MITRAL STENOSIS JMJ 1 Mitral stenosis Mitral valve













 –")




 indicate chronic")








 • Auscultation – Loud")

 • Small volume pulse • Usually regular in early stages, • If")

 • Severe mitral stenosis with pulmonary hypertension • Mitral fascies / malar")
 • If R heart failure develops • obvious distension of jugular")
 • Tapping impulse felt parasternally on left side • Palpable 1 st")
 • Loud 1 st heart sound – If the mitral valve is")
 • If the patient is in sinus rhythm – Murmur becomes louder")
































 follows A 2")
 RV hypertrophy P mitrale or atrial")





- Slides: 88
MITRAL STENOSIS JMJ 1
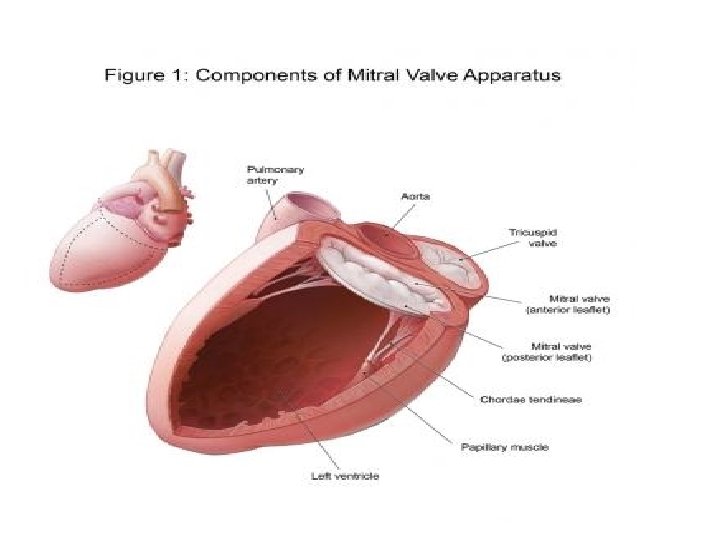
Mitral stenosis • Mitral valve – Consist of fibrous annulus, – Anterior & posterior leaflets – Chordae tendinae, – Papillary muscle JMJ 2
FIVE MITRAL VALVE COMPONENTS
Mitral Annulus: Anatomical structure that separates the LV & LA
MITRAL LEAFLETS Mitral Leaflets & Scallops: Thin and pliable leaflets that contain scallops which represent segmental markers. Anterior Leaflet (AML): larger & thicker Dome-shaped Scallops: A 1 (lateral), A 2 (central), A 3 (medial) Posterior Leaflet (PML): thinner & more flexible Crescent shaped
Chordae Tendinae: Fibrous strings that attach specific portions of mitral leaflets to papillary muscle tips Normal average length is around 20 mm Normal average thickness is 1 -2 mm Primary (marginal)- attaches at leaflet tips (‘coaptation line’) Function to maintain coaptation of leaflets Failure of primary leads to rupture or elongated chordae Cause development of prolapse or flail leaflet Secondary (basal)- attaches at midbody of leaflets Provides support length to leaflets Thicker & longer Can rupture & not damage coaptation or develop regurgitation Tertiary– attaches at base of leaflets Function as structural suppor
Papillary Muscles: Large trabeculae muscles that branch from 1/3 rd of LV, connecting chordae to mitral leaflets 2 papillary muscles: Anterolateral (APM): Dual blood supply (LAD & Cx) Posteromedial (PPM): Single blood supply (Either RCA or LCX) Prone to injury from MI due to single blood supply
The mitral apparatus has very specific details that make up the large picture of the ‘mitral valve’. If we zoom in on the mitral leaflets from the atrial surface, we can identify two zones that are used for describing location of pathology seen. Body (‘Smooth’) Zone: surface area on leaflet body Coaptation (‘Rough’) Zone: represents the coaptation area of leaflets. Crucial area to observe in assessment of mitral valve function
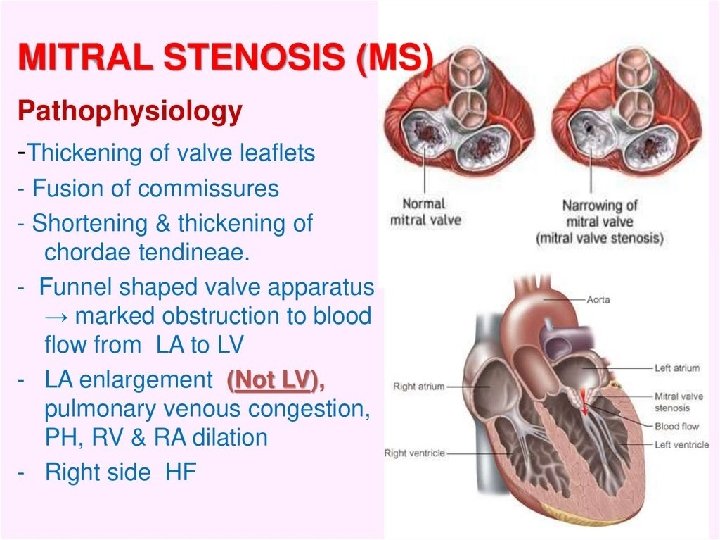
Mitral stenosis • MS is characterized by obstruction to left ventricular inflow at the level of MV due to structural abnormality of the MV apparatus. • MS is due to thickening and immobility of the mitral valve leaflets. • The normal MVO has a CSA of 4 -6 cm 2. 1. Carabello, B. A. (2005). "Modern Management of Mitral Stenosis". Circulation 112 (3): 432– 7
