Tracheal Surgery Sina Ercan M D Yeditepe University



































- Slides: 64
Tracheal Surgery Sina Ercan, M. D. Yeditepe University Department of Thoracic Surgery
Lesson: Surgical Pathologies of Trachea and Their Treatment At the end of this lecture, the student should be able to: • List the presenting symptoms of patients with tracheobronchial stenosis • List the major pathologies of trachea • Explain the main role of cervicothoracic somputerized tomography and pulmonary function tests in diagnosing tracheal obstructive pathologies • Define the pathologic cascade of developement in postintubation tracheal stenosis • Explain the initial evaluation and management of patients with tracheal stenosis
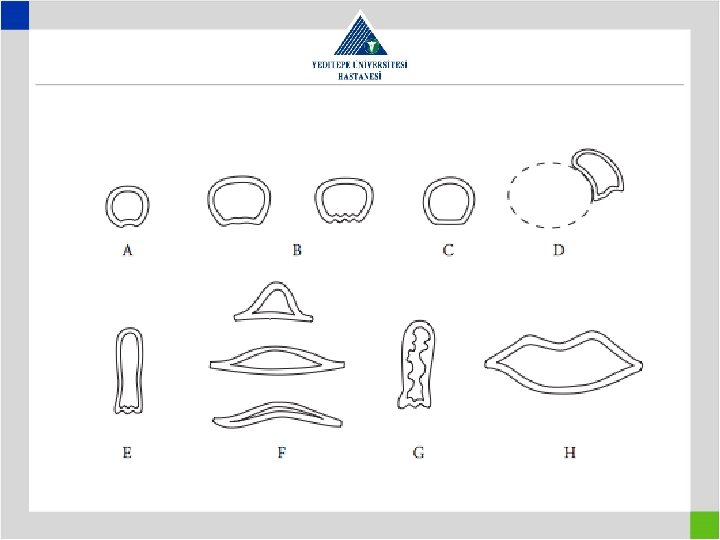
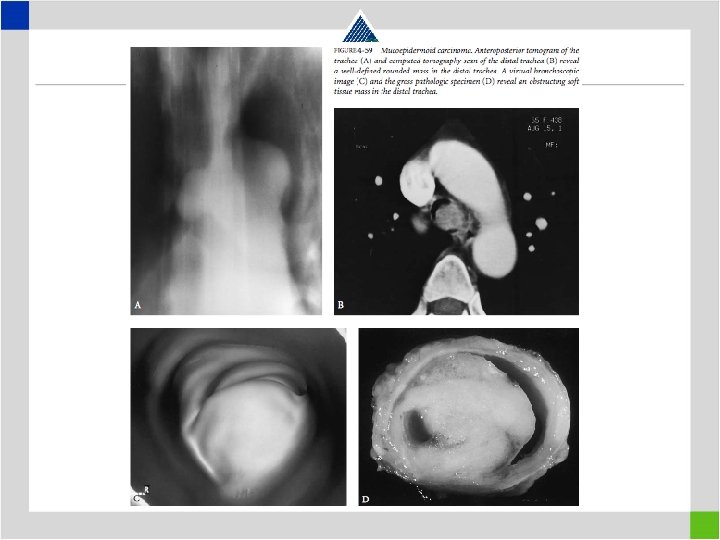
