community Programs DSS Hot Topics 02/15/2018
Presentation Plan Types of assessments and how to refer well Understanding assessment results These slides contain a lot of informationand examples that will not be discussed but are here for your reference in the future
Please Note Psychological assessments is the unique domain of clinical psychologists Most psychologists have 5 -6 years training in assessments (not counting postdoctoral training) School psychologists assess within the domain of educational needs Masters level psychometricians assess under the guidance of a clinical psychologist Some other mental health professionals can do diagnostic assessments Court allows psychiatrists to perform some forms of forensic assessments
Please Note Many psychological tests are protected by law and sharing the content with nonpsychologists can be illegal or otherwise unethical The actual test protocols are not shared and not a part of the medical record that can be released (although the written analysis by the psychologist would be) The assessment client can usually not be accompanied by others while doing the actual psychological tests beyond the interview To protect the validity of the test in the future To protect the validity of the assessment in the moment (e. g. , client is not influenced)
If you are going to refer for a psychological assessment, also consider assessment for A physical with the primary care physician can screen for most of these: Hearing Vision Sensory problems (Physical Therapist) Thyroid/hormonal issues Iron deficiency or other nutritional issues Diabetes/other blood sugar issues Sleep apnea/sleep disorders Seizures
Referring Don’t rely on verbally passing on the referral question – provide a referral letter in addition Provide the context – what are the circumstance leading to the referral Make sure the assessor knows of any time constraints E. g. , report needed before school starts or a court date Tell the assessor what you hope to use the assessment results for The assessor may help identify other assessment needs It often allows the assessor to recognize it if you are asking for the wrong kind of testing, or asking the wrong professional When getting consent for the assessment, the assessor is required to disclose the purpose of the assessment
How speed the process and enhance the results Call ahead of time to ask if they do the requested kind of assessment and check what the timeline would be Get releases of information as soon as having scheduled the appointment Contact information sources and have them send relevant information Most facilities will (and should) only send their own documents and not forward documents received from other sources DCP only does the following assessments: Juvenile fire behavior risk assessments (as part of the Youth Fire Intervention Program) Any assessments ordered by Court Assessments on existing clients as a part of out treatment of the client
Consent Unless a court ordered assessment, consent is needed If has a guardian, consent can only be given by that guardian, or someone specifically designated by Court to have that right Placement of the child does not give the right to consent on client’s behalf Many clinics violate this (for both assessment and therapy) The consent has to be an “informed consent. ” The clinician needs to have a conversation with the person about client rights and about what the assessment will include. A consent to therapy does not mean that a consent has been given for psychological assessment and vice versa
Court Ordered vs. Voluntary/Referred
Court Ordered Should be ordered prior to disposition (i. e. , it is completed to aid the sides in forming their dispositions) The written order contains: Specified person to be assessed Specified kind and content of assessment (e. g. , psychological, competency, parenting competency) – making sure to include everything that is wanted (e. g. , recommendations) Specified provider (or clinic)
Court Ordered Court is the identified client The assessor represents the Court The psychologist-client privilege is not held by the assessment subject, but is held by the court instead The psychologist can, will, and should, share all relevant information with the court. The psychologist can only share information with others with the Court’s permission, including the assessment subject’s future providers (smart psychologists will include in the assessment report’s recommendation that the report should be shared with future treatment providers) The court owns the report and may insist on involved attorneys coming to the courthouse to read it
Court Ordered If the assessor witnesses in Court, the only loyalties are 1) truth/scientific standards and 2) the interests of the Court Refusal or inability to complete the assessment is reported to the Court Assessment subject usually technically has the right to have an attorney present – which may make the assessment impossible Assessor can never have the assessment subject as a client – past, present, or future
Court Ordered - examples Forensic Assessments (see later) Parenting competency and what would be needed to get the person to become a competent parent Treatment needs “Please help us understand what the heck is going on with this person”
