Please Confirm your attendance tiny ccintusatt Submission is

Please. . Confirm your attendance tiny. cc/intusatt Submission is open until 7: 40

Intussusception

Intussusception acquired intussusceptum intussuscipiens

PATHOPHYSIOLOGY peristaltic activity mesentery venous obstruction arterial insufficiency

PATHOPHYSIOLOGY • The intussusceptum telescopes into the distal bowel by peristaltic activity. • There may or may not be a lead point. • The mesentery of the proximal bowel is compressed, resulting in venous obstruction and bowel wall edema may progress into arterial insufficiency ischemia and bowel wall necrosis.

PATHOPHYSIOLOGY • The intussusceptum telescopes into the distal bowel by peristaltic activity. • There may or may not be a lead point. • The mesentery of the proximal bowel is compressed, resulting in venous obstruction and bowel wall edema may progress into arterial insufficiency ischemia and bowel wall necrosis.

Types of Intussusception - most common

Primary Intussusception no lead point gastroenteritis recent URTI

Secondary Intussusception identifiable lead point
")
Secondary Intussusception § Meckel diverticulum (most common)

Please. . Confirm your attendance tiny. cc/intusatt Submission is open until 7: 40

INCIDENCE well-nourished boys highest incidence

CLINICAL PRESENTATION intermittent ‘currant jelly’ stools mass this triad is seen in <25% of children


CLINICAL PRESENTATION pull the legs • Between attacks comfortable

CLINICAL PRESENTATION
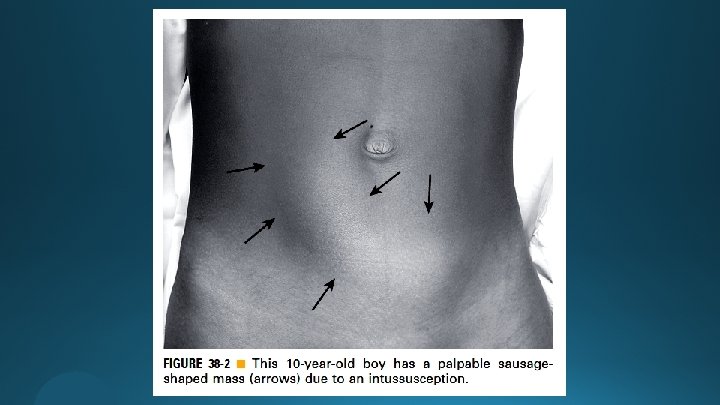
 § Sausage-shaped (Dance sign)")
PHYSICAL EXAMINATION (early) § Sausage-shaped (Dance sign)
![PHYSICAL EXAMINATION (late) [ ? rectal prolapse ]](http://slidetodoc.com/presentation_image_h/18292c4d4bcecd19523e2e133edeca28/image-19.jpg "PHYSICAL EXAMINATION (late) [ ? rectal prolapse ]")
PHYSICAL EXAMINATION (late) [ ? rectal prolapse ]