Mitral Stenosis • Almost always rheumatic in origin – although in older people it can be caused by heavy calcification – also a rare form of congenital MS • Mitral valve orifice slowly gets diminished (5 cm 2 - 1 cm 2 ) – Progressive fibrosis, – Calcification of the valve leaflets – Fusion of the cusps and subvalvular apparatus.
Etiology • Rheumatic heart disease • Congenital MS • Mitral annular calcification (particularly in patients with ESRD). • Conditions that simulate MS: IE with large vegetation, LA myxoma, ball valve thrombus, and cor triatum. • Less common causes: malignant carcinoid disease, SLE, RA, mucopolysaccharidoses, Fabry disease, Whipple disease, and methysergide therapy.
Pathophysiology • The flow of blood from LA to LV is restricted and left atrial pressure rises. . • Leading to pulmonary venous congestion and breathlessness. • There is dilatation and hypertrophy of the LA, • And left ventricular filling becomes more dependent on left atrial contraction.
To maintain sufficient cardiac output 1. Left arterial pressure increases 2. Left arterial hypertrophy and dilation 3. Pulmonary veins, pulmonary arterial and Rt heart pressure increases 4. Increase of pulmonary capillary pressure 5. Followed by development of – pulmonary oedema – Atrial fibrillation with tachycardia – Loss of coordinated atrial contraction JMJ 5
To maintain sufficient cardiac output 6. This is prevented by (Reactive pulmonary hypertension) – Alveolar and capillary thickening – Pulmonary arterial vasoconstriction 7. Pulmonary hypertension leads to – R/ ventricular hypertrophy, dilation and failure with subsequent tricuspid regurgitation JMJ 6
Pathophysiology • Normal valve area: 4 -6 cm 2 • Mild mitral stenosis: 2 – MVA 1. 5 -2. 5 cm – Minimal symptoms • Moderate mitral stenosis 2 – MVA 1. 0 -1. 5 cm usually does not produce symptoms at rest • Severe mitral stenosis – MVA < 1. 0 cm 2 JMJ 4
Pathophysiology: MS ↓ MVA ↑ LAP, LAE LA remodelling AFib LA clot LA enlargement (compensation to attempt to lower LAP) ↑ LAP transmitted to pulmonary venous system Pul congestion ↑PVR , PHTN Exertional Dyspnea /Pul edema RV pressure overload RVH RV dilates & fails Fatigue/Dyspnea/ ↓Functional capacity CO ↓ (first with exercise then at rest) With significant obstruction to flow from PVR & MS
Pulmonary Hypertension Backward transmission of the elevated left atrial pressure Loud P 2, later becomes palpable Parasternal heave TR Hepatomegaly & Pulsatile liver Peripheral edema JVD ↑ Pulmonary artery pressure Prominent a wave Prominent v wave RV hypertrophy & enlargement Tricuspid regurgitation ↑RAP & development of right sided heart failure
History • Generally asymptomatic at rest during the early stage. However, factors that ↑ HR such as fever, severe anemia, thyrotoxicosis, exercise, and Afib �dyspnea. • Systemic embolization may lead to stroke, renal failure, or MI. • Hoarseness : compression of the LRLN against the pulmonary artery by the enlarged LA. Also, compression of bronchi by the enlarged LA can cause persistent cough. Cough also occurs due to pul congestion • Hemoptysis may occur. • Palpitation • Chest pain (due to pul hypertension) • Oedema / Ascites (Right heart • Pregnant women with mild MS may become symptomatic failure) duringndtheir 2 trim (↑in blood vol ).
