OUTCOMES OF DOAC IN PATIENTS WITH MITRAL STENOSIS









 Dabigatran 367 (32. 9%) Rivaroxaban 472 (42. 3%) Apixaban")











- Slides: 22
OUTCOMES OF DOAC IN PATIENTS WITH MITRAL STENOSIS JACC VOL 73, NO 10, 2019
INTRODUCTION • AF is associated with an increased risk of thromboembolic events. • DOACs are effective in preventing thromboembolisms among patients with AF. • However, patients with moderate to severe mitral stenosis and mechanical prosthetic heart valves have been excluded from all pivotal trials. • Warfarin remains the only oral anticoagulant approved for patients with AF and mechanical prosthetic heart valves or moderate to severe mitral stenosis.
INTRODUCTION • Mitral stenosis combined with AF increases the risk of a stroke >20 times. • Mechanism is related to blood stasis in the left atrium. • Strokes or systemic embolization can be the first manifestation of mitral stenosis. • Can occur in patients with mild MS even before the development of other systems. • Thrombi in MS, even in the absence of AF, are often large, and can cause disastrous embolisms.
INTRODUCTION • Efficacy of warfarin in the prevention of thromboembolisms in mitral stenosis can be hampered by the poor quality of the anticoagulation therapy. • More pronounced in developing countries. • Desirable to determine the efficacy of DOACs in patients with MS + AF. • Many physicians are unclear of the definition of “nonvalvular AF”, and some of them try off-label use of DOACs in patients with MS, especially in the case of adverse events with warfarin. • Medical records of these patients were reviewed and compared with patients who received conventional warfarin treatment.
VALVULAR AF • ACC 2019: • • “…refers to AF in the setting of moderate-to-severe mitral stenosis (potentially requiring surgical intervention) or in the presence of an artificial (mechanical) heart valve. ” ESC 2016 & EHRA 2018 • “…refers to AF patients that have either rheumatic valvular disease (predominantly mitral stenosis) or mechanical heart valves. ” • EHRA Type 1: • • “refers to AF patients with VHD needing therapy with a vitamin K antag- onist (VKA), including in particular moderate –severe mitral stenosis of rheumatic origin and mechanical prosthetic valve replacement. ” EHRA Type 2: • “refers to VHD patients need- ing thromboembolic prevention therapy for AF with a VKA or a NOAC, including essentially all other native valvular stenoses and insuffi- ciencies as well as mitral valve repair, bioprosthetic valve replacements and transaortic valve intervention (TAVI). ”
METHODS • 98% of the population of South Korea belong to the mandatory National Health Insurance Service (NHIS). • Remaining 2% receive medical benefits for the lowest income population. • This study used the HIRA database. • National organization that reviews and assesses medical costs and health care service quality. • Mandatory for all health care providers to join the program. • Cohort dataset includes: • Patient ID, age, sex, prescription drugs, and diagnoses.
STUDY POPULATION • Inclusion criteria: • • MS of any degree (rheumatic, nonrheumatic, with or without insufficiency) AF • • • If recorded at least once in the database on hospital discharge or more than twice in the outpatient department. On oral anticoagulation for at least 3 weeks Between February 2008 and January 2017. • Exclusion criteria: • All patients who had a history of mitral valve surgery.
DATA COLLECTION AND STUDY OUTCOMES • • • Basic demographic data of each subject was acquired from the database. CHA 2 DS 2 -VASc score was calculated. Primary Outcome: • first hospitalisation with a principal diagnosis of an ischaemic stroke or systemic embolism after 3 weeks of DOAC use. • • Ischaemic strokes and systemic embolisms were defined as patients who did not have the preceding codes recorded for >1 year and new recorded codes were displayed consecutively at least twice at the time of the hospital discharge diagnosis. Safety Outcome: • Occurrence of an intracranial haemorrhage.
PATIENT CHARACTERISTICS
PATIENT CHARACTERISTICS DOAC N (%) Dabigatran 367 (32. 9%) Rivaroxaban 472 (42. 3%) Apixaban 192 (17. 2%) Edoxaban 84 (7. 5%)
OUTCOMES • Mean follow-up duration was 27 months.
