New Paradigms for the Prevention of Cardiovascular Disease




 Small Dense LDL")

 This")
 Apolipoprotein NONPOLAR LIPID CORE POLAR SURFACE COAT Cholesterol Ester")
 LDL particle elevations common and")
 0. 95 IDL 1. 006 1. 02 1. 06 1.")

 superior to LDL Cholesterol Over 240 NMR related")


 versus LDL Cholesterol (LDL-C) 1. Even in")







")


 20")
 can be")




 LDL-C in Relation to Number of Metabolic Syndrome Components in Framingham")
 LDL Subclasses According to Presence of Components of the Metabolic Syndrome")




")

![Treatment Considerations Combination therapy (statin + other agent[s]) may be necessary to achieve both](https://slidetodoc.com/presentation_image_h/a94dcdd2e9bb1a5e2cf31c8149a357a4/image-40.jpg "Treatment Considerations Combination therapy (statin + other agent[s]) may be necessary to achieve both")
 § Isolated lipid")
 Cardiospecific inflammatory marker")





 Risk")


")
? l An atherogenic lipoprotein containing apo(a) and apo. B. l 20")
 – NHLBI Recommendations 1. It is essential that Lp(a) assays used in clinical")
 – NHLBI Recommendations 4. 5. 6. Lp(a) screening in the general population is")
 Testing May Be Useful Intermediate-risk individuals for better risk")
 F Niacin and estrogen reduce Lp(a) levels F")