Physical examination • Presence of mitral facies (pinkish-purple patches on the cheeks) indicate chronic severe MS (reduced CO & vasoconstriction). JVD may be seen. • In pt with sinus rhythm, a prominent a wave : ↑ RA pressure from pul HTN & RVfailure. • A prominent v wave : is seen with TR.
Palpation • The arterial pulses are reduced in volume due to the decreased SV. • Pulses may be irregular in Afib. • Tapping apex beat that is not displaced. • Left parasternal heave - presence of RVH due to pulmonary HTN • A P 2 may be palpable in the 2 LICS.
Parasternal Heave • Grade 1 : visible but not palpable • Grade 2 : Visible & palpable and obliterable • Grade 3: Visible & palpable but not obliterable
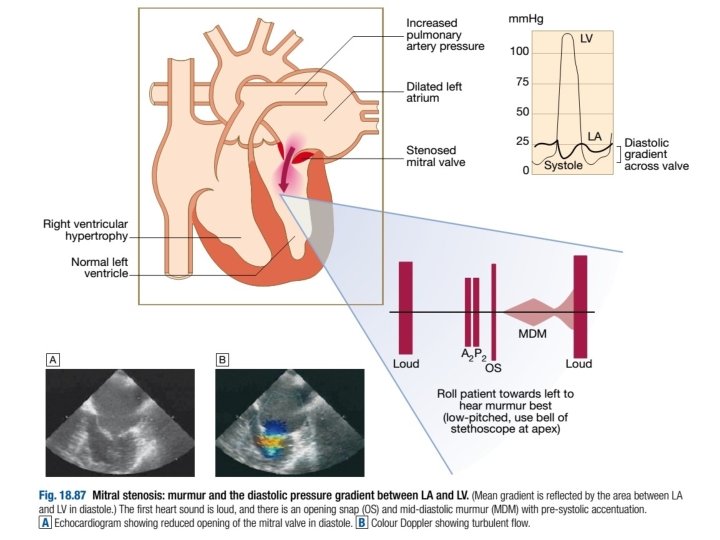
Cardiac auscultation: Heart sounds • The S 1 is accentuated because of a wide closing excursion of the mitral leaflets. • The degree of loudness of the S 1 depends on the pliability of the MV. • The intensity of the S 1 ↓ as the valve becomes more fibrotic, calcified, and thickened. • The S 2 is initially normal but, with the development of PHTN, P 2 becomes ↑ in intensity.
Cardiac auscultation: Opening snap • An OS of the MV is heard at the apex when the leaflets are still mobile. • The OS is due to the abrupt halt in leaflet motion in early diastole. • Note: The OS following S 2 may be mistaken for a split S 2 (OS is best appreciated at the apex, not the base. ) • As the MS progresses and LAP is ↑, the OS occurs earlier after S 2 or A 2. Thus, the shorter the A 2 -OS interval, the more severe the MS.
Cardiac auscultation: murmur • low-pitched diastolic rumble that is most prominent at the apex. • Although the intensity of the diastolic murmur does not correlate with the severity of the stenosis, the duration of the murmur is helpful since it reflects the transvalvular gradient and the duration of blood flow across the valve. • The ↑ in atrial pressure after atrial contraction, results in an increase in the loudness of the murmur, termed "presystolic accentuation".
MS: • The diastolic murmur and OS are diminished with inspiration, but augmented with expiration (in contrast to TS). With inspiration, the A 2 -OS interval widens. • Increasing venous return, eg, by lying the patient down and lifting the legs, augments the gradient; as a result, the diastolic murmur lengthens while the A 2 -OS intervals shorten. (Similar changes are seen in response to exercise. ) • In contrast, reducing venous return with amyl nitrate, the Valsalva maneuver, or standing after squatting shortens the murmur and lengthens the A 2 -OS interval.
Pathophysiology • The flow of blood from LA to LV is restricted and left atrial pressure rises, • Leading to pulmonary venous congestion and breathlessness. • There is dilatation and hypertrophy of the LA, • And left ventricular filling becomes more dependent on left atrial contraction.