Tracheal Stenosis Etiology • Benign stenosis – Idiopathic stenosis – Iatrogenic stenosis • Postintubation stenosis • Due to previous surgical interventions – Traumatic stenosis – Benign tumors and pathologies • Malignant stenosis – Primary malignant tracheal tumors – Secondary malignant tracheal tumors
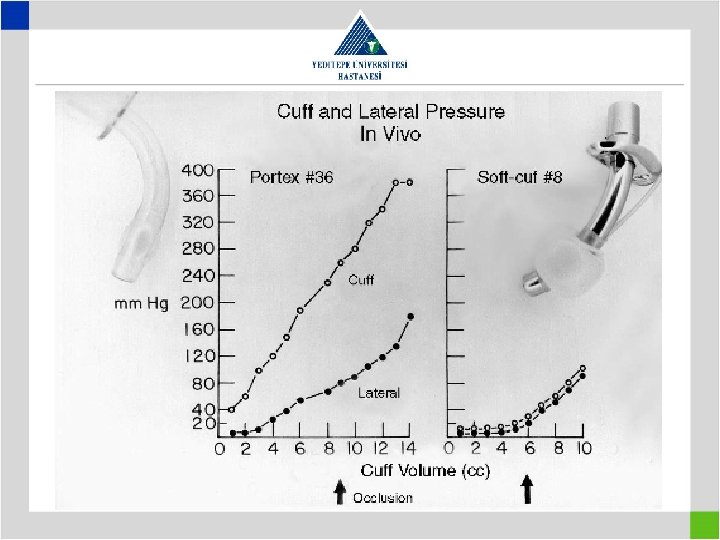
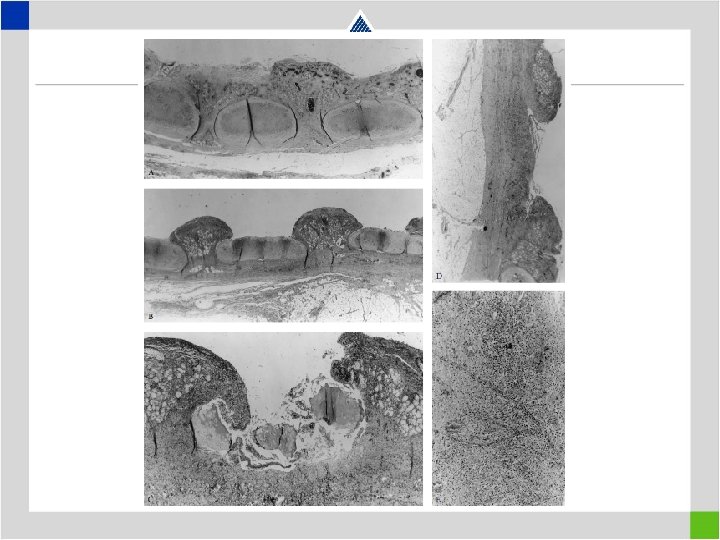
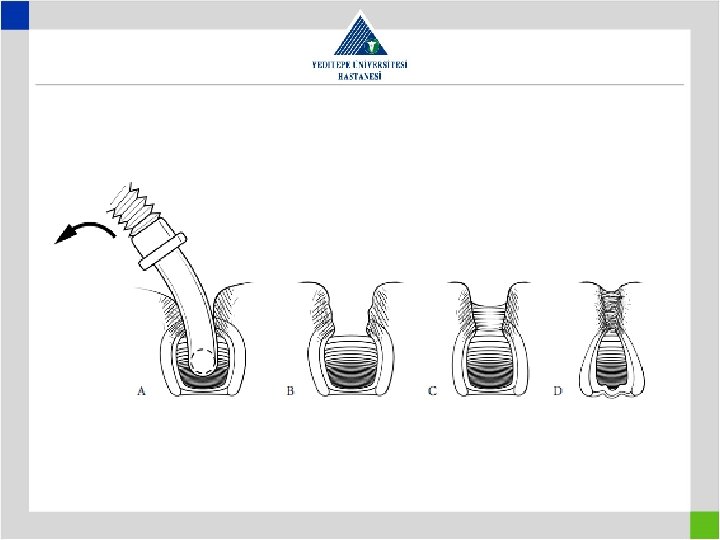
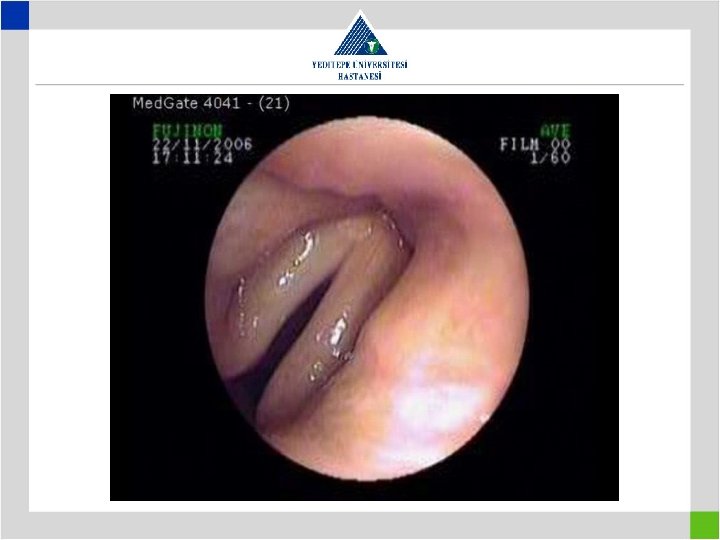
• Terminal tracheal injury due to high cuff pressure
Diagnosis • Airway obstruction symptoms such as dyspnea, stridor • Patients can be misdiagnosed with asthma and treated for years • Flow-volume loop compression on both phases is typical for airway obstruction
Diagnosis • Flow-volume loop in fixed airway obstrucion
