RENAL Diseases Investigation of renal system Haematuria PSGN




. • 2")
 • 1 - Hemoglobinuria. (")
. • 1 - Drugs • 2 -")







 H/O")





 • Renal involvement occurs in 25– 50% of children")
 Alport")
 • Glomerulonephritis with Ig. A as the predominant immunoglobulin in")
 • Treatment: supportive • Prognosis: mainly good, only 30% has")
. • Haematuria + proteinuria + sensorineural hearing")



 GLOMERULONEPHRITIS • Chronic glomerulonephritis that frequently leads to glomerular destruction and end-stage")
 GLOMERULONEPHRITIS • Nephritis with rapid progression to end-stage renal failure •")

 •")


![Urine Analysis Prerenal. • Urine osmolality exceeds 500 m. Osm/kg [mmol/l] H 2 O.](https://slidetodoc.com/presentation_image_h/8942b737f9c0ae5458c399096cbcfca1/image-40.jpg "Urine Analysis Prerenal. • Urine osmolality exceeds 500 m. Osm/kg [mmol/l] H 2 O.")

. • Hypertension: – The primary")

- Slides: 44
RENAL Diseases • Investigation of renal system • Haematuria/ PSGN • ARF/CRF • Proteinuria/ Nephrotic syndrome • UTI • Congenital Anomalies
HEMATURIA • Hematuria is one of the most common urinary findings that bring children to the attention of the pediatric nephrologist. • Generally, hematuria is defined as the presence of 5 or more red blood cells (RBCs) per high-power field in fresh centrifuged speciment.
• Hematuria: can be gross “Macroscopic” (ie, the urine is overtly bloody, smoky, or tea colored) or microscopic. It may be symptomatic or asymptomatic, transient or persistent, and either isolated or associated with proteinuria and other urinary abnormalities.
• The role of the primary care physician in the management of a child with hematuria includes the following: • Recognize and confirm the finding of hematuria. • Identify common etiologies. • Select patients who have significant urinary system disease that might require further expertise in either diagnosis or management and referral.
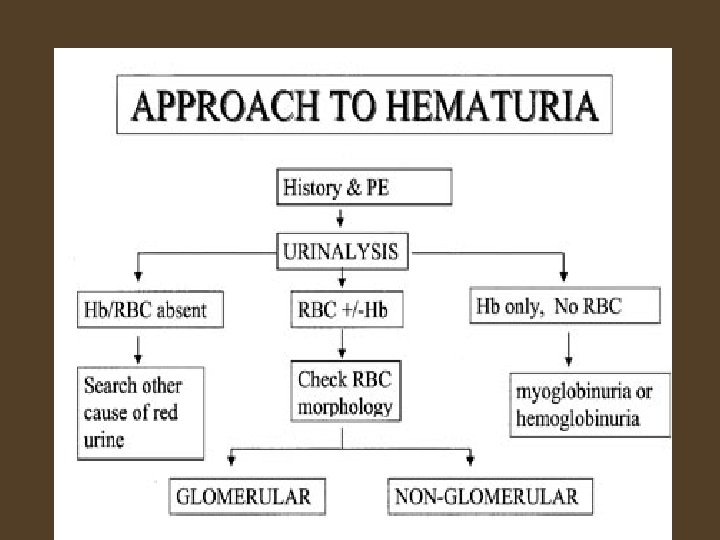
Causes of RED urine • 1 - Heme-negative (no RBC or Hb). • 2 - Heme-positive ( Hb + no RBC). • 3 - True Hematuria ( RBC +- Hb).
Causes of Heme-positive ( no RBC but positive Hb) • 1 - Hemoglobinuria. ( As in Hemolytic Anemia) • 2 - Myoglobinuria: (Resulting from muscle injury or secondary to viral infection, cruch injury, or DIC)
Causes of Heme-negative (no RBC or Hb). • 1 - Drugs • 2 - Dyes • 3 - Metabolites.
Red urine without RBCs
Causes of True Hematuria: • 1 - Glomerular hematuria : • Thin basement membrane disease (benign familial hematuria) • Alport syndrome • Ig. A nephropathy • Hemolytic uremic syndrome • Postinfectious glomerulonephritis • Membranoproliferative glomerulonephritis • Lupus nephritis • Anaphylactoid purpura (Henoch-Schönlein purpura).
• 2 - Nonglomerular hematuria: • • • • Fever Strenuous exercise Mechanical trauma (masturbation) Menstruation Foreign bodies Urinary tract infection Hypercalciuria/urolithiasis Sickle cell disease/trait Coagulopathy Tumors Drugs/toxins (NSAIDs, anticoagulants, cyclophosphamide, ritonavir, indinavir) Anatomic abnormalities (hydronephrosis, polycystic kidney disease, vascular malformations) Hyperuricosuria