Pathophysiology • Situation which increases heart rate or cardiac output like pregnancy and exercise – poorly tolerated – shortens diastole and produces a further rise in left atrial pressure • Atrial fibrillation - progressive dilatation of the LA • Pulmonary oedema - accompanying tachycardia and loss of atrial contraction • All these lead to marked haemodynamic deterioration
Clinical features: Signs • Atrial fibrillation • Mitral facies (calcification) • Auscultation – Loud first heart sound (S 1), – Opening snap: may be audible and move closer to S 2 with increase in severity – Mid-diastolic murmur: Turbulent flow produces characteristic low pitched – accentuated by exercise – inaudible if the valve is heavily calcified. • Crepitations, pulmonary oedema, effusions (raised pulmonary capillary pressure)
Signs • • • Face : Pulse : RV : Apex: Sounds: • Murmurs: Mitral fascies atrial fibrillation Heaving, sustained Localized, tapping Loud S 1, Loud P 2 (if pulmonary hypertension), opening snap Mid diastolic rumble at apex JMJ 8
Signs (Pulse) • Small volume pulse • Usually regular in early stages, • If the patient is in sinus rhythem • In severe disease, may develop atrial fibrillation • Irregularly irregular pulse JMJ 11
Mitral Stenosis: Physical Exam S 1 • • S 2 OS S 1 First heart sound (S 1) is accentuated & snapping Opening snap (OS) after aortic valve closure Low pitch diastolic rumble at the apex Pre-systolic accentuation (esp. if in sinus rhythm)
Signs (Face) • Severe mitral stenosis with pulmonary hypertension • Mitral fascies / malar rash • Bilateral • Cyanotic or dusky pink discolouration • Over the upper cheeks • Due to Vascular stasis JMJ 10
Signs (Jugular Veins) • If R heart failure develops • obvious distension of jugular veins • If pulmonary hypertension or tricuspid stenosis is present • ‘a’ Wave will be prominent JMJ 12