The pseudo-Court-ordered work-around (please avoid!) Court may order a person to go out and get assessed (or may order the person to follow the recommendations of someone else who recommends an assessment) The assessment subject is now the client The client can now deny any information being shared with the Court The client can shop around and choose to only disclose the assessment conclusions that the client liked best If subpoenaed, the assessor now has a responsibility to be an advocate for their client’s best interest (without committing perjury)
Voluntary/referral Doctor-patient confidentiality applies as per the assessor’s profession (e. g. , as that of a therapist) As with any medical/mental health service, the client’s consent is needed Any guardian must consent PLEASE NOTE: Physical custody does not give right to sign for mental health services or assessment. It has to be full guardianship or a Court order that specifically spells out right to consent to mental health services Consent for therapy or psychiatric management does not imply consent for assessment except as intimately linked to therapy process (e. g. , psychosocial intake assessment) A separate consent should be obtained for additional assessment work (a frequently violated ethical principles)
Types of Assessments
Alcohol and Other Drug Assessment Conducted by a licensed alcohol and drug counselor Usually not trained in mental health counseling Only a few psychotherapists or clinicians are licensed or trained as such The assessor has to rely on the information provided Other sources are invaluable and usually appreciated Others’ factual observations Past records Who/where previously treated
Psychiatric Assessment “Psychiatric assessment” is vague – so best to be more specific Psychiatrists typically do not have the required training to administer and interpret most psychological tests (including personality tests and IQ tests) Will usually involve: Seen by a psychiatrist (primarily trained as a medical doctor, but with a specialization in psychiatry) A brief interview (between 15 -60 minutes) Might include some review of past records
Psychiatric Assessment continued Will usually result in: An opinion regarding diagnoses that appear to fit A brief 1 -page report Recommendations regarding best medication management May provide recommendations for other treatment modalities Don’t obsess about the exact diagnosis. Many psychiatrists will not spend the extra time and intrusion into the client’s privacy to get the diagnosis exactly right if it would does not change the medications prescribed
Sample psychiatric assessment referral RE: Tony Stark (DOB 01/15/2002) Dear Dr. Strange, Please accept this referral for a psychiatric assessment. I am making this referral in my capacity as the adolescent’s supervising social worker (DSS). A signed release of information is enclosed. Tony is a resident at the County’s group home for adolescents. He has been having increasing behavioral issues over the last year and is becoming easily overwhelmed and overstimulated. He has been refusing to go to school due to the crowded rooms and hallways and at the group home is refusing to attend groups. There is a family history of significant mental illness. We are seeking this psychiatric assessment to assess for the potential presence of mental illness and for potential medication management to allow him to continue his education and return to therapeutic and skills-building activities.
Neurological Assessment Conducted by a medical doctor (neurologist) or a nurse with specific training for it This assessment targets physical trauma and biological and structural abnormalities Initial screenings for neurological concerns is sometimes done by a general practitioners with extra training (e. g. , screening for concussions) Emergency Rooms may do screenings, but usually emphasize acute stabilization. If any suspected head trauma or other neurological issues, a follow-up with a the primary care physician or neurologist is recommended
Neuropsychological Assessment with a psychologist specialized in neuropsychology Targets identifying specific malfunctions in how the brain is operating Testing is usually extensive Focus on identifying specific areas of abnormal vs. normal functioning (i. e. , “pass” (normal) vs. “fail” (an anomaly is going on) Less focus on where someone fits on a continuum
Sample neuropsychology referral RE: Bruce Hulk (DOB: 11/03/1978) Dear Dr. Banner, Please accept this referral of Bruce Hulk for a neuropsychological assessment. I am making this referral in my capacity as his care coordinator. A signed release of information is enclosed. Bruce is a 39 years old male who has been in a protected work placement at Stream Industries since an aneurism when he was 25 years old. His job involves completing simple repetitive tasks that may change every few weeks when we have a new customer. While he does some of the jobs fast and perfectly, he makes frequent mistakes on other tasks, appearing to have some processing difficulties with these latter tasks. When this occurs, he often has sudden spurts of anger. We seek a neuropsychological assessment to better predict the tasks he may and may not be able to do so as to be able to maintain his employment.