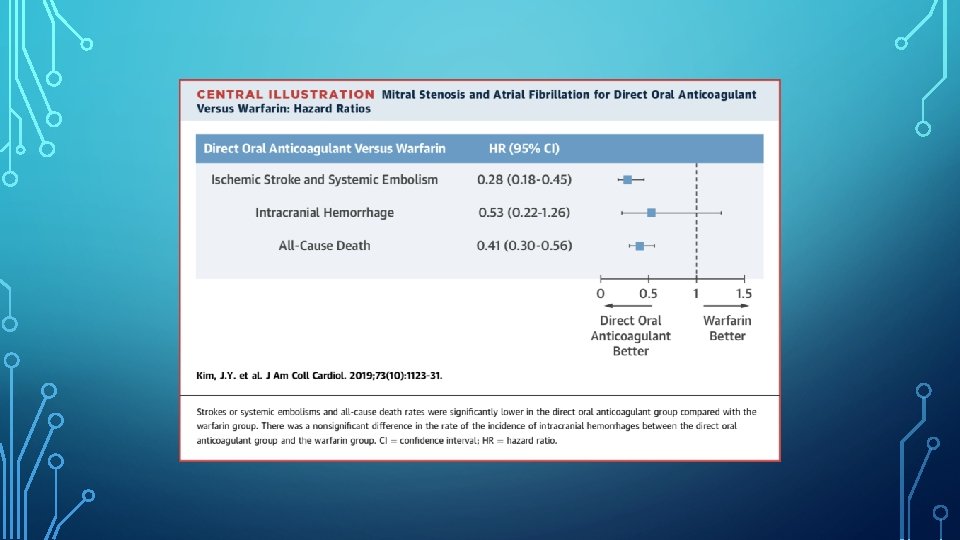
DISCUSSION • First study to investigate the efficacy of DOACs in patients with MS and AF. • Main findings: • • DOACs were associated with lower rates of thromboembolism. DOACs were as effective as warfarin in preventing haemorrhagic strokes.
DISCUSSION • In each of the 4 DOAC trials (edoxaban: ENGAGE AF-TIMI 48; dabigatran: RE-LY; rivaroxaban: ROCKET-AF; apixaban: ARISTOTLE): • • Patients with mechanical heart valves or haemodynamically significant mitral stenosis were excluded. All included mild MS (ENGAGE AF-TIMI 48: 254, RE-LY: 193, ARISTOTLE: 131, ROCKET-AF: not reported). • No published data on the effects of DOACs in patients with moderate to severe MS thus far. • However, this study was not able to ascertain the severity of MS.
DISCUSSION • RE-ALIGN trial • Randomized, Phase II Study to Evaluate the Safety and Pharmacokinetics of Oral Dabigatran Etexilate in Patients after Heart Valve Replacement) • Dabigatran increased both embolic and bleeding events.
DISCUSSION • Oral anticoagulation with a vitamin K antagonist is recommended in patients with: • • MS + AF MS + SR + history of prior embolic event or left atrial thrombus. • MS has much higher risk than other native valve diseases for strokes and should receive strict anticoagulation therapy. • However, the REMEDY trial showed that only a quarter of patients had an INR that was in a therapeutic range (on enrollment).
WARFARIN TREATMENT IN KOREAN PATIENTS • Real-world data shows that the quality of warfarin therapy is inadequate in Koreans. • A multicenter observational study of the quality of anticoagulation with warfarin in Korean patients showed that only 31% of patients were within therapeutic range – 41% INR <2. • Physicians concerns regarding high incidence of ICH with anticoagulation in the Asian population may have caused them to make the INR target low or not prescribe an anticoagulant. • HR 4. 06 vs Caucasians.
WARFARIN TREATMENT IN KOREAN PATIENTS • Unlike the CHA 2 DS 2 -VASc score system, doctors may not be familiar with the stroke risk of MS + AF. • A nationwide (Korea) study on the trends of antithrombotic therapy in high-risk AF patients showed that <41% received anticoagulants prior to DOACs being approved.
DISCUSSION • Rate of thromboembolic events with DOAC therapy in MS + AF was significantly lower than that in the warfarin group. • May be due to the low therapeutic control of the INR in the warfarin group. • Events rates were higher in this study population: 2. 22% in the DOAC group, and 4. 19% in the warfarin group. • In comparison, the DOAC trials had event rates <2%.
LIMITATIONS • Study conducted with data from off-label use. • Several reasons why patients received DOACs • • Developing thromboembolisms or bleeding events during warfarin use. Off label-use of DOACs before the evaluation of MS. Mild MS. Retrospective observational study using the HIRA database. • • • Unable to ascertain the severity of MS and other valvular pathologies. Data does not contain lab findings or clinical measurements. Unable to rule out misclassification of patients with MS. • Diagnoses made based on ICD-10 codes alone.
LIMITATIONS • Excluded patients who underwent mitral valve surgery in this study protocol. • Exclusion of patients who had severe mitral MS and were at a higher risk for thromboembolic events. • Reduced study population after propensity score matching. • Information regarding the INR and time in therapeutic range was not available.
CONCLUSION • This study revealed worthwhile exploratory data on the effectiveness of DOACs in patients with mitral stenosis and AF. • DOAC use appears reasonable in patients with MS and AF. • Clinical trial evaluation of the superiority of DOACs in moderate to severe MS would be justified.