Signs (Palpation) • Tapping impulse felt parasternally on left side • Palpable 1 st heart sound • Combined with left ventricular backward displacement • Produced by an enlarging left ventricle • Sustained parasternal impulse • Due to R ventricular hypertrophy JMJ 13
Signs (Auscultation) • Loud 1 st heart sound – If the mitral valve is pliable – It will not occur in calcified mitral stenosis • Opening snap – Valve suddenly opens with the force of the increased L arterial pressure • Low pitched ‘rumbling’ mid diastolic murmur – Best heard with bell held lightly – At the apex with the patient lying on the left side JMJ 14
Signs (Auscultation) • If the patient is in sinus rhythm – Murmur becomes louder at the end of diastole – As a result of atrial contraction – (Pre- systolic accentuation) JMJ 15
How to determine the severity of mitral stenosis • Closeness of the opening snap to the 2 nd heart sound ∞ severe MS • Length of mid-diastolic murmur ∞ severity • As the valve cusps become immobile – Loud 1 st heart sound softens – Opening snap diasppears – When pulmonary hypertension occurs : P 2 intensity increase, mid diastolic murmur become quieter JMJ 17
How to determine the severity of mitral stenosis • Presence of pulmonary hypertension – Recognized by R/ ventricular heave & loud pulmonary component of 2 nd heart sound – And signs with R heart failure : Oedema, hepatomegaly – Graham Steell murmur JMJ 16
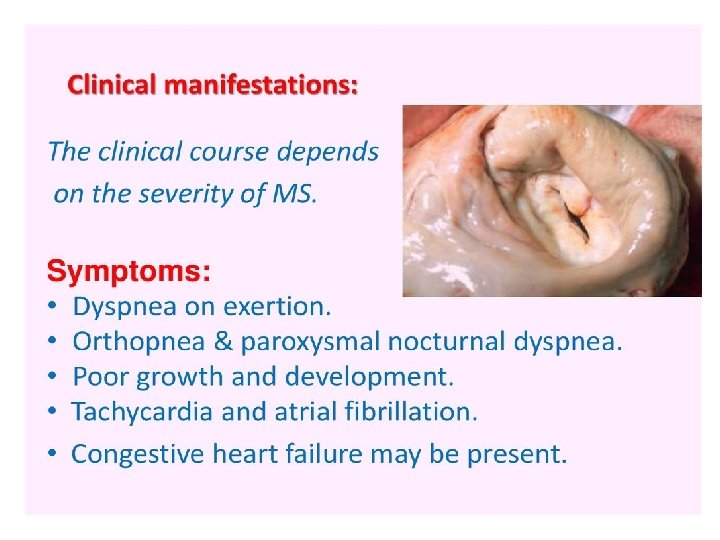
Symptoms Atrial fibrillation Pulmonary Hypertension • Palpitation • Systemic emboli • Dyspnoea • Pulmonary infections (Recurrent bronchitis) • Haemoptysis • Cough • R/ heart failure • Fatigue • Abdominal and lower limb swelling JMJ 7