DIAGNOSIS
 not used")
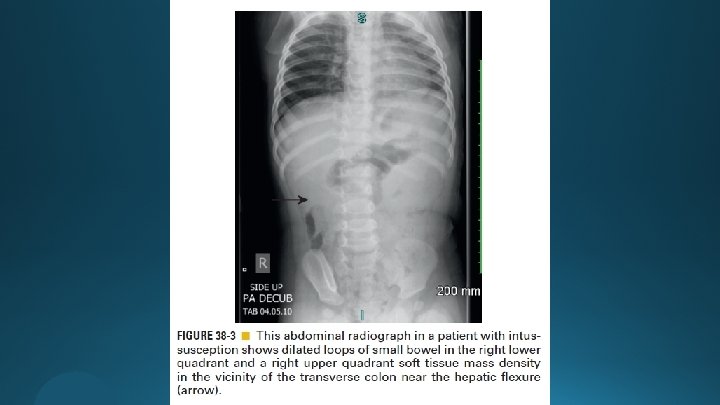
Abdominal Radiography (AXR) not used
 Target doughnut Pseudokidney")
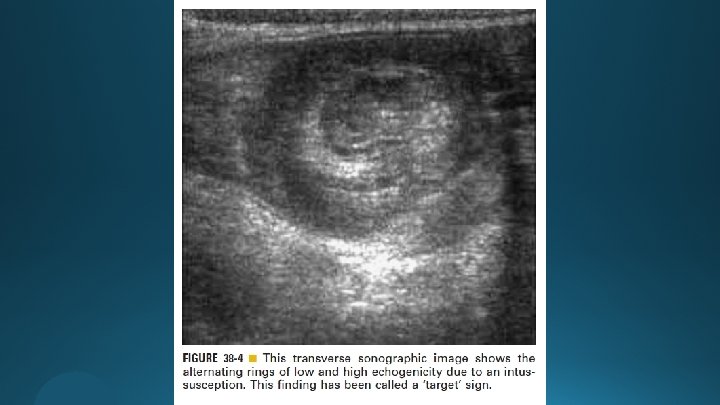
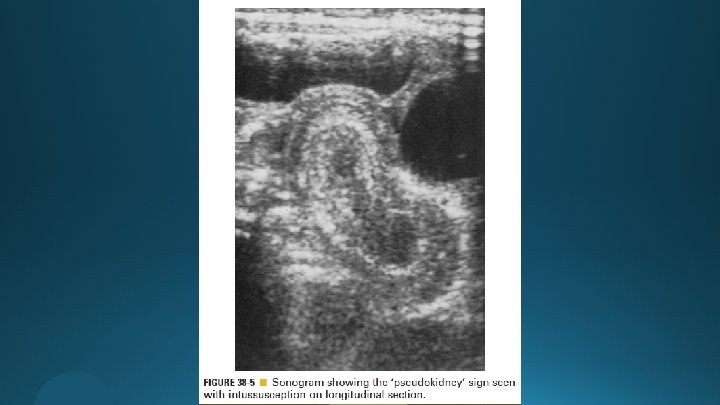
Ultrasonography (US) Target doughnut Pseudokidney

CT and MRI

NONOPERATIVE MANAGEMENT
 § Peritonitis § Persistent")
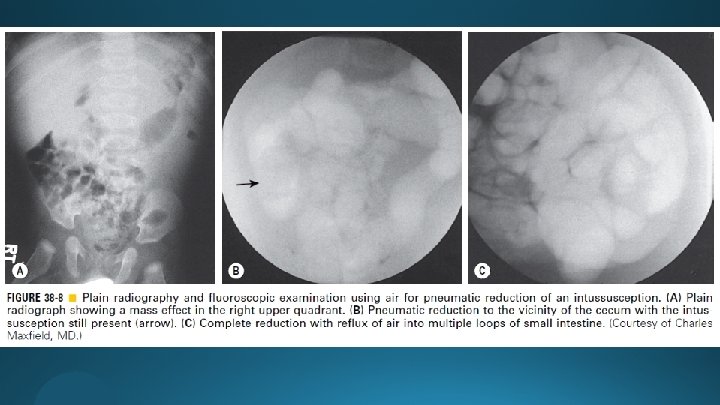
Hydrostatic and Pneumatic Reduction § Intestinal perforation (free intra-abdominal air) § Peritonitis § Persistent hypotension § Decreased morbidity § Dec. cost § Dec. length of hospitalization