APPROACH TO HEMATURIA. HISTORY: clots in urine ? Extraglomerular causes fever, abdominal pain, dysuria, frequency, and recent enuresis in older children (? UTI). recent trauma to the abdomen ? Hydronephrosis early-morning periorbital puffiness, weight gain, oliguria, the presence of dark-colored urine, and the presence of edema or hypertension (? Glomerular causes) Is painless (? Glomerular causes) Recent throat or skin infection (? Postinfection glomerulonephritis). Joint pains, skin rashes, and prolonged fever in adolescents (? Coollagen Vascular Disorders). Skin rashes and arthritis (? Henoch Schonelein Purpura or SLE). exercise, menstruation, recent bladder catheterization, intake of certain drugs or toxic substances, or passage of a calculus Family history (? Inherited or Familial Renal diseases).
• Investigation: – Studies performed in all patients: • • urine microscopy and culture CBC serum creatinine serum C 3 level US kidneys urine protein = urine albumin/creatinine ratio calcium = urine calcium/creatinine ratio
– Studies performed in selected patients: • • Dnase B titer or streptozyme < 6 months duration Skin or throat culture ANA titer Urine analysis looking for cast Coagulation study/ platelet count Sickle cell screen Audiogram – Renal biopsy • Microscopic haematuria plus any of the following: – Diminished renal function – Proteinuria • Persistant microscopic haematuria (>1 year) • Second episode of gross haematuria – Cystoscopy • Pink o microscopic haematuria, dysuria and sterile urine culture
Glomerular: brownish or colacoloured and may contain RBCs cast, proteinuria Lower urinary tract: red to pink color urine and may contain clots
• • 7 years old boy Frank haematuria (smokey or tea colored) H/O throat infection 2 weeks ago O/E peri-orbital edema, BP 140/90 (hypertension) – What is the most likely diagnosis – What investigations
Post-streptococcal glomerulonephritis: • Rare before the age of 3 years • Nephritic picture: Gross haematuria, edema , hypertension, renal insufficiency (normal RF-ARF) • Complications of hypertension: encephalopathy, congestive heart failure • Rarely: nephritic- nephrotic picture.
Diagnosis: • Urine analysis: RBCs, RBCs cast, proteinuria • Low complement C 3 • Evidence of streptococcal infection: throat culture, ASO titer and DNase B antigen and streptozyme test • Mild normochromic anaemia • Renal function
Complications: ARF volume overload, hypertension, fits, hyperkalemia, hyperphosphatemia, hypocalcaemia and acidosis Treatment • Antibiotics • Management of ARF • Treat Hypertension.
Prognosis • Complete recovery 95% • Infrequently: severe acute phase leading to chronic renal insufficiency • Recurrence are extremely rare.
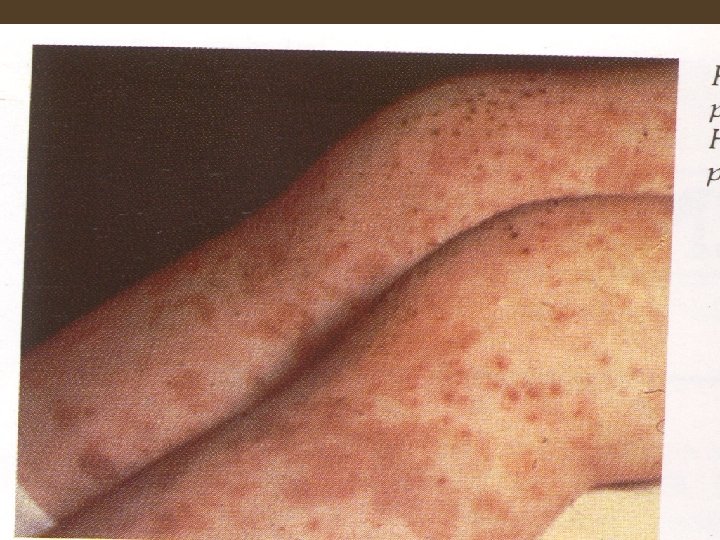
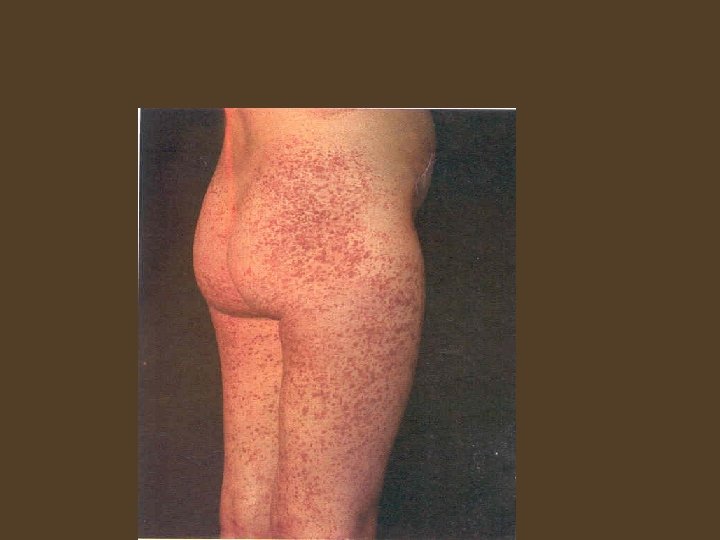
Case History: • 5 years old boy • Generalized malaise, abdominal pain, joints pain, peri orbital oedoma, skin rash (as seen in the picture). • He presented with Hematuria. • What is the most likely diagnosis?