- Slides: 66
New Paradigms for the Prevention of Cardiovascular Disease Tara Dall, MD Advanced Lipidology Delafield, Wisconsin Assistant Clinical Professor Medical College of WI Diplomate, American Board of Clinical Lipidology www. advlip. com
Disclosures F Speakers Bureau: Abbott, Astra. Zeneca, Takeda, Glaxo. Smith. Kline, Liposcience F Research support: none
Meet Barb age 55 Body for Life Champion • • • Picture perfect Health Normal lipid panel Normal BP, no identifiable heart disease risk factors
Barb Suffered a Massive Heart Attack at age 59 • • But she had “Normal Cholesterol”, Normal BP, no traditional heart disease risk factors Was there any additional testing that would have identified her as high risk?
Emerging Risk Markers • • Apo B LDL Particle Concentration (NMR) Small Dense LDL P hs. CRP Lp. PLA 2 (PLAC) Vitamin D deficiency Lipoprotein (a) Myeloperoxidase (MPO)
So Why Is LDL So Important in CVD? Gradient driven process…LDL Particles invade the arterial wall Ì Oxidative Ì Foam Modification Cell Formation Ì Atherosclerosis The higher the number of LDL particles (LDL-P), the greater the risk for CHD. 2 Fredrickson et al. NEJM 1967; 276: 148
LDL Cholesterol Is Not LDL!! Apo B This is an LDL particle (LDL-P) This is LDL Cholesterol (LDL-C) POLAR SURFACE COAT Phospholipid Free cholesterol NONPOLAR LIPID CORE Cholesterol Ester Triglyceride A convenient analytic surrogate of LDL since 1972
Lipoprotein Particle Structure (VLDL, HDL) Apolipoprotein NONPOLAR LIPID CORE POLAR SURFACE COAT Cholesterol Ester Triglyceride Phospholipid Free cholesterol Apolipoprotein The amount of cholesterol per particle varies from person to person, so LDL-C and HDL-C cannot give accurate “counts” of LDL and HDL particles.
Questions of the Day 1. Are unrecognized (and under-treated) LDL particle elevations common and significant contributors to the residual risk of many patients with “acceptable” levels of LDL-C? 2. When cholesterol (LDL-C, non HDL-C) and particle number (LDL-P) measures of LDL quantity are discordant (esp. diabetes, metabolic syndrome), which is most predictive of observed cardiovascular risk? 3. Is LDL-P is a more sensitive indicator of low risk than LDL-C or non HDL-C? 4. Are achievement of LDL-P treatment goals superior to LDL-C or non HDL-C values to indicate a the patient has achieved adequate LDL reduction? 5. Does LDL size (“quality”) contribute independently to risk once LDL particle number is taken into account? 6. What therapies lower LDL-P?
Lipoprotein Subcases Density (g/ml) 0. 95 IDL 1. 006 1. 02 1. 06 1. 10 Chylomicrons VLDL Chylomicron Remnants LDL HDL 2 Lp(a) HDL 3 Apo B = non HDL-C 1. 20 5 10 20 40 60 Diameter (nm) 80 1000
Measures of Atherogenic Lipoproteins Non HDL~ Apo B = LDL Particle Concentration >90 % Apo B is on LDL (exception Type III dyslipoproteinemia)
Weight of Evidence: LDL Particles (NMR) superior to LDL Cholesterol Over 240 NMR related papers published to Date
Evidence Supporting Apo B over LDL-C: Prospective Epidemiologic Studies & Placebo Wing of Major Statin Trials QCVS-13: Quebec Cardiovascular Study 13 year follow up THROMBO MS Thrombogenic Factors & Recurrent Coronary Events Metabolic Synd LIPID Long-term Intervention with Pravastatin in Ischemic Disease AFCAPS/Tex. CAPS Air Force Texas Coronary Atherosclerosis Prevention Study 4 S Scandinavian Simvastatin Survival Study Womens HS Women’s Heart Study THROMBO Thrombogenic Factors & Recurrent Coronary Events NPHS Northwick Park Heart Study AMORIS Apolipoprotein-related Mortality Risk QCVS-5 Quebec Cardiovascular Study 5 year follow up Sniderman A D& Marcovina SM. Clin Lab Med 26 (2006) 733– 750
Evidence Supporting Apo B over Non HDL-C: Prospective Epidemiologic Studies & Placebo Wing of Major Statin Trials Apo. B Superior as a Predictor Carotid IMT CMS HHMS AMORIS Carotid Intimomedial Thickness Studies (4) Casale Monferrator Study Harvard healthy Men Study Apolipoprotein-related Mortality Risk Equal Predictors of Risk Womens HS J-DM Women’s Heart Study Jiang Diabetes Mellitus Sniderman A D& Marcovina SM. Clin Lab Med 26 (2006) 733– 750
Associations of LDL Particle Number (Apo. B) versus LDL Cholesterol (LDL-C) 1. Even in high TG patients, more than 90% of total plasma apo. B is associated with LDL particles, except in type III hyperlipidemia [1, 2] 2. LDL particle number (Apo. B) is a superior predictor of CHD risk versus LDL-C in: • Prospective epidemiologic trials [312] • In assessing residual risk on statin or fibrate therapy in intervention trials [13 -17]. 3. LDL particle number (Apo. B) is a superior predictor of CHD risk versus non HDL-C: • Prospective epidemiologic trials [8, 11, 18] • In assessing residual risk on statin or fibrate therapy in intervention trials [13 -15, ]. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. Atherosclerosis. 1991; 89: 109 -16. Clin Chem Acta. 1978; 82: 151 -60. Circulation. 1996; 94: 273 -8. Circulation. 1999; 99: 2517 -22. Lancet. 2001; 358: 2026 -33. Arterioscler Thromb Vasc Biol. 2002; 22: 1918 -23. AJC. 2005; 997 -1001. Diabetologica. 2006; 49: 937 -944. Arterioscler Thromb Vasc Biol. 2007; 27: 661 -670. JAMA. 2005; 294: 326 -33. J Lipid Res. 2007; 48: 2499 -2505. JAMA. 2007; 298: 776 -785. Circulation. 2000; 101: 477 -84. Circulation. 2002; 105: 1162 -9. Arterioscler Thromb Vasc Biol. 2000; 20: 2408 -2413. JACC. 1998; 32: 1648 -1656. Circulation. 2003; 107: 1733 -1737. Lancet. 2003; 361: 777 -780.