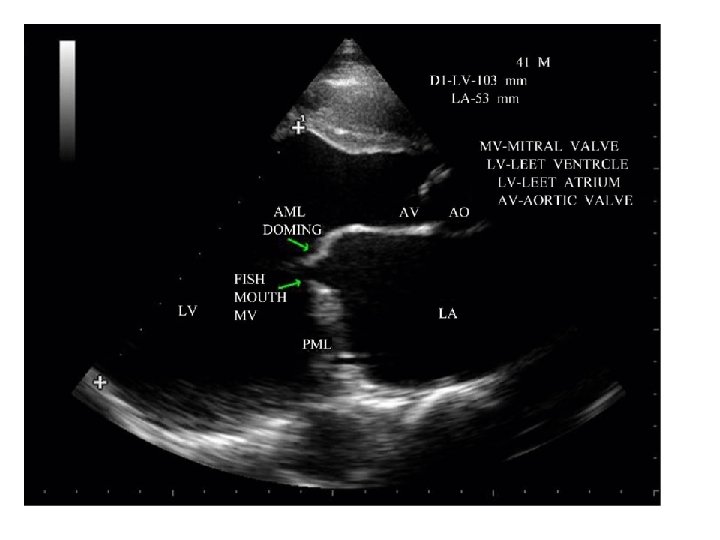
Investigations • Echo – – Thickened immobile cusps Reduced valve area Reduced rate of diastolic filling of LV Enlarged LA • Doppler echocardiography - definitive evaluation – Pressure gradient across mitral valve – Pulmonary artery pressure – Left ventricular function • Cardiac catheterisation - assessment of coexisting conditions. – Coronary artery disease – Mitral stenosis and regurgitation – Pulmonary artery pressure
Investigations • Chest X-ray • Electrocardiogram • Echocardiogram • Cardiac magnetic resonance • Cardiac catheterization JMJ 18
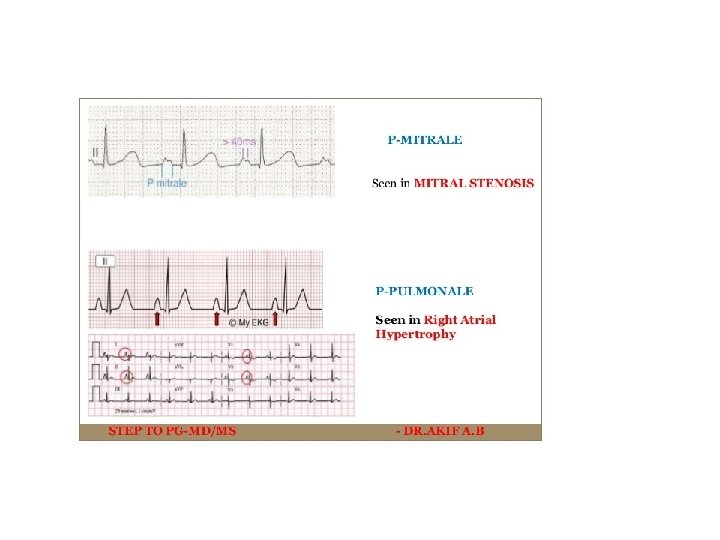
Investigations –ECG • Sinus rhythm in ECG shows a bifid P wave – Owing to delayed L/atrial activation • Atrial fibrillation may be present • ECG features of R/ventricular hypertrophy – Right axis deviation – Perhaps tall R wave in lead V 1 JMJ 20
Investigations –ECG JMJ 21
Investigations –ECG JMJ 22
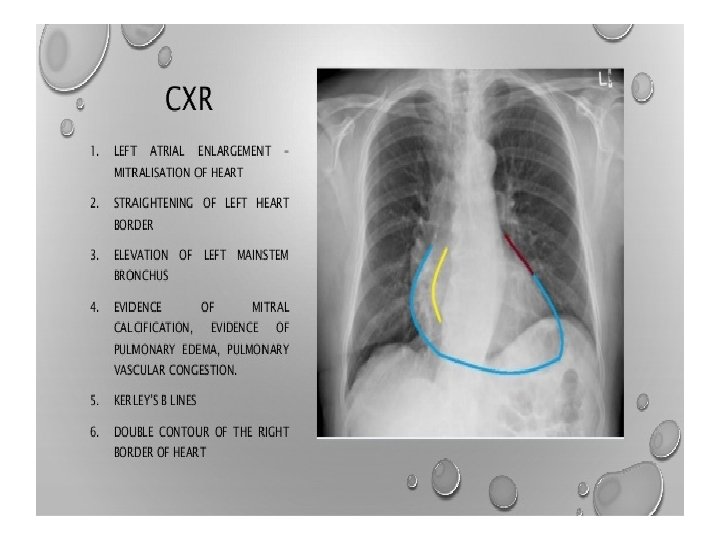
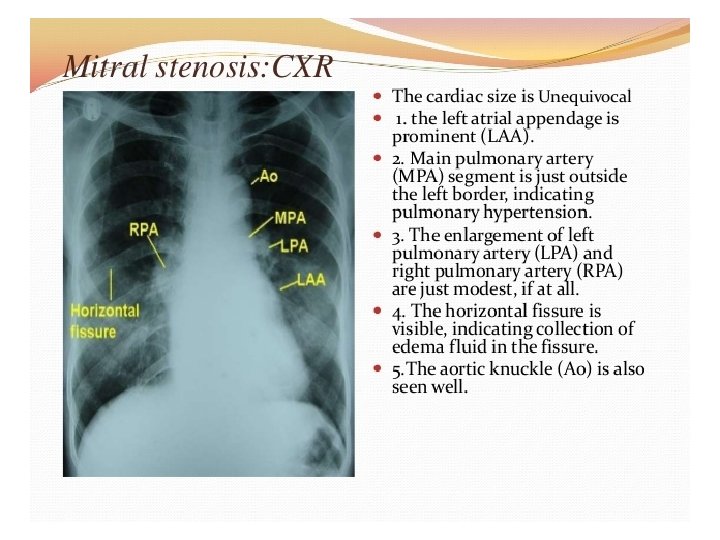
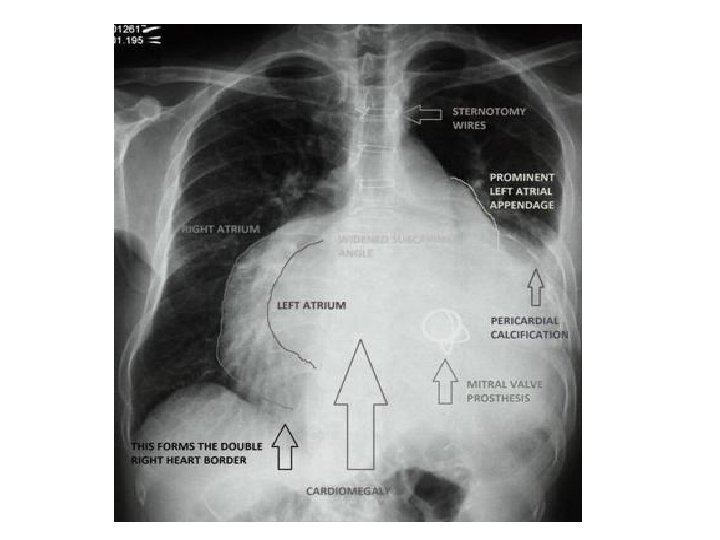
Investigations –X-ray • Small heart with an enlarged L/ atrium • Pulmonary venous hypertension • Calcified mitral valve– on penetrated or lateral view • Signs of pulmonary oedema or pulmonary hypertension JMJ 19
Mitral Stenosis. The left atrium is enlarged, displacing the left atrial appendage outward (red arrow). On the right side of the heart, a "double density" consisting of overlapping of the left atrium (black arrow) and right atrium (white arrow) is seen. The left main bronchus is elevated by the enlarged left atrium pushing it upwards (blue arrow).
Frontal radiograph of the chest shows a convexity in the region of theleft atrium indicating left atrial enlargement from mitral stenosis.