“Diagnosis” Assessment A request for an assessment to get a diagnosis Be aware that many specialty clinics/specialist psychologists have biases Usually not very useful except to qualify for programs/funding sources Instead, ask for such things as: etiology (cause), contributors to the problem, nature of the problem, treatment recommendations Avoid limiting the diagnostic question (e. g. , don’t ask “does he have ADHD? ”)
Differential Diagnosis Asks the psychologist to determine what diagnosis fits best. Example: I am referring Oliver Queen for a differential diagnosis for bipolar disorder vs. ADHD. – This asks the psychologist to determine whether Oliver is best understood, treated, and offered services, as if he has bipolar disorder or ADHD. Can be asked as a part of a wider assessment
Rule Out A Rule Out assessment is used when there is not much evidence of a specific mental health or cognitive issue, but that it would be important to catch it if it actually is there Example: Ms. Snow is 17 years old and certain changes has been seen over the last couple of years. She is now unfocused in school, she gets irritable easily and has been skipping school and staying home. There is a family history of schizophrenia. –Ms. Snow may be referred for an assessment to Rule Out schizophrenia to make sure this is not developing Usually requested as a part of a wider assessment
Sample referral for diagnosis RE: Clark Kent (02/13/2008) Dear Dr. Fate, Please accept this referral for an assessment for a differential diagnosis (i. e. , Bipolar vs. Autism vs. trauma/neglect). I am writing in my capacity as Clark’s DSS social-worker. We also seek recommendations for what level of care Clark may need and if placement with a foster-familt may be appropriate. A signed release of information is enclosed. We are trying to find the right services and foster-family for Clark, and are not sure of the nature of his real difficulties, but it is apparent that he has special needs. Past mental health providers have not agreed on a diagnosis, but all of them focused on treatment, and not diagnosis. The couple who raised Clark was an elderly farm-family who recently passed away. They were not his real parents. They found him alone in the field and chose to raise him instead of letting the authorities know. He has had limited contact with other children and appears to struggle to get along with others. He avoids eye-contact. He does not speak much and sometimes stutters. He does everything fast, appearing to not be able to sit still for long.
Forensic Assessments Sometimes conducted by a psychiatrist (if brief/limited in scope) Usually conducted by a forensic psychologist (psychologist with specialized forensic training) Forensic assessments are usually assessments that are specifically identified as such for various Court reasons The assessor collects and analyzes data, and may make recommendations and projections, but only Court makes determinations and decisions Risk assessments are forensic assessments. The research is based on past offenders, so risk can only be properly assessed for someone who already has already committed an offense
Forensic Assessment Examples Need for guardianship/competency Competency to stand trial Not guilty by reason of mental defect (NGRI) Examples of risk assessments Sex Offender: What is the risk of committing another sexual offense, and how to reduce that risk Violent Offender: What is the risk of committing another violent offense, and how to reduce that risk Juvenile Fire Behavior: Risk of future fire behaviors, and how to reduce that risk (provided by the Youth Fire Intervention Program/Dr. Klausen)
Cognitive Assessment Conducted by a psychologist Usually understood to mean an assessment of their intelligence (IQ) If not otherwise requested, may result in a brief assessment that only establishes an overall intellectual level and maybe Verbal vs. Visual/spatial intelligence Request an assessment of relative intellectual strengths and weaknesses for a more thorough assessment A cognitive assessment will not usually include testing of general memory unless specifically requested Cognitive assessments can provide much richer information if there has already been a past cognitive assessment and the psychologist can get those results Past academic and work history is often useful for the psychologist to have The same cognitive assessment can not be given twice within a short time-span. Make sure that the psychologist knows of any recent cognitive assessment so the psychologist can choose different cognitive tests
Sample cognitive assessment referral RE: Peter Parker (DOB: 05/35/1998) Dear Dr. Mid-Nite, Please accept this referral for a cognitive assessment. I am Mr. Parker’s mother. A signed release of information is enclosed. Mr. Parker always struggled to learn and makes a lot of poor choices. He is spending all his money on Magic The Gathering cards or gives the money away. I am concerned that he may not have the cognitive capacity to understand the world around him or take care of himself or his finances. I am making this referral to establish his intellectual level to see if we should request for Court to order an assessment for need for guardianship and disability. Alternatively, if he has any areas of relative intellectual strengths that may suggest employment options.
