Revision arthroplasty around the hip and the knee


































 THR")
















- Slides: 57
Revision arthroplasty around the hip and the knee Small group discussion 2 Hip and knee cases Periprosthetic Fracture Management Curriculum events 2020
Learning objectives for the cases • • Classify the fracture Describe the options and indications for nonoperative, fixation, and revision treatment Select an appropriate treatment Identify and address potential complications
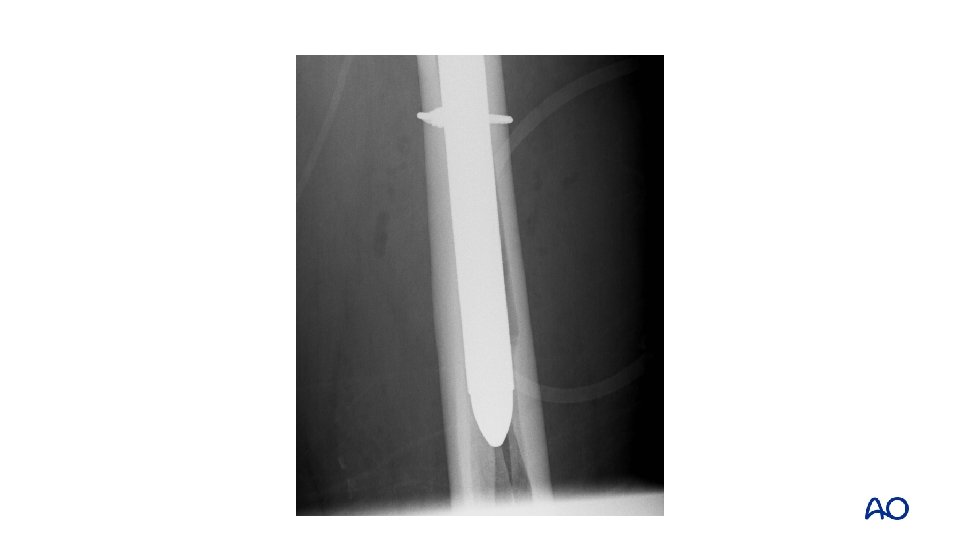
Case 1: Case description • • 78 -year-old Cementless total hip replacement 6 weeks ago Fell at home Severe pain—was unable to get it up
Case 1 • • Describe the implant and the fracture Classify
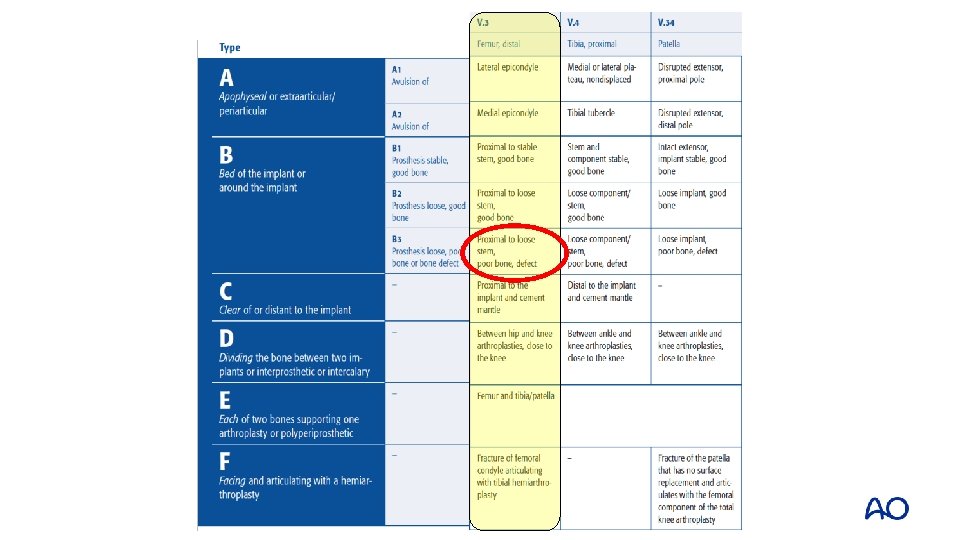
Case 1 • • Cup is well fixed Stem is loose Fracture extends into greater trochanter (B 2) Distal diaphysis intact
Case 1 • Describe strategy of treatment step by step
Case 1 • • • Remove stem Prepare distal femur Insert trial stem Insert stem Reduce fracture Definitive fixation
Case 1 • Monoblock stem • Hook plate
Case 2 • • • 86 -year old woman Elective THR 29 years ago Pain left hip for than 10 years Slips and fell Clinically intact soft tissue with no signs of infection • Slight elevate ESR (25 mm), normal CRP
Fracturepatternfx fxof ofshaftfixationand anddesign Case 62 months post # fixation Case 10 5 4 2 ?
