Mitral valve repair Anatomy Mitral Stenosis Opening of





 • Slow process. • Repeated")



 Ischemia. Congenital. Cardiomyopathy.")
 • Type")






















- Slides: 36
Mitral valve repair
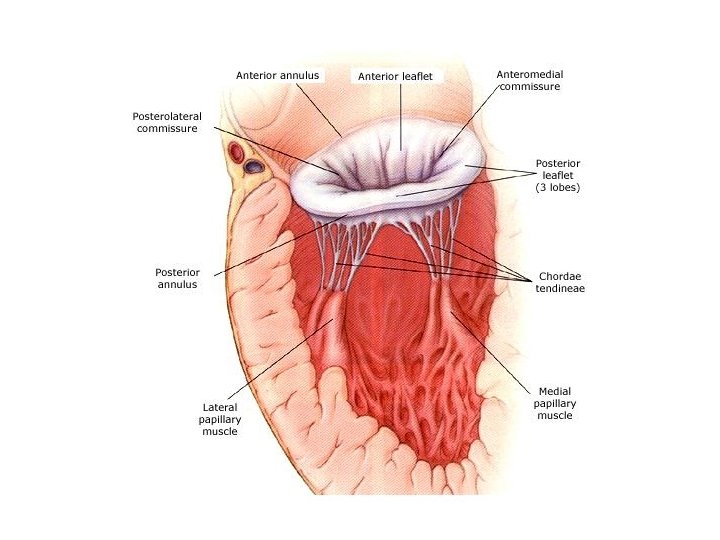
Anatomy
Mitral Stenosis Opening of the valve is narrowed. Normal valve opening 4 -6 cm sq. Symptoms 2 -2. 5 cm sq. Severe < 1 cm sq.
Pathophysiology • • High pressure in left atrium and lungs. Increase work of right ventricle. Atrial fibrillation. (palpitations) Stroke.
Causes of Mitral Stenosis • Rheumatic fever. • Congenital.
Rheumatic fever • Immune complexes. (Strep throat/ renal infections) • Slow process. • Repeated attacks. • Replacement.
Indication for surgery • Valve opening area < 1. 5 cm sq. • Gradient > 12 mm. Hg.
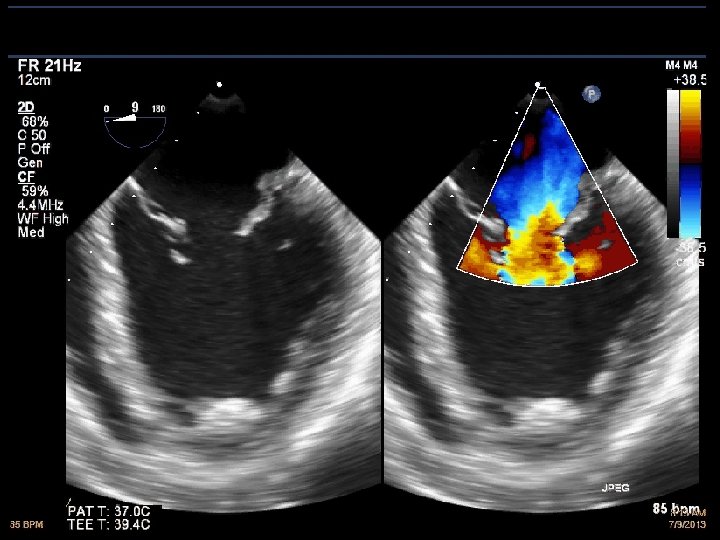
Mitral Incompetence • • Valve does not close properly. Blood flows back into the left atrium. Volume overload of left ventricle. Left ventricular failure.
Aetiology • • • Rheumatic Fever. Endocarditis Barlow's syndrome. (Floppy valve) Ischemia. Congenital. Cardiomyopathy.
Carpentier classification • Type 1 - Normal leaflet movement, annular dilatation. (cardiomyopathy) • Type 2 - Increased leaflet movement, prolapsing segments. (Barlow's) • Type 3 a- Restricted leaflet movement. ( Rheumatic) • Type 3 b- Ischaemic leaflet retraction
Surgery • • • General anaesthesia. TEE on board. Cardio-pulmonary bypass. Cell saver. Repair before replace.
Type 1: Annulus dilatation
Remodelling annuloplasty
Type 2 – Valve prolapse • • To much thickened leaflet. Stretched out chordae. Elongated papillary muscles. Leaflet prolaps.
Mitral valve segments
Quadrangular excision repair
TEE- Post repair
Triangular excision repair
Artificial chordoplasty
Artificial chordoplasty and cleft repair
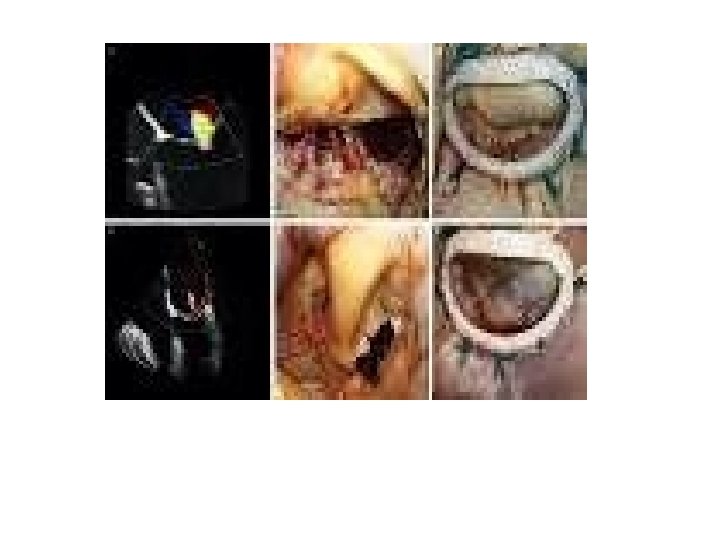
Type 3 a- Rheumatic valves
Type 3 b- Ischaemic incompetence • Valve dysfunction because of impaired coronary blood flow. • Posterior leaflet retraction. (P 3 area) • Needs to be fixed > moderate incompetence. • Remodelling annuloplasty.
Mitral valve replacement • Native valve removed. • Mechanical or Tissue prosthesis.
Mechanical prosthesis
Tissue prosthesis
Mechanical mitral valve replacement • • Surgical mortality Bleeding risk Thrombo-embolism Endocarditis 2% - 4% 1%/year 0. 1%/year
Clotted mitral valve
Pannus ingrowth
Minimally invasive mitral surgery
The future- Robotic surgery