Memory Assessment Most cognitive assessments do not include a memory assessment unless specifically asked Memory assessments require a general cognitive assessment unless one has been done very recently Memory assessment results are interpreted in relation to overall cognitive abilities. If someone is found to have a memory of around 60, but an IQ around 60, then the person is not found to have specific memory problem, although the person has a very poor memory. The psychologist can regardless help the person’s support system have a better understanding of realistic expectations of the person’s memory.
Learning Disability/Disorder Public agencies and psychologists define learning disabilities differently. Public agencies (including schools) usually focus on how far behind a child must be before extra resources are provided (usually 2 years in Wisconsin). Psychologists focus on whethere is something in how the person processes information that prevents the person from learning as well as expected given their intelligence. Example: Logan is at the 99 th percentile for intelligence and 60 th percentile for how much he has learned. Absent a social reason (e. g. , missed a year of school) the psychologist will conclude that there is a learning problem. Before a learning disability assessment, it is good to make sure there have been recent hearing and vision tests. The assessment should include a thorough assessment of different forms of intelligence, and a standardized assessment of how much he has learned compared to others.
Sample Learning Disability Assessment Referral RE: Scott Summers (DOB: 04/38/2008) Dear Dr. Druid, Please accept this referral for a learning disability assessment. I am Mr. Summers’ primary teacher at Xavier’s School for Gifted Youngsters. A signed release of information is enclosed. We know that Mr. Summers is intelligent, but over the last year he has been unable to make any progress in his reading and reading frustrates him. Recently, he has started to struggle in math. He had an eye-exam last week and his eyesight is perfect when wearing his glasses. We seek a better understanding of what is causing his learning difficulties and how we best can help. His academic records have been gathered and will be forwarded as soon as this referral is accepted.
Personality Assessment Usually conducted by a psychologist Useful to help a client better understand themselves Useful for caregivers, providers, and other supports to make use of to better understand, predict, and help the individual Particularly useful if there have been a lot of failed services Provides an understanding of how the individual thinks, insecurities, interpersonal tendencies, motivations, behavioral tendencies, and other psychodynamic information This is usually the best form of assessment for generating specific recommendations for treatment, services, and adjustments in the person’s life
Sample Personality Assessment Referral RE: Logan Howlett (DOB: 05/18/2001) Dear Dr. Xavier, Please accept this referral for a personality assessment. I am writing in my capacity as Logan’s foster-care co-ordinator. A release of information is enclosed. Logan has been in several foster-home placements that have not worked out because he has had a hard time getting along with various foster-care family members and has episodes of rage. He has also been discharged from two therapists because he did not feel like therapists “got him” (an assessment therapists agreed with). Logan also agrees that he does not understand himself either. Logan really wants help and in general is a very loving boy. Any insight you can help us gain about how he works inside would we greatly appreciated, as well as any recommendations for how to make therapy and any future placement successful for him.