Hydrostatic and Pneumatic Reduction ≈85%
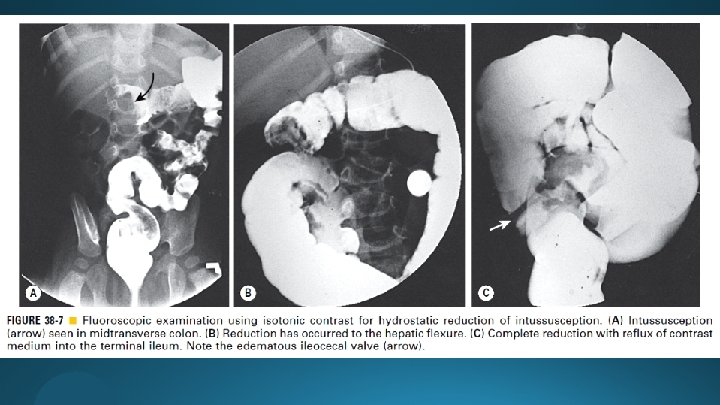

Hydrostatic and Pneumatic Reduction - 80 mm. Hg for younger infants - 110– 120 mm. Hg for older infants - Possibility of tension pneumoperitoneum (rates of perforation 0. 4 -2. 5%) - Poor visualization of lead points - Poor visualization of the intussusception reduction process

Hydrostatic and Pneumatic Reduction cessation large gauge needle exploration

Hydrostatic and Pneumatic Reduction § Unsuccessful § Successful - Be admitted for observation - Receive a short period of bowel rest - Be given intravenous fluids

OPERATIVE MANAGEMENT

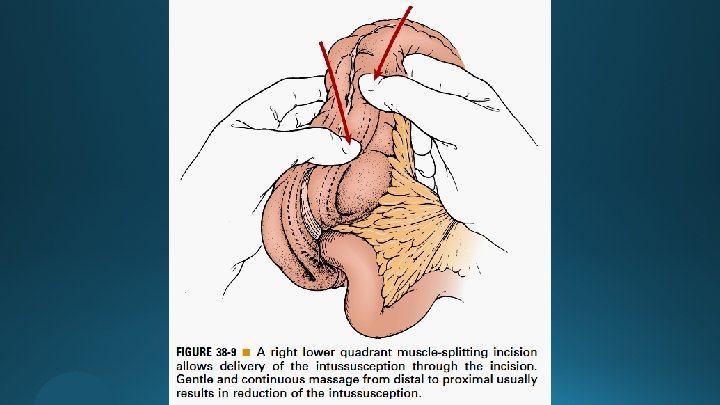
Open Approach

Open Approach

Open Approach - Inability to manually reduce the intussusception - The finding of ischemic bowel - Identification of a lead point

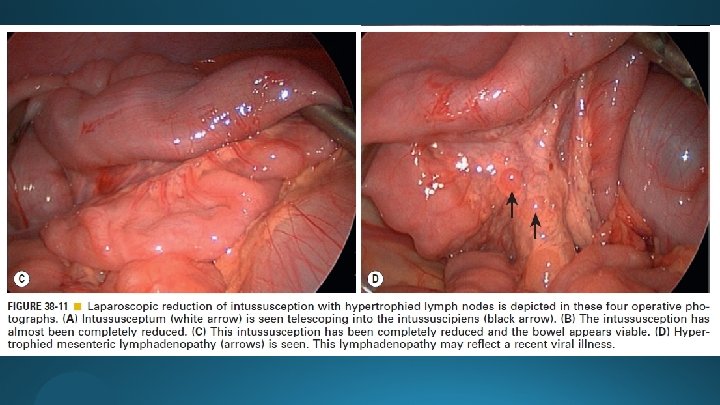
Laparoscopic Approach
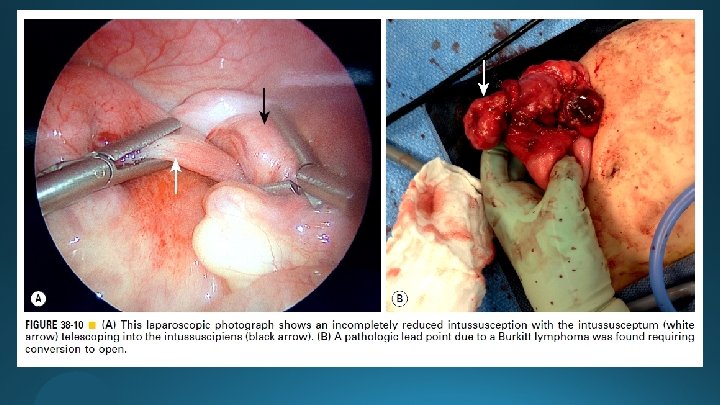

