Parvovirus Dr ChiYoung Wang l l l The








")











- Slides: 21
Parvovirus Dr. Chi-Young Wang
l l l The strict age dependent; 100% mortality under 1 o days of age but negligible in 4 -5 wks old. In 2 -3 wks, mortality below 10%. Old goose no symptoms. Especially for geese and Muscovy ducks. Vaccination of breeding stock has reduced the impact significantly.
Susceptibility to Chemical and Physical Agent l Very resistant. l Stable at p. H 3. 0 for 1 hour at 37 ℃. l No loss of titers at 56 ℃ for 30 min.
Laboratory Host System 1. 2. 3. 4. Muscovy duck parvovirus is different from goose parvovirus. Embryonated goose or Muscovy duck eggs. Primary cells from these eggs. An embryonic goose fibroblast cell lines (CGBQ).
Mode of transmission 1. Excrete virus in feces and spread by direct and indirect contact (eat contaminated feed and water). 2. Vertical transmission (Egg transmission). 3. Old geese as carriers. 4. No biological vector
Clinical signs (3 -5 days for day-old; 5 -10 days for 2 -3 weekold) 1. Rapid with anorexia, prostration, and death occurs within 2 -5 days: under 1 wk. 2. Older birds with maternal antibodyprotracted course. 3. Acute: anorexia, polydipsia, weakness, reluctant to move, nasal and ocular discharge, headshaking, and profuse white diarrhea, psedudomembrane covering tongue and oral cavity. Red swollen were founded in uropygial glands and eyelids.
Clinical signs 4. 5. 6. Prolong disease: growth retardation, loss of down around the back and neck, ascites. Penguin-like posture. Poor management and secondary bacterial, fungal, or viral infections may influence the final mortality levels.
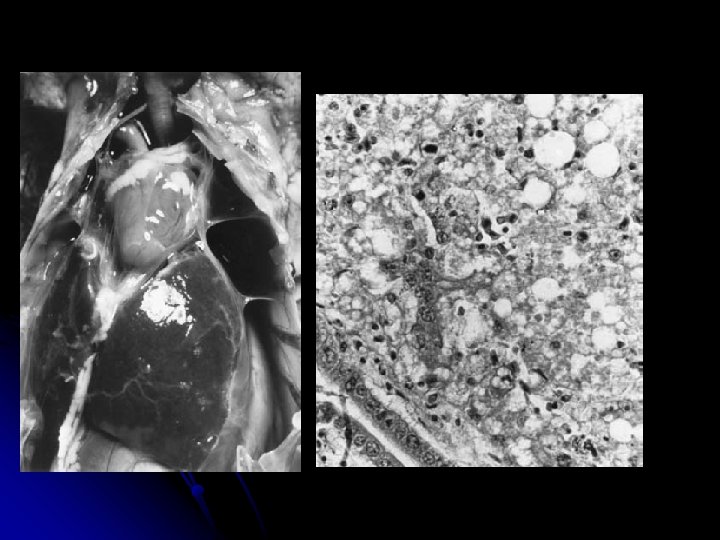
Gross lesions 1. 2. 3. Acute: pale myocardium rounded at its apex. Liver, spleen, and pancreas are swollen and congested. A sero-fibrinous pericarditis, perihepatitis with straw-colored fluid in the abdomen, and hemorrhages in thigh and pectoral muscle (less frequent).
Gross lesions 4. Pulmonary edema, liver dystrophy, and catarrhal enteritis. 5. Diptheritic and ulcerative lesions in the mouth, pharynx, and esophagus.
Microscopic lesions 1. 2. 3. 4. Degenerative changes in myocardial cells with loss of striation and fatty infiltration. The same changes in intestinal and smooth muscle cells. Degeneration of hepatocytes with vacuolation and fatty infiltration. Small, eosinophilic inclusion-like bodies were seen in cytoplasm of vacuolated hepatocytes. Shrunken and necrotic acinar cells of pancrease.
Immunity 1. Virus replication occurs in the intestinal wall and enters the blood stream. Virus reaches the liver and heart, where the most severe pathological changes occur.
Immunity 2. Adult breeders transferred maternal antibody through egg yolks. A relatively high level of acquired antibody persists about 2 week of age. 3. Initial production of Ig. M and Ig. G. Viral neutralization (VN) tests or AGP was used to measure antibody up to 80 months.
Diagnosis 1. Immunofluorescence or immunoperoxidase assay. 2. Agar gel diffusion technique of the allantoic fluid. 3. Inoculation of 10 -15 day old embryonated geese or Muscovy duck eggs via the allantoic cavity. Embryo mortality occurs 5 -10 days with hemorrhages and ochre-colored livers.
Diagnosis 4. PCR for VP 1 and 2 genes. 5. VN test in embryos or primary cell cultures and titer>1/16 considered positive. 6. Inoculation of cultures before they reach confluency. Syncytium formation and intranuclear inclusions are present in infected cells.
Diagnosis 7. Electron microscopy. 8. ELISA or a blocking ELISA. 9. A plaque reduction assay. 10. Differential diagnosis: DVE (herpesvirus) with high mortality in geese and ducks of all ages.
Intervention 1. Only egg from parvovirus-free flocks were put together and good hatchery hygiene. 2. Remove carrier by serological tests. 3. The first 4 -5 weeks of life should be protected. 4. Hyperimmune serum in newly hatched goslings. But needs two doses of serum.
Intervention 5. Active immunization of adult breeding geese and Muscovy ducks showed good protection via egg yolks. 6. Attenuation of virus in duck embryo cell cultures can be used. 7. Inactivated vaccines was effective.