Henoch-Schönlein Purpura or (Anaphylactoid Purpura) • Renal involvement occurs in 25– 50% of children during the acute phase • Haematuria with or without casts or proteinuria during the first few weeks of illness • The nephrotic syndrome, moderate azotemia, hypertension, oliguria, and hypertensive encephalopathy may occasionally occur. • Most children with renal involvement recover
Recurrent Gross Haematuria or Persistent Microscopic Haematuria • • Ig. A nephropathy (Berger) Alport syndrome Familial idiopathic haematuria Idiopathic hypercalciuria.
Ig. A Nephropathy (Berger) • Glomerulonephritis with Ig. A as the predominant immunoglobulin in mesangial deposits, in the absence of any systemic disease • Haematuria + minimal proteinuria • Normal C 3 + usually normal RF • Diagnosis: renal biopsy
Ig. A Nephropathy (Berger) • Treatment: supportive • Prognosis: mainly good, only 30% has progressive disease: hypertension, diminished renal function, or proteinuria exceeding 1 g/24 hr between episodes of gross hematuria
ALPORT Syndrome. • Hereditary nephritis. (85%X-linked, AR&AD). • Haematuria + proteinuria + sensorineural hearing loss (minority) + eye abnormalitie (10%) Corneal erosione. • Diagnosis: renal biopsy. • Males with Alport syndrome commonly develop endstage renal failure in the 2 nd or 3 rd decade of life, occasionally in association with hearing loss. Females usually have a normal life span and only subclinical hearing loss.
Idiopathic Familial Benign Haematuria • • No proteinuria All investigations normal Urine test of the parents and siblings An excellent prognosis, but long-term follow-up is required to exclude Alport syndrome
Idiopathic Hypercalciuria • This entity may be inherited as AD, and may present with recurrent gross hematuria or persistent microscopic hematuria, or dysuria in the absence of stone formation, or sandy urine. • Hypercalciuria (without hypercalcemia) • Diagnosis: 24 -hr urinary calcium excretion exceeding 4 mg/kg, urine calcium to creatinine ratio (mg/mg)>0. 2 • Hypercalciuria may lead to nephrolithiasis • RX: Oral thiazide & decrease Ca intake.
Membranous Glomerulopathy • Uncommon in childhood and a rare cause of haematuria. • The most common cause of nephrotic syndrome in adults. • Associated with systemic lupus erythematosus, cancer, gold or penicillamine therapy, and syphilis and hepatitis B virus infections. • Diagnosis: Renal biopsy.
MEMBRANOPROLIFERATIVE (MESANGIOCAPILLARY) GLOMERULONEPHRITIS • Chronic glomerulonephritis that frequently leads to glomerular destruction and end-stage renal failure. • Most common in the second decade of life. • Presentation: nephrotic syndrome, gross hematuria or asymptomatic microscopic hematuria, proteinuria and hypertension. renal function may be normal to depressed. Low C 3 complement level. • Diagnosis by renal biopsy.
RAPIDLY PROGRESSIVE (CRESCENTIC) GLOMERULONEPHRITIS • Nephritis with rapid progression to end-stage renal failure • Causes: poststreptococcal, lupus, membranoproliferative, the glomerulonephritides of Goodpasture disease, anaphylactoid purpura, and other forms of vasculitis • Acute renal failure, often after an acute nephritic or nephrotic episode • Diagnosis: Renal biopsy • Paediatric Nephrology Emergency