Laparoscopic Approach
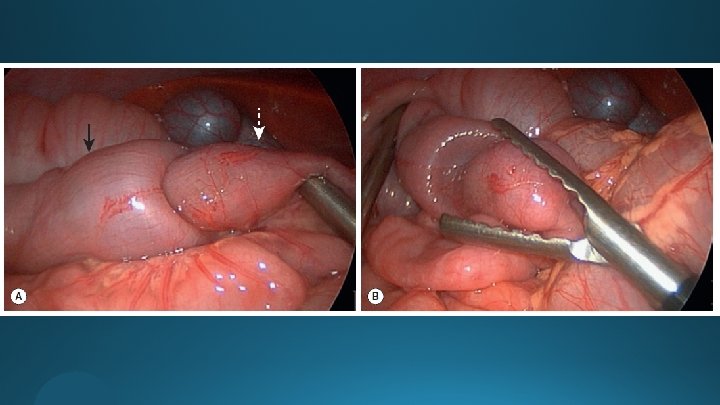
 (parents")
RECURRENT INTUSSUSCEPTION 10– 15% less likely up to 10% are more aware) (parents

POSTOPERATIVE INTUSSUSCEPTION

POSTOPERATIVE INTUSSUSCEPTION • Dx: • Rx:

HYPERTROPHIC PYLORIC STENOSIS
")
HYPERTROPHIC PYLORIC STENOSIS (HPS)

Etiology

Diagnosis
 (signs of gastritis are not uncommon (‘coffee-ground’ emesis))")
Diagnosis (projectile) (signs of gastritis are not uncommon (‘coffee-ground’ emesis))

Diagnosis “olive sign” Profound dehydration (rarely seen today due to early Dx and proper fluid management)
![Diagnosis seen in most patients [ ? paradoxical aciduria ]](http://slidetodoc.com/presentation_image_h/18292c4d4bcecd19523e2e133edeca28/image-54.jpg "Diagnosis seen in most patients [ ? paradoxical aciduria ]")
Diagnosis seen in most patients [ ? paradoxical aciduria ]