Understanding Assessment Results
Biased Assessment Tools Few established assessment tools are biased The bias is usually a matter of what it is used for Bathroom scale example For example, most IQ tests are predictive and largely unbiased for predicting success within mainstream academic and professional pursuits, as well as ability to navigate through typical bureaucracies and financial arrangements. They are biased if looking at predicting ability to excel at a musical instrument, and only relevant for some aspects of parenting. As long as a properly trained psychologist knows what the assessment results are being used for, the psychologist can make sure that the assessment tools are chosen and interpreted accordingly
What You Should Receive A feedback session should be offered where the assessor explains the results An assessment report containing: The referral question What tests were conducted Other sources of information (e. g. , what records were reviewed) Assessment results outlined test by test (e. g. , scores on the tests) This allows future psychologists to use the information Interpretations of the results Recommendations and implications as it relates to the referral question
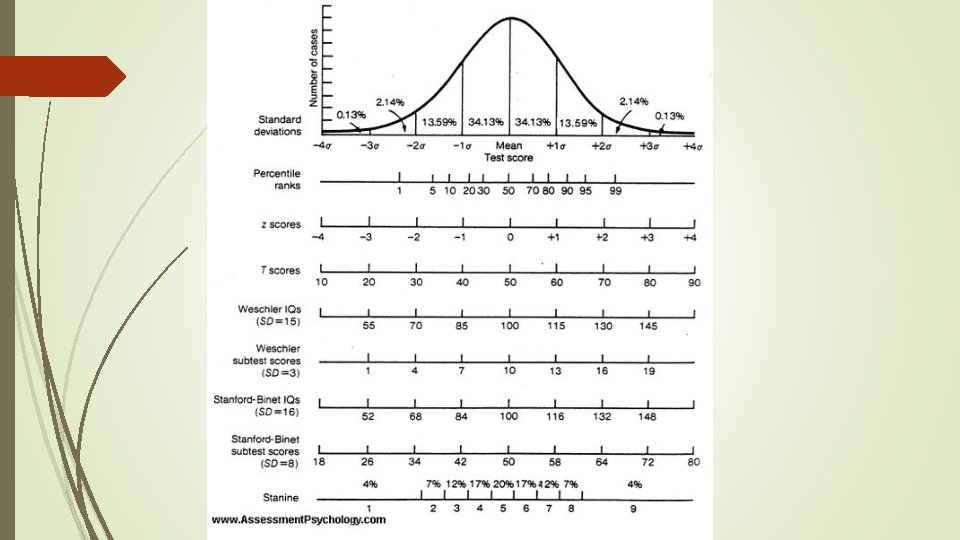
Statistics Percentile Rank: Easiest to use to get a quick idea. Tells how many percent of the population is at this level or less 12 th percentile for depressive symptoms = 12% of the population has this few depressive symptoms or less 95 th percentile for intelligence = 95 % of the population have an intelligence this high or less Standard Deviation (SD) – how far from the mean/norm. 68% are between +/- 1 SD (Average). 96% percent are between +/- 2 SD (Average + Above/Below Average) 2% are beyond this at either end (cognitive disability range or gifted). IQ: Mean = 100, SD = 15 T-Scores: Mean = 50, SD = 10 Assessment results (especially IQ) will often be given as a range (high certainty the measures ability or scale falls within that range)
About Intelligence Quotient Tests An IQ test is not one IQ test. Each IQ test consists of many IQ tests called subtests. Most IQ tests are about forms of intelligence relevant to success in mainstream academic and professional settings IQ does not tell intelligence compared to people in general IQ tells intelligence compared to people of the same age An 18 -year old with an IQ of 100 will be more intelligent than an 8 -year-old or 90 year old with an IQ of 115 IQ is VERY stable over time, assuming no radical changes in the person’s circumstances that are outside of what most people experience IQ is much more variable in young children
Intellectual Disability (Previously Mental Retardation) Intellectual disability diagnosis requires IQ below 70 (some use 65) – bottom 2% - often called intellectual disability range AND Deficits in self-care AND Started in first few years of life
Common IQ Scales Full Scale Invalid if big discrepancies between underlying subtests Verbal – ability to process and express data verbally Non-verbal/Performance/Perceptual/Visuo-Spatial - ability to process and express data non-verbally (e. g. , through pictures) Working Memory - how much information can hold and work on in consciousness at one time Processing Speed – how fast can process and make choices when making the right choice is easy Fluid Reasoning – ability to problem-solve in a novel situation
Interpreting Subtests Each IQ Scale is the result of collapsing the performance of two or more subtests Differences between the performance of different subtests can raise interesting hypotheses This is usually speculative Mostly has value if it fits other subtests (e. g. , did poorly on all the subtests across scales when they required using hands) AND Fits real-life data (e. g. , turns out that he also struggles to use scissors and tie shoe -laces and it is recognized that he may have issues with fine motor-skills)
Big Discrepancies Between IQ Scales Full Scale IQ is then invalid People often misjudge, overestimate, or underestimate the person Can lead to cognitively based personality styles Examples: High processing speed Limited working memory Higher verbal than perceptual
Common IQ Tests Wechsler’s Intelligence Scale for Children (WISC) 6 to 16 years old Verbal; Perceptual; Working Memory; Processing Speed Wechsler’s Adult Intelligence Scale (WAIS) 16 to 90 years old Verbal; Perceptual; Working Memory; Processing Speed Wechsler’s Abbreviated Scale of Intelligence (WASI) 6 to 90 years old Short version: IQ screen only Full version: Full Scale IQ with some idea of Verbal and Perceptual