Acute Renal Failure • Develops when renal function is diminished to the point at which body fluid homeostasis can no longer be maintained. • Oliguria (daily urine volume less than 400 ml/m 2) is common, the urine volume may approximate normal. • Nonoliguric renal failure: in certain types of acute renal failure (aminoglycoside nephrotoxicity).
Etiology • Prerenal causes – Hypovolemia, hypotension, hypoxia (dehydration, Hemorrhage, Sepsis, H. F) • Renal causes – – – – Acute tubular necrosis Acute interstitial nephritis Glomerulonephritis Localized intravascular coagulation Tumors Developmental abnormalities Hereditary nephritis • Postrenal causes – Obstructive uropathy, stone, blood clot.
CLINICAL MANIFESTATIONS OF ACUTE RENAL FAILURE • Diminished urine output • Oedema (salt and water overload) • Hypertension, vomiting, and lethargy (uremic encephalopathy). • Complications of acute renal failure: volume overload with congestive heart failure and pulmonary edema, arrhythmias, gastrointestinal bleeding due to stress ulcers or gastritis, seizures, coma, and behavioral change Life threatening: GIT bleed, pericarditis and encephalopathy
Diagnosis • Careful history • Examination • Investigation: CBC, urea and electrolytes, PO 4, Ca, blood gases, C 3, US kidneys, urine electrolytes ( Na and creatinine), fractional excretion of Na (less than 1% in hypovalaemia) (FENa= (UNa x PCr/PNax. UCr) X 100).
Urine Analysis Prerenal. • Urine osmolality exceeds 500 m. Osm/kg [mmol/l] H 2 O. • Sodium content is usually less than 20 m. Eq/l (mmol/l). • The fractional excretion of sodium (urine Na x plasma Cr divided by the plasma Na x urine creatinine concentration X 100) is usually less than 1%. Renal • osmolality less than 350 m. Osm/kg [mmol/l] H 2 O • Usually exceeds 40 m. Eq/l (mmol/l) • Usually exceeds 1%
Treatment • Pre-renal=Hypovolemia: volume replacement may be critical • Renal: – Fluid restriction: input= output + 400 ml/m 2/24 hr (insensible losses) – Hyperkalemia: no potassium-containing fluid, foods, or medications until adequate renal function is reestablished • > 7 m. Eq/L (mmol/L): Nebulised salbutamul, IV Calcium gluconate, sodium bicarbonate, ca resonium, glucose and insulin – Moderate acidosis is common in renal failure: Na bicarbonate
Treatment • Hypocalcemia and hyperphosphataemia: Ca binders (Ca carbonate). • Hypertension: – The primary disease process (nifedipine, diazoxide, sodium nitroprusside or labetalol as a continuous intravenous infusion is indicated for hypertensive crises). – Expansion of the extracellular fluid volume (salt and water restriction is critical). • Indications for dialysis: fluid overload, and congestive heart failure, electrolyte abnormalities (especially hyperkalemia), central nervous system disturbances, hypertension.
Prognosis • In general, recovery of function is likely following renal failure resulting from prerenal causes, the hemolytic-uremic syndrome, acute tubular necrosis, acute interstitial nephritis, or uric acid nephropathy. • On the other hand, recovery of renal function is unusual when renal failure results from most types of rapidly progressive glomerulonephritis, bilateral renal vein thrombosis, or bilateral cortical necrosis.