Diagnosis ≥ 4 mm ≥ 16 mm
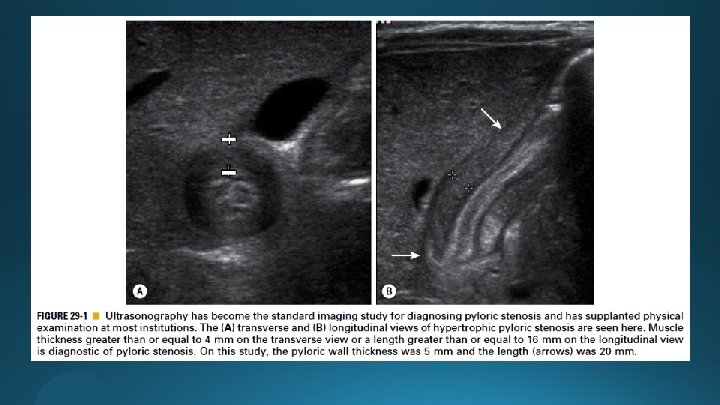

Diagnosis

DDx for nonbilious vomiting

Treatment NOT Pyloromyotomy

Treatment

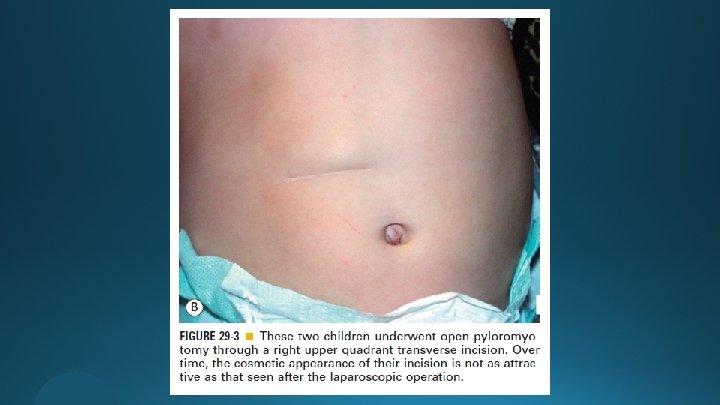
The Open Approach § Right upper quadrant transverse incision § Omega-shaped incision