Common IQ Tests continued Woodcock-Johnson Tests of Cognitive Abilities 2 years old to 90 years old Very thorough and wide range of abilities tested (7 subscales) Heavily supported by research Provides age equivalency data (e. g. , what age does this child function at intelligence-wise) Differential Abilities Scale (DAS) 2 years 6 months to 11 years 11 months Wide range of cognitive abilities, including some memory Peabody Picture Vocabulary Test Ages 2 to 90 years old Measures receptive verbal ability Minimizes effect of speech problems and reduces impact of language barrier Quick and relatively good predictor of scholastic aptitude Does not distinguish as well between Aptitude (i. e. , IQ and Achievement)
“Achievement” Testing Achievement testing is testing of how much a person has obtained of academic knowledge compared to same-age and same-grade peers Achievement reflects past ability to learn, and if there have been significant improvements in their life may not predict future learning Always done in conjunction with an IQ-test, unless there are recent IQ test results available This is usually a part of Learning Disability Testing Can help get an idea of the effects of the child’s past environment
Common Achievement Tests Wide Range Achievement Test (WRAT) 5 to 94 years old Can be done in groups Wechsler Individual Achievement Test (WIAT) 4 years to 50 years 11 months Woodcock-Johnson Tests of Achievement 2 to 90 years old Very thorough across a wide range of abilities
IQ vs. Achievement An “under-achiever” is someone whose IQ is much higher than their achievement level. Usually caused by one or more of the following: Learning disorder Mental health issues that have interfered with learning Environmental interference during previous years in school (e. g. , frequent moves) An “over-achiever” is someone whose IQ is much lower than their achievement level. Usually caused by one or more of the following: A particularly driven and persistent personality Environmental supports and motivators that pushes the person to learn more Brain-damage (IQ is affected much more than past learning)
IQ and Achievement IQ scores and Achievement scores are very useful for setting realistic expectations and maximize learning IQ predicts at what speed and depth of sophistication the person would best learn Achievement indicates at what grade-level (curriculum progression) the person would best be taught at Too low expectations: Slower learning Less accomplishment (e. g. , in a work setting) Loss of motivation and focus Too high expectations: No learning May give up on learning Development of an identity as a “failure”
Personality Inventories Used to get a better sense of the person’s internal and interpersonal dynamics Many questions (sometimes hundreds) answered by the client or in some cases by a caregiver Completed individually (e. g. , not conferring with others) Questions are selected through thorough empirical principals and extensive research Compares the individual to peers (age and usually gender) Each has multiple personality scales May focus on behavioral symptoms and/or internal traits Results given as T-scores (Mean = 50; SD = 10) The results must be interpreted by a psychologist who has gotten to know the client (existing therapist or someone who also did a clinical interview)
Common Personality Inventories Minnesota Multiphasic Personality Inventory-2 (MMPI-2) Minnesota Multiphasic Personality Inventory-Adolescent (MMPI-A) Millon Clinical Multiaxial Inventory-III (MCMI-III) The above three: Give a wide and deep picture of the persons personality, including insecurities, psychiatric symptomatology and interpersonal dynamics Built-in validity measures and hard to fool Child Behavior Checklist (CBCL or Achenbach) Behavioral Assessment System for Children (BASC) Above two focus on mood and behavioral issues in children Provide comparisons across multiple people completing them
Disorder-specific inventories The good ones are empirically based and well researched Rarely differentiates between the assumed cause and other potential reasons for the symptoms They are only appropriate to get an idea of concern’s severity They are not appropriate to be used for deciding what the issue is Example: If a girl has really high anxiety, then an ADHD inventory will most likely find high levels of ADHD without the girl having ADHD
Some Common Disorder-Specific Rating Scales Connor’s Rating Scale Beck Depression Inventory (BDI) Beck Anxiety Inventory (BAI) UCLA PTSD Index (UCLA)