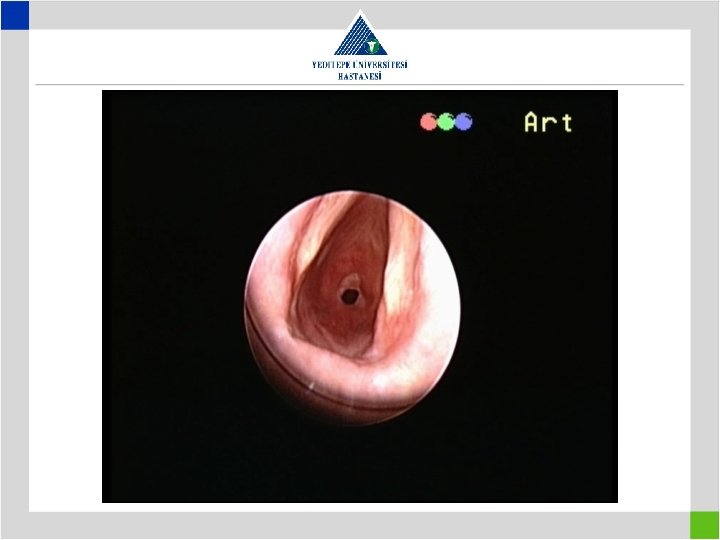
Diagnosis • Preop glottic insufficiency to be searched – Preop awake laryngoscopy – Preop work-up for presence of aspiration – Tracheostomy means previous intubation – look for a distal second lesion – Vocal cords do not move both in paralysis and cricoarythenoid arthritis or traumatic ankylosis
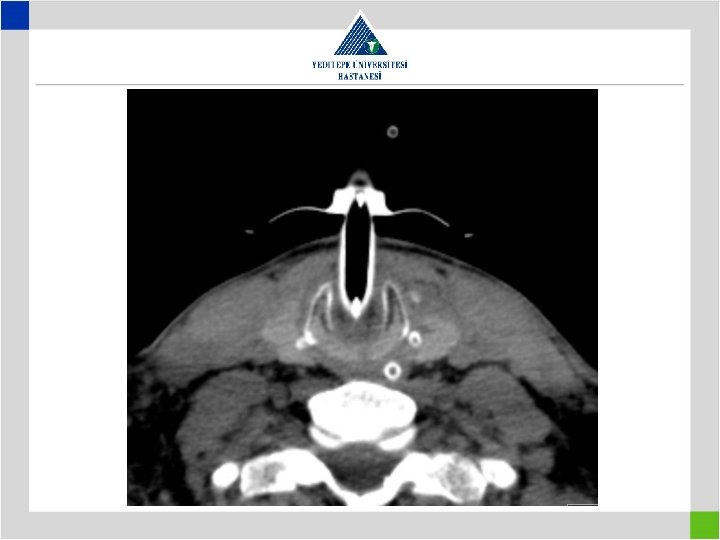
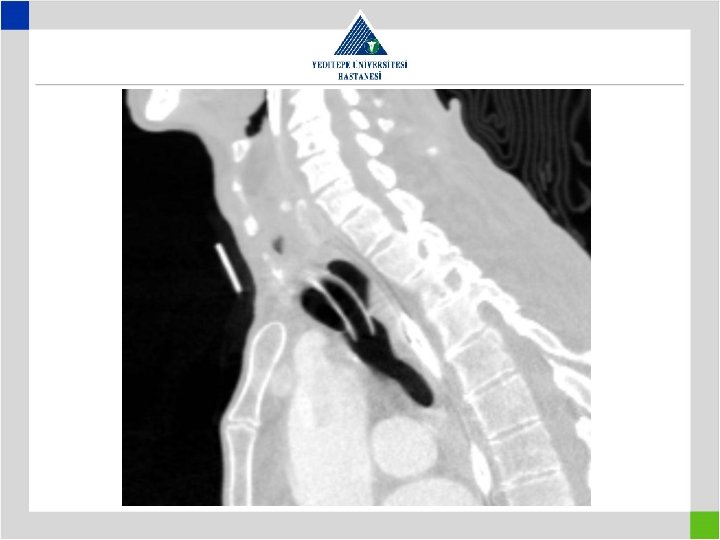
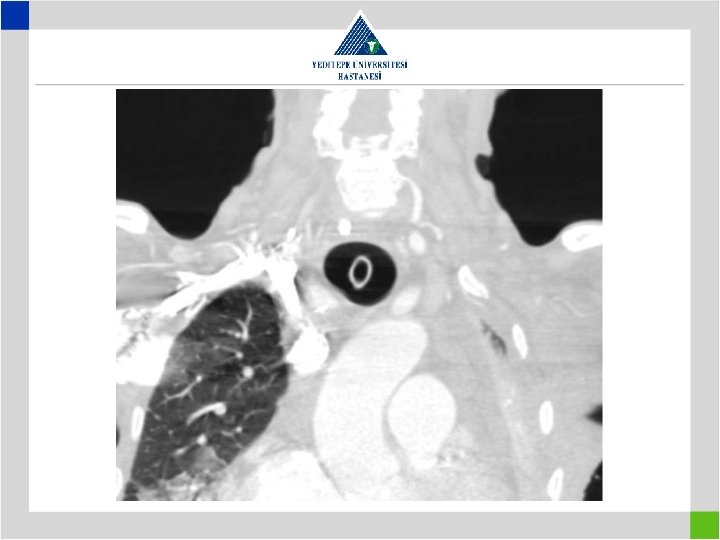
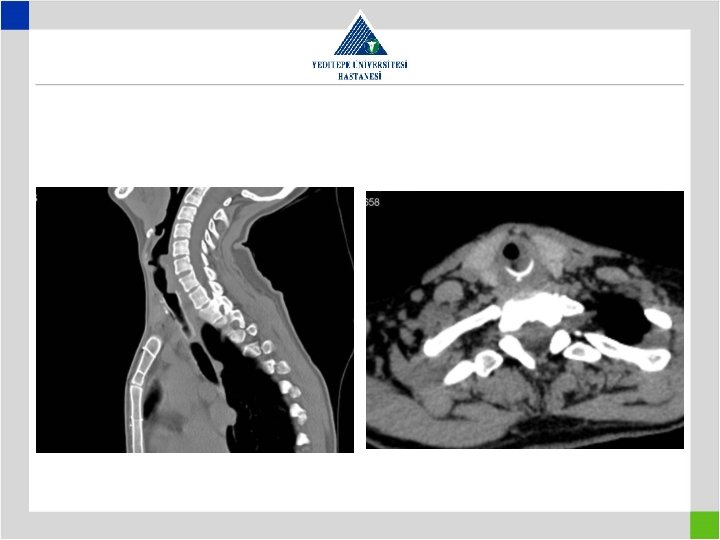
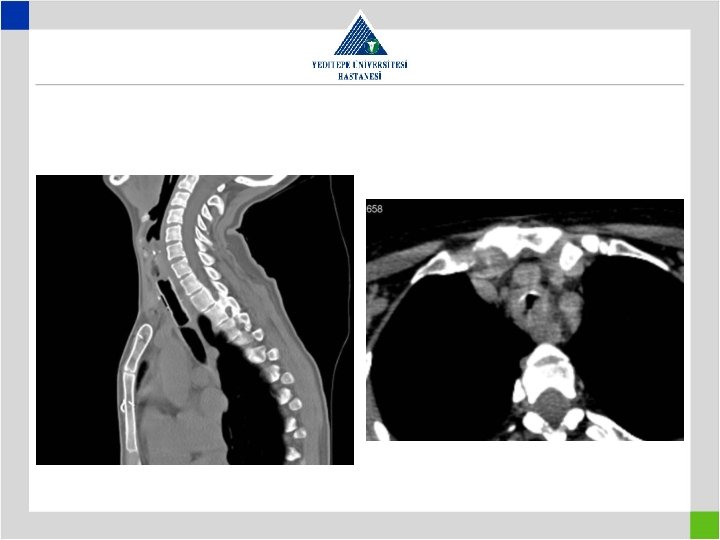
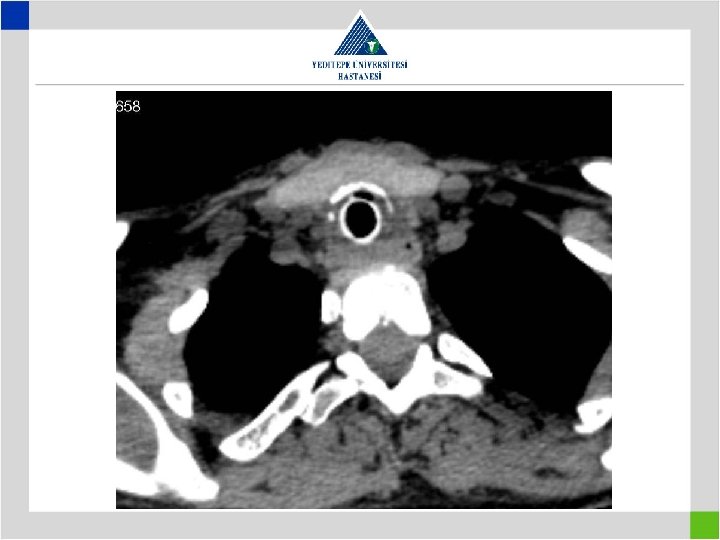
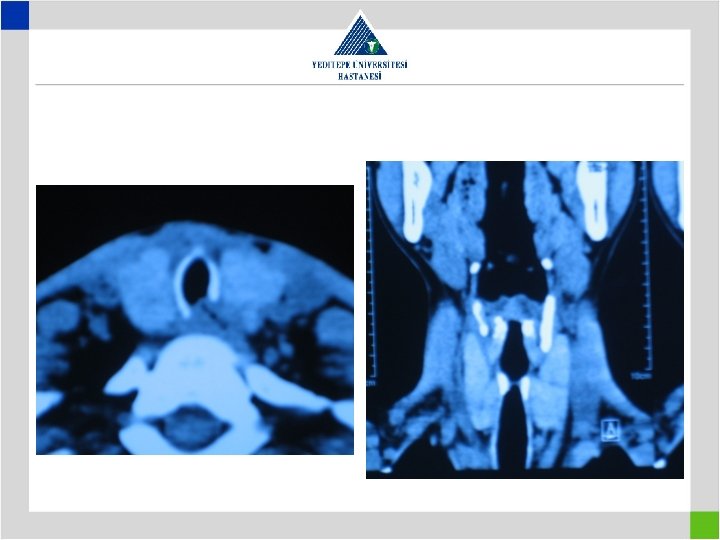
Diagnosis • Stenotic segment calculation to be correct • CT image in supine position may falsly indicate a preglottic stenosis – Overresection – increased anastomotic tension – restenosis • Pediatric trachea tolerates the tension poorly in comparison with adults – Insufficient resection – remaining fibrosis – restenosis
Tracheomalasia
Iatrogenic Laryngotracheal Stenosis • Incorrect tracheostomy applications – Wrong indication – Wrong technique – Wrong care
Iatrogenic Laryngotracheal Stenosis • Incorrect tracheostomy applications – Wrong indication -–- Wrong technique – Wrong care
Iatrogenic Laryngotracheal Stenosis • Incorrect tracheostomy applications – Wrong indication – Wrong technique – Wrong care Care
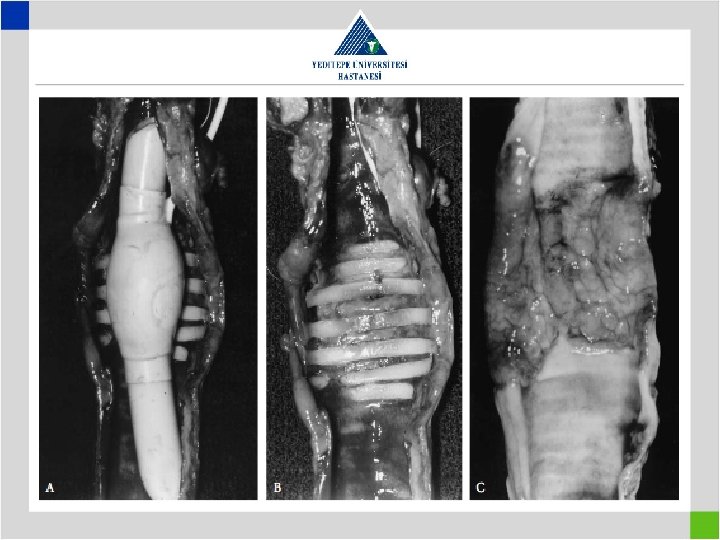
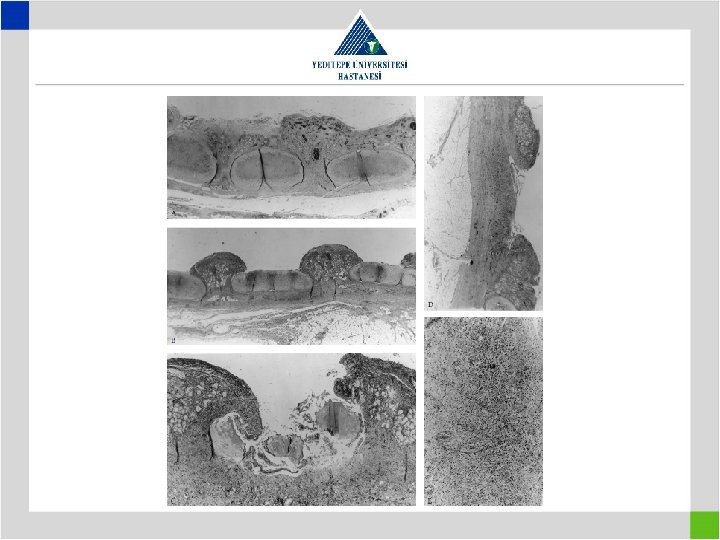
Iatrogenic Factors • Metal stents in bening tracheal conditions cause elongation of pathologic segment and cause the patient to loose the previously present chance of surgical cure