The Open Approach

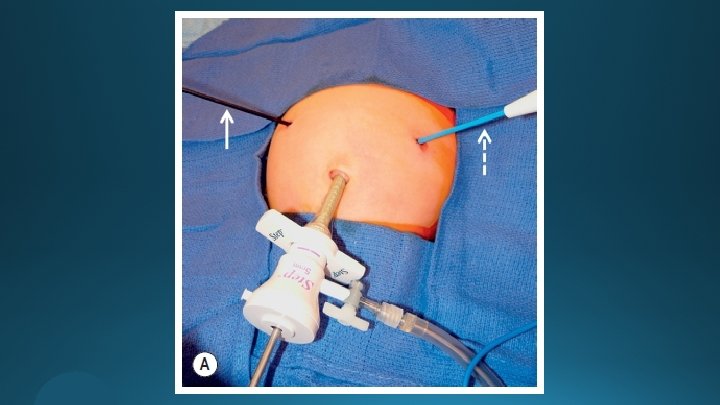
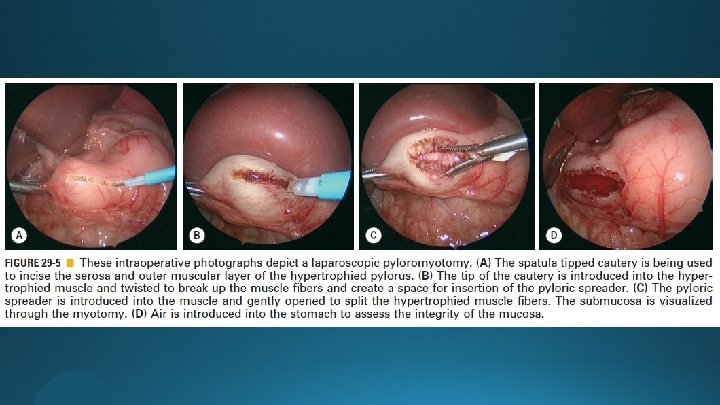
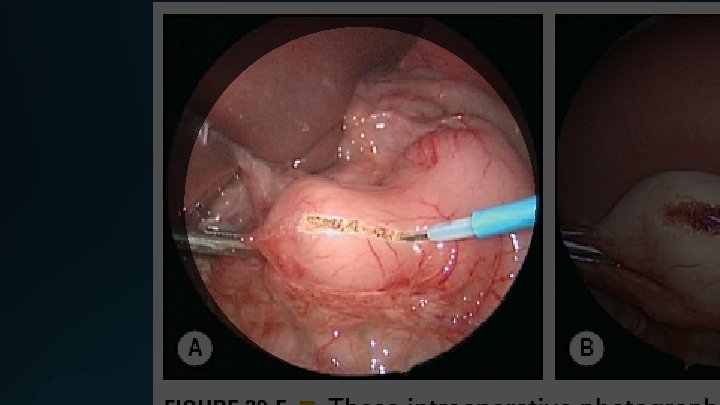
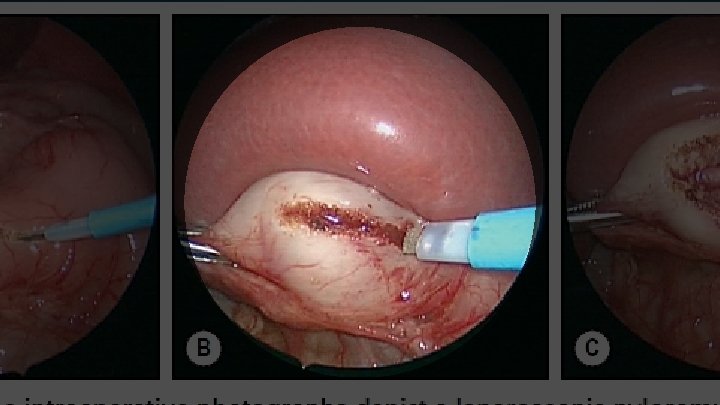
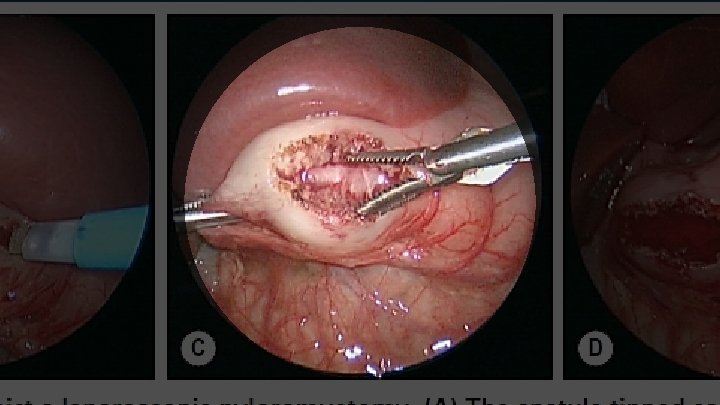
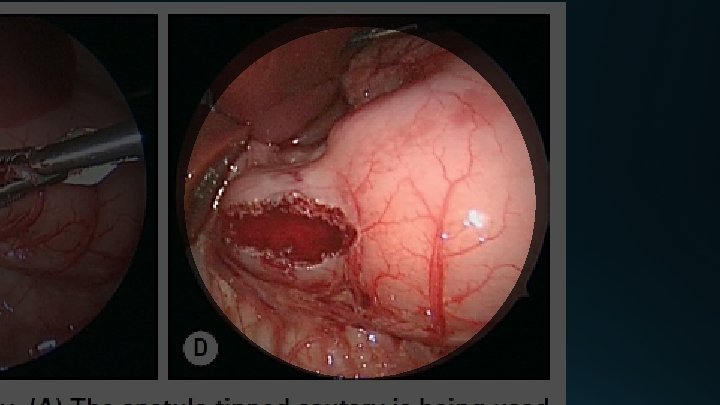
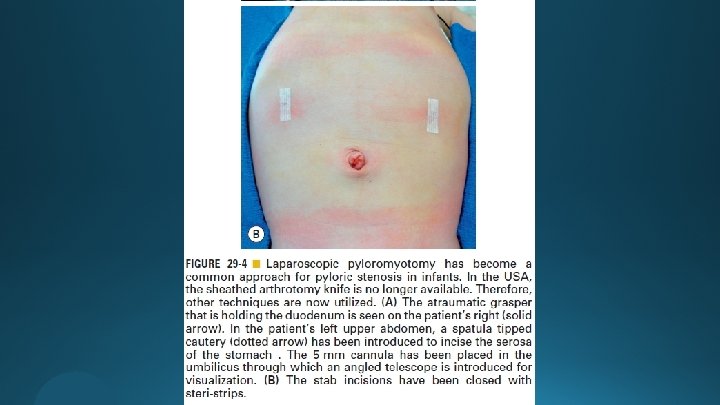
The Laparoscopic Operation

Postoperative Care

Complications

Outcomes mortality • Morbidity nearly zero

tiny. cc/intusfiles Raed Al-Taher, MD Department of General Surgery Division of Pediatric Surgery University of Jordan Hospital University of Jordan r. altaher@ju. edu. jo
- Slides: 76