Fracturepatternfx fxof ofshaftfixationand anddesign Case 2 Fracture Case 10 5 4 2 Postop
Fracturepatternfx fxof ofshaftfixationand anddesign Case 2 Fracture Case 10 5 4 2 Postop 2 years
Case 2: Take-home messages • • • Remove all the cement Complex fracture can heal (bone formation) Be ready to revise the cup when necessary
Case 3: Case description • • 82 -year-old man Left side: treated for recurrent dislocation (constrained liner) after femoral and acetabular revision
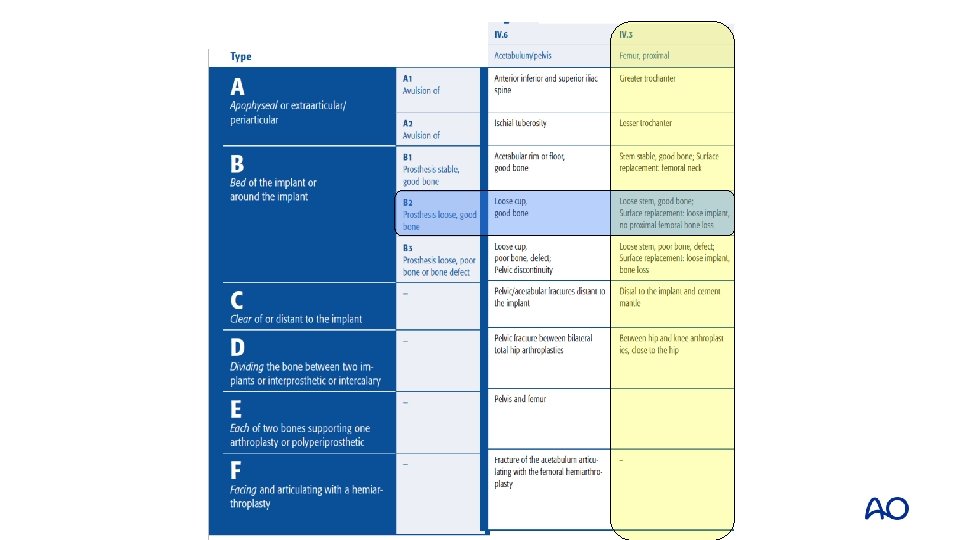
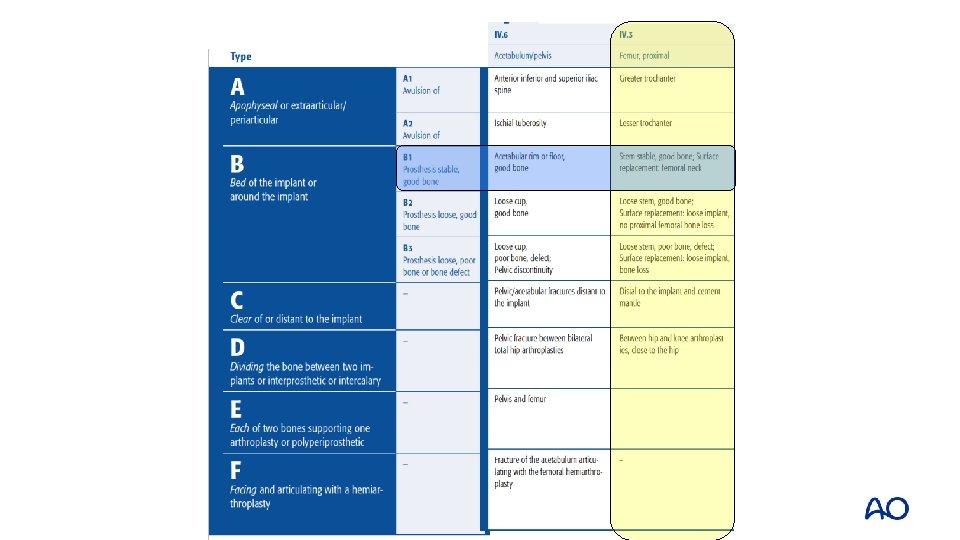
Case 3 • Right side: 20 years after Met-PE • Fracture of the greater trochanter and pelvis, no trauma (UCS 6/3 IV. E) • Options?