Projective Testing No right or wrong answer Open questions or requests “What do you see in this picture? ” Can you draw your family for me? Looks at trends across responses more than individual responses Should never be the sole basis for any conclusions Great for getting a sense of what ways a person processes and thinks Provides hypotheses to explore with further interview or testing Can provide specific illustrations of what has been more robustly identified by other tests Good at detecting psychosis that the person is keeping hidden
Examples of Common Projective Tests Draw a person/family/tree Incomplete Sentences Thematic Apperception Test Roberts Apperception Test Rorschach If it says that uses Exner, then based on norms and data If not, it is based on clinician interpretation
Jargon Client “denied” – this just means that the client said “no” to something they were asked. It does not imply that the client was hiding something R/O or Rule Out If before a diagnosis in a list of diagnoses: “The following diagnosis may fit, but it could not be confirmed or ruled out at this time” Otherwise, it expresses the intent or request to double-check whether or not it is there
Jargon Continued X “secondary to” Y – X is there, but is there because of Y. Example: Clark has significant ADHD symptomatology secondary to Autism (e. g. , Clark was not so unlucky to randomly be born with both, but was born with Autism, which also brought with it attention difficulties) By history Added after a diagnosis (e. g. , Bipolar I Disorder, by history) Means that it was diagnosed by a previous clinician The present clinician trusts this diagnosis, without having personally established that the criteria for it have been met
Common Mistakes Uncommon among well-trained psychologists
Just because a diagnosis was provided does not mean it was thorough If you specifically and clearly point out that a thorough diagnosis is needed, then you should be getting that If the referral was about something else (e. g. , cognitive assessment): The diagnosis is likely to be an afterthought Might only provide the diagnoses directly relevant to the referral question (e. g. , learning disorder or dementia) even if other mental health issues are present
Diagnosis accumulation A mental health diagnosis is usually meant to replace previous diagnoses Assessors are often poor at making this clear Instead, clients and their supports tend to just add diagnoses Example: Kara was diagnosed with Attention-Deficit/Hyperactivity Disorder at 10. Soon, her therapist recognized that focusing problems were due to anxiety, and she diagnosed Generalized Anxiety Disorder. Later, Kara opens up about her parents dying in an inferno while she narrowly escaped, her foster-sister jealously tormenting her, and the foster-parents severely restricting her activities. Her only living relative (Clark) was missing. The therapist realized that Kara’s anxiety is specific to triggers relating to her trauma, and she was diagnosed with PTSD. Kara has a diagnosis of only PTSD - not ADHD/GAD/PTSD.
Diagnosis – “…and the kitchen sink” Occam’s Razor applies A clinician should give the fewest diagnoses necessary to capture the client’s difficulties Many mental health professionals give a list of all the diagnoses the client meets the criteria for
Not looking for alternate explanations This is most commonly a problem in a brief assessment This is rarely a problem if conducted by a psychologist Almost all diagnoses include a criteria of “not better explained by…” Diagnosis-specific rating scales worsen this
Forgetting about functional impairment One of the criteria for almost all diagnoses is: “…causes marked distress in the individual or impairment in occupational, interpersonal or other important area of functioning”
Misuse of Assessment Printouts Some assessment tools will provide a computer printout (e. g. , CBCL) and even computer generated interpretations (e. g. , MMPI-2, MMPI-A) Special circumstances can greatly distort the computer generated results These printouts must be interpreted by a mental health worker who knows the case and has specific and thorough training in assessments (e. g. , psychologist, school psychologist, or masters level psychometricians – it is very rare for a psychiatrist to have the appropriate training) The printout should usually not be released, just the report generated by the clinician. If the printout is released, it has to be released with the report. The exception is when released to another clinician with appropriate training and knowledge of the case
Questions?