Iatrogenic Factors • Continuous suturing technique with nonabsorbable suture material resulting in restenosis
• Suture material preference – Nonabsorbable sutures • More calcification in anastomosis • Protruding into the lumen over time, causing granulation – Absorbable sutures • Monofilament • Multifilament • Suture technique – Interrupted suture in pediatric patients • 4/0 sutures in adults and 5/0 in pediatrics
Restenoz
Restenoz
Idiopathic and Postintubation Laryngeal Stenosis
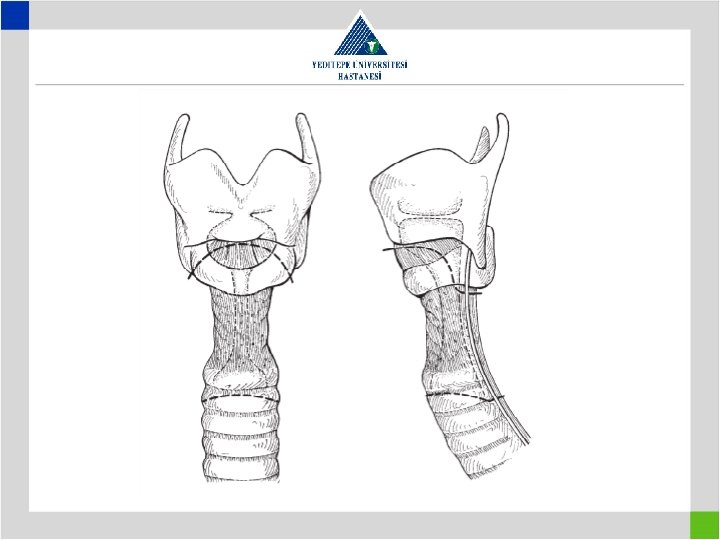
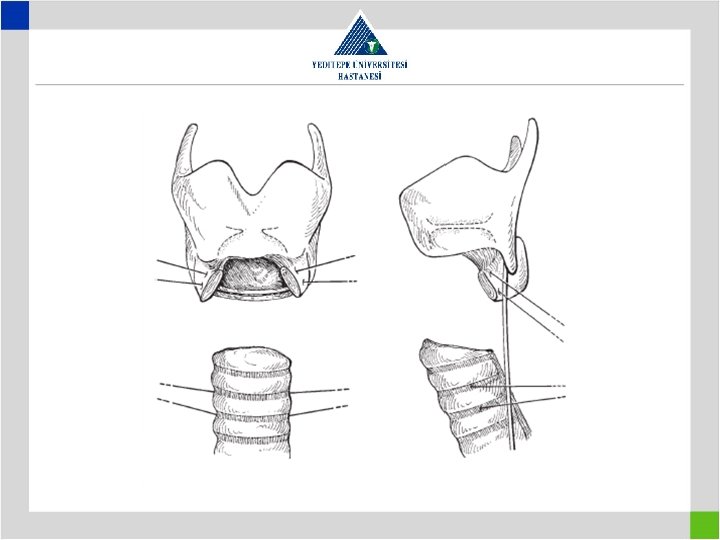
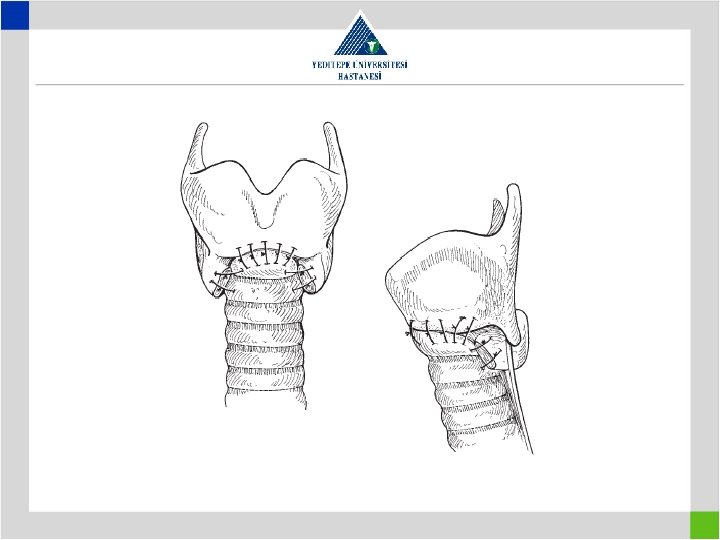
Laryngotracheal Resection Technique • These resections are different and more complex than a regular tracheal resection • Subglottic laryngeal airway is narrow and usually affected by scar formation • Laryngotracheal anastomosis requires at least 6 mm of a healthy distance beyond the vocal cords