Case 3 • • Reaming the liner and cementing a polyethylene cup and 32 mm metallic head Bone graft through a window, fixation of greater trochanter
Case 3 • Rapid recovery, no pain
Case 3: Take-home messages • • • Be careful with complications in older population Avoid major surgery if not necessary Improve tribology and materials according to functional requests of the patient
Case 4: Case description • • • 75 -year-old man BMI 30, normal health status, no medication, farmer Knee arthroplasty 17 years ago Revision 3 years ago: aseptic loosening, satisfied 1 year postop Car accident 3 months ago (no doctor’s visit) Walked with crutches, now visits outpatient clinic
Case 4
Case 4 • • • Lab: normal; ESR/CRP Negative aspiration Plain x-rays and CT: • Loosening tibial component • Possibly also femoral component • Significant bone loss tibial side • Fracture classification?
Management options • • • Nonoperative until fracture healing? Revision TKA? Treatment of the femoral periprosthetic fracture 3 months after trauma Reduction of fracture possible? Treatment of bone loss on tibial side Other considerations?
Surgery • • Removal of prosthesis, standard approach Tibia: Fluoroscopy controlled intramedullary preparation, bone impaction and trabecular metal (TM) cone reconstruction (bone loss epiphysis/metaphysis)
Surgery • • • Fracture is partially healed. Flexion position at fracture accepted, but bypassed with longer uncemented stem Bone impaction grafting and trabecular metal cone reconstruction of distal femur and intramedullary canal Hinged revision total knee arthroplasty (TKA) implant used
Case 4
Case 4: 6 weeks postop • • No pain Function 120/0/0
Case 4: Take-home messages • • Fractures can be stabilized or excised during revision surgery Biology needs to be respected if strong, durable fixation is to be achieved
Case 5: Case description • • 64 -year-old woman Medial cementless unicompartmental replacement Always severe pain with weight bearing since operation Presents at two months with worsening varus deformity
Postop
8 weeks postop
Case 5 • • • What went wrong? Why the fracture? How to treat?
Management options • Tibial component is ingrown to proximal tibia fragment • ORIF vs revision total knee replacement (TKR)?
Proximal tibial allograft
Case 5: Take-home messages • • Periprosthetic fractures require consideration of both the bony injury and the loose prosthesis Revision to a TKA offers a durable solution
Case 6 • • • 39 -year-old with severe juvenile rheumatoid arthritis (JRA) THR and revision THR many years prior, no issues Revision TKR 4 years prior Minor fall Severe pain left knee
Case 6
Case 6 • What is going on?
Case 6: Postop
Case 6: Postop
Case 6: Take-home messages • • Composite structural bone graft/prosthetic replacement solutions are an option in cases where the native bone stock is severely depleted Consider tumor prosthesis with diaphyseal replacement as an alternative
Case 7: Case description • • 71 -year-old man Elective THR Ready for discharge home on day 2 Slips and falls on the ward
Case 7: Case description • • 71 -year-old man Elective THR Ready for discharge home on day 2 Slips and falls on the ward
Case 7 • • • Proximal fracture through calcar and greater trochanter Uncemented stem with loss of fixation Vancouver B 2
Case 7 • • Fully coated long, straight stem Failure to ream full length of cylindrical stem
Case 7 • • Vancouver B 1 Fix without revision
Case 7 • • Healed at 6 months Persistent limp
Case 7: Take-home messages • Be careful with aggressive “designs” and implanting tools