Investigations –Echocardiogram • Transthoracic echocardiography – To determine L/ R/ atrial and ventricular size – The sevirity of MS • Transoesophageal Echocardiography (TOE) – To detect the presence of L/ atrial thrombus JMJ 23
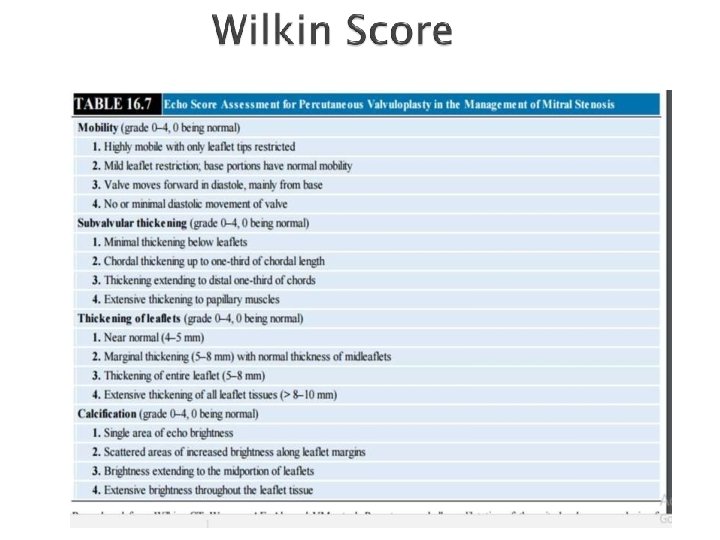
� 1. Score Higher than 11: should not undergo valvuloplasty � 2. Score of 9 -11: gray zone, suboptimal result � 3. Score less than 8 : optimal result
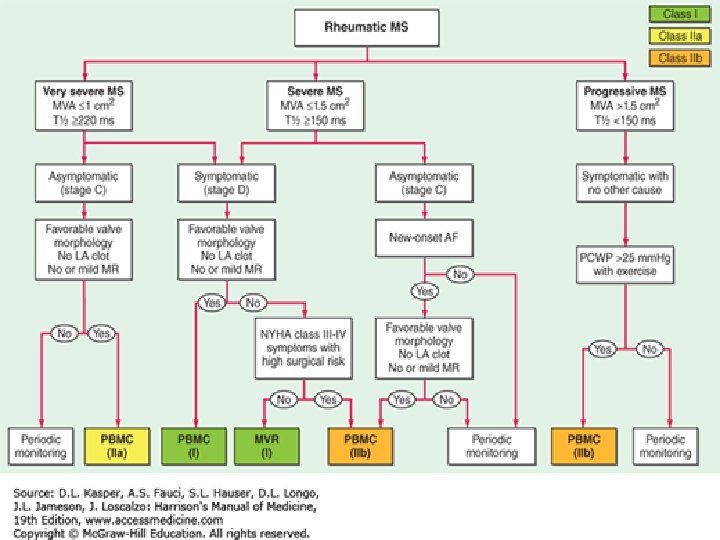
Grading Degree of mitral stenosis Mean gradient Mitral valve area Progressive mitral <5 mm. Hg stenosis >1. 5 cm 2 Severe mitral stenosis 5 – 10 mm. Hg 1. 0 – 1. 5 cm 2 Very severe mitral stenosis > 10 mm. Hg < 1. 0 cm 2
Treatment • Need no treatment other than prompt therapy of attacks of bronchitis • Early symptoms like dyspnea - diuretics • Onset of atrial fibrillation : digoxin, anticoagulants (to prevent atrial thrombus and systemic embolism) • If pulmonary hypertension or symptoms of pulmonary congestion : surgical therapy JMJ 24
Management • Patients with minor symptoms should be treated medically • Surgical Management: patient remains symptomatic despite medical treatment or if pulmonary hypertension develops – Balloon valvuloplasty, – Mitral valvotomy – Mitral valve replacement
Medical Management • Restrict Activity • CCF- Diuretis, Digoxin • Atrial fibrillation: ventricular rate control by β-blockers or rate-limiting calcium antagonists, digoxin, • Pulmonary congestion: diuretic therapy • Systemic embolism: anticoagulants • Antibiotic prophylaxis against infective endocarditis is no longer routinely recommended
Surgical Management • Mitral valvuloplasty: treatment of choice if specific criteria are fulfilled – Significant symptoms – Isolated mitral stenosis – No (or trivial) mitral regurgitation – Mobile, non-calcified valve/subvalve apparatus on ech – LA free of thrombus
Surgical Management • Valvoplasty: closed or open mitral valvotomy are acceptable alternatives • Valve replacement: substantial mitral reflux or if the valve is rigid and calcified • Regular follow up: at 1– 2 -yearly intervals because restenosis may occur
Treatment • Operative therapies – Trans-septal balloon valvotomy – Closed valvotomy – Open valvotomy – Mitral valve replacement JMJ 25
Mitral Balloon Valvotomy. A. After transseptal puncture, the deflated balloon catheter is advanced across the interatrial septum, then across the mitral valve and into the left ventricle. B. -D. The balloon is inflated stepwise within the mitral orifice
Treatment: Trans-septal balloon valvotomy JMJ 27
Treatment: Trans-septal balloon valvotomy • Catheter introduced into R atriam via femoral vein • Under local anasthesia • Inter atrial septum is punctured • Catheter enter into left atrium then to mitral valve • Balloon is inflated, briefly to split the valve commissures JMJ 26
Treatment: Trans-septal balloon valvotomy • Complications – Regurgitation may result • Contraindications – Heavy calcification – More than mild mitral regurgitation & thrombus in the L/atrium • TOE is done before this procedure JMJ 28
Treatment: Closed valvotomy • For the patients with – mobile, – non calcified and – non regurgitant mitral valves • Fused cusps forced apart by a dilator (introduced through the apex of L/ ventricle) • Cardiopulmonary bypass is not needed for this operation JMJ 29
Treatment: Open valvotomy • Often preferred to closed valvotomy • Cusps are carefully dissected apart under direct vision • Cardiopulmonary bypass is requied JMJ 30
Treatment: Mitral valve replacement • It is necessary if – Mitral regurgitation is present – Badly diseased or badly calcified stenotic valve, – Moderate or severe mitral stenosis & thrombus in L atrium despite anticoagulation • Artificial valve >20 yrs • Anticoagulants are necessary JMJ 31
Valve replacement
History Symptoms most commonly begin in the fourth decade, but MS often causes severe disability at earlier ages in developing nations. Principal symptoms are dyspnea and pulmonary edema precipitated by exertion, excitement, fever, anemia, tachycardia, pregnancy. .