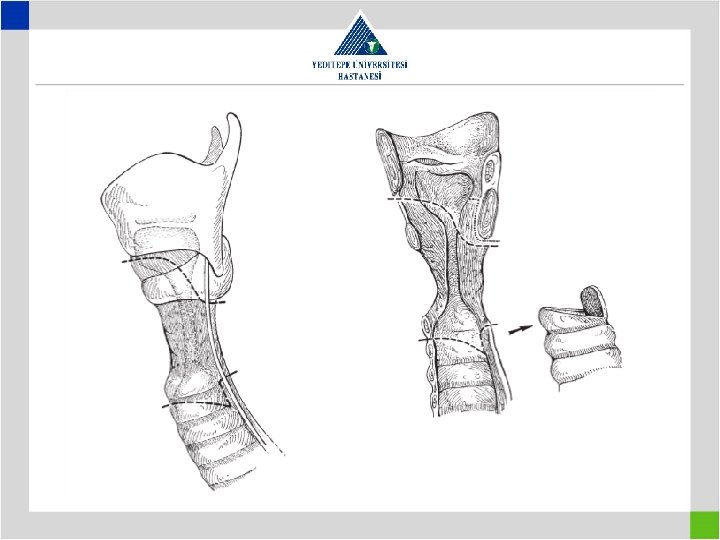
Laryngotracheal Resection with Posterior Membrane • Especially postintubation stenosis involves cricoid cartillage 360° • The scar tissue on the posterior cricoid plate needs to be excised
Complications in Laryngotracheal Resections • Vocal cord problems and deglution problems can be symultaneous • Deglution problems usually seen following release techniques – Thyrohyoid > suprahyoid release Also after; - Long segment resection - Advanced age - Presence of neurological problems
Complications in Laryngotracheal Resections • Laryngeal edema is more common after laryngotracheal resection • Postextubation wheezing and stridor • Edema can be differentiated from cord paralysis by examining under mild anesthesia • In edema a #5. 5 – 6 ETT is placed and kept in trachea for a few days, then extubate • If edema continues then tracheostomy placed
Treatment of Complications • Best treatment is to prevent the complications • In tracheal surgery the best chance lies in the first surgery • A T-tube providing a sufficient airway sometimes to be prefered over a risky resection and reconstruction
Treatment of Complications • Minimal aspiration is normal in elderly • If preoperative aspiration was serious and resistant to treatment then a permanent tracheostomy is the right treatment • Postoperative aspiration may improve with physiotherapy over time
Treatment of Complications • A significant complication of laryngotracheal resections is uni- or bilateral vocal cord paralysis • This may improve over time • If persistant, then the cord is fixed in such a position that, it will allow enough phonation while not limiting the breathing
Conclusions • Success in tracheal surgery is highly volume dependent and not appropriate for occasional performance • Preop evaluation is not with only CT but should include physiologic, anatomic and endoscopic evaluation • A dedicated anesthesiologist and an ENT specialist to be included in the team
Conclusions • Proper infrastructure and surgical tools to be available – – Flexsible and rigid endoscopy sets Fast track laryngeal mask Jet ventilator A collection of different size and model T-tubes and tracheostomy tubes • The surgeon to be competent in the old and current literature knowledge and he should always have a B and even a C plan in mind