Etiology • Most commonly rheumatic, although history of acute rheumatic fever is now uncommon; • Rare causes include congenital MS and calcification of the mitral annulus with extension onto the leaflets.
Clinical Features Symptoms Fatigue, exercise intolerance Low cardiac output Oedema/ascites Right heart failure Dyspnoea Pulmonary congestion Cough Pulmonary congestion Haemoptysis Pulmonary congestion, pulmonary embolism Palpitations Atrial fibrillation Chest pains Pulmonary hypertension Thromboembolic complications Stroke, ischaemic limb Paroxysmal nocturnal dyspnoea Orthopnoea
Signs Atrial fibrillation Mitral fascies Crepitations, pulmonary oedema/congestion, effusions ↑ Pulmonary capillary pressure HEART SOUND: Loud S 1 + opening snap Mid-diastolic murmur RV heave Loud P 2 Pulmonary hypertension
Physical Examination Right ventricular lift; palpable S 1; opening snap (OS) follows A 2 by 0. 06– 0. 12 s; OS–A 2 interval inversely proportional to severity of obstruction. Diastolic rumbling murmur with presystolic accentuation when in sinus rhythm. Duration of murmur correlates with severity of obstruction.
Diagnosis ECG Tall R-waves (V 1 -V 3) RV hypertrophy P mitrale or atrial fibrillation Imaging X-ray (chest) Enlarged LA & appendage Signs of pulmonary venous congestion Echocardiography Thickened immobile cusps Reduced valve area Enlarged LA ↓ LV diastolic filling Doppler (DEFINITIVE) Pressure gradient across mitral valve Pulmonary artery pressure Left ventricular function Cardiac catheterisation
• At-risk pts should receive prophylaxis for recurrent rheumatic fever (penicillin V 250– 500 mg PO bid or benzathine penicillin G 1– 2 M units IM monthly). • In the presence of dyspnea, sodium restriction and oral diuretic therapy beta blockers, rate-limiting calcium channel antagonists (i. e. , verapamil or diltiazem), or digoxin to slow ventricular rate in AF. • Warfarin (with target INR 2. 0– 3. 0) for pts with AF or history of thromoembolism • . For AF of recent onset, consider conversion (chemical or electrical) to sinus rhythm, ideally after ≥ 3 weeks of anticoagulation. • Mitral valvotomy in the presence of symptoms and mitral orifice ≤ ~1. 5 cm 2. • In uncomplicated MS, percutaneous balloon valvuloplasty is the
Surgical Management Baon valvuloplasty Indications: Significant symptoms Isolated mitral stenosis No/trivial mitral regurgitation Mobile, non-calcified valve/sub-valve apparatus on echo LA free of thrombus
Complications Hemoptysis, pulmonary embolism, pulmonary infection, systemic embolization; endocarditis is uncommon in pure MS. Laboratory ECG Typically shows atrial fibrillation (AF) or left atrial (LA) enlargement when sinus rhythm is present. Right-axis deviation and RV hypertrophy in the presence of pulmonary hypertension. CXR Shows LA and RV enlargement and Kerley B lines. Echocardiogram Most useful noninvasive test; shows reduced separation, calcification and thickening of valve leaflets and subvalvular apparatus, and LA enlargement. Doppler flow recordings provide estimation of transvalvular gradient, mitral valve area, and degree of pulmonary
JMJ 32
JMJ 33