NMR Lipoprotein Analysis Lipoprotein subclasses of different size broadcast lipid NMR signals that are naturally distinguishable. The measured amplitudes of these signals provide subclass quantification. Otvos JD. Handbook of Lipoprotein Testing. AACC Press 2000
NMR Measures LDL Particle Number Not LDL Cholesterol Measured LDL-C 90 mg/d. L LDL particles 900 nmol/L LDL NMR Signals LDL particles 1600 nmol/L
Changing Face of Lipidology
1. 00 Framingham Heart Study Offspring Cohort 0. 98 0. 96 Low LDL-C n=1249 Probability of Event Free Survival 0. 94 Event-free survival among participants with lowdensity lipoprotein cholesterol (LDL-C) above or below the median. 0. 92 0. 90 0. 88 0. 86 Median values were 131 mg/d. L for LDL-C High LDL-C n=1251 0. 84 0. 82 How predictive is LDLC with respect to event -free survival? 0. 80 0. 78 0. 76 0. 74 0 2 4 6 8 10 Years of Follow-up 12 14 16 Cromwell W et al. J Clin Lipidol 2007; 1: 583 -592
1. 00 Framingham Heart Study Offspring Cohort 0. 98 0. 96 Event-free survival among participants with lowdensity lipoprotein cholesterol (LDL-C) above or below the median. Probability of Event Free Survival 0. 94 0. 92 High LDL-C n=284 0. 90 0. 88 Median values were 131 mg/d. L for LDL-C 0. 86 0. 84 0. 82 Low LDL-C n=282 0. 80 Additional Data 0. 78 0. 76 0. 74 0 2 4 6 8 10 Years of Follow-up 12 14 16 Cromwell W et al. J Clin Lipidol 2007; 1: 583 -592
Framingham Heart Study Offspring Cohort 1. 00 0. 98 Low LDL-C n=1249 0. 94 Probability of Event Free Survival Event-free survival among participants with low-density lipoprotein cholesterol (LDL-C) and LDL particle number (LDL-P) above or below the median. Low LDL-P 0. 96 Low LDL-P 0. 92 Median values were 131 mg/d. L for LDL-C and 1414 nmol/L for LDL-P. High LDL-C n=284 0. 90 0. 88 0. 86 Significant # of LDL-C / CV-risk disconnects LDL-P was strongly associated with increased CVD risk in both men and women (p<0. 0001) High LDL-P High LDL-C n=1251 0. 84 High LDL-P 0. 82 Low LDL-C n=282 ? Explanation Particle number (LDL-P) 0. 80 0. 78 0. 76 LDL-P was approximately twice as strongly related to CVD incidence as LDL-C is the key risk factor 0. 74 0 2 4 6 8 10 Years of Follow-up 12 14 16 Cromwell W et al. J Clin Lipidol 2007; 1: 583 -592
Incidence CHD Events at Alternative Measures of Lipoprotein Concentrations Quartile 1 Framingham Offspring Study* (n=3, 066) * Adjusted for age and gender Cromwell WC, et al. J Clin Lipidology. 2007; 1(6): 583 -592.
Carotid Atherosclerosis in MESA (adjusted for age, sex, race, smoking, diabetes, TG, and HDLc) Carotid IMT (microns) Quartile 1: LDLc <100 mg/d. L (n=1, 425) n=32 Ptrend = 0. 006 n=352 n=153 n=888 Q 1 Q 2 Q 3 Q 4 LDL Particle Number Mora et al, AHA/ADA Metabolic Syndrome Meeting, May 2006
LDL Particle Number is Highly Heterogeneous Among Patients with Type 2 Diabetes Mellitus at LDL Cholesterol Target Goal <100 mg/d. L W. C. Cromwell and J. D. Otvos American Journal of Cardiology 2006; 98: 15991602
LDL Cholesterol and LDL Particle Numbers in T 2 DM Patients with LDL-C < 100 mg/d. L (n=2, 355) 5 th 37% (n=870) 20 th 50 th 80 th percentile 63% (n=1485) LDL-C Percent of Subjects 70 7% (n=162) 100 31% (n=741) 130 38% (n=891) 160 (mg/d. L) 16% (n=383) Percent 8% (n=178) 24% of LDL-P Subjects 700 1000 1300 1600 (nmol/L) Am J Cardiol. 2006; 98: 1599 -1602
LDL Particle Number Distribution in T 2 DM Subjects 5 th 1% (n=19) 20 th 24% (n=364) 50 th 43% (n=631) 80 th 21% (n=307) percentile 11% (n=163) LDL-C 71 -99 mg/d. L 75% Percent of Subjects (n=1, 484) 700 16% (n=147) 1000 43% (n=377) 1300 30% (n=260) 1600 (nmol/L) 9% (n=76) 2% (n=15) 41% Percent LDL-C of < 70 mg/d. L Subjects (n=871) 700 1000 1300 1600 (nmol/L) Am J Cardiol. 2006; 98: 1599 -1602
Relationship of Alternate Measures of LDL Quantity 1. Low Density Lipoprotein (LDL) can be quantified by cholesterol (LDL-C) or particle number (LDL particle number) tests. § Cholesterol content per particle is highly variable § Measuring cholesterol content does not equal particle number § Alternate measures of LDL quantity (LDL-C versus LDL particle number) are highly correlated, but also highly discordant 2. The greatest discordance between cholesterol and particle measures of LDL quantity is noted in patients with: § Metabolic Syndrome § Insulin Resistance § Type 2 Diabetes Mellitus § High Triglycerides or Low HDL-C
Small LDL Particles Contain Less Cholesterol Than Large LDL Particles Up to 70% More Particles 100 mg/d. L Large LDL Small LDL Cholesterol Balance But they also have more particles = more Apo B
Even LDL Particles of the Same Size Can Differ in Cholesterol Content Up to 40% More Particles 100 mg/d. L Normal Cholesterol Per Particle Less Cholesterol Per Particle Cholesterol Balance
Relations of LDL Particles and LDL Cholesterol to Levels of HDL Cholesterol and Triglycerides Otvos et al. , Amer J Cardiol 2002; 90: 22 i-29 i.
The Metabolic Syndrome Clinical Identification Diagnosis is established when 3 of these risk factors are present. Risk Factor Defining Level Abdominal obesity (Waist circumference) Men Women TG HDL-C >102 cm (>40 in) >88 cm (>35 in) Men Women Blood pressure Fasting glucose <40 mg/d. L <50 mg/d. L 130/ 85 mm Hg 100 mg/d. L 150 mg/d. L 15 - Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATPIII). Revised Circulation 2005
LDL-C (mg/d. L) LDL-C in Relation to Number of Metabolic Syndrome Components in Framingham Men 0 1 N=286 N=407 2 N=355 3 N=233 4 N=113 5 N=30
LDL Particles (nmol/L) LDL Subclasses According to Presence of Components of the Metabolic Syndrome in Framingham Men N=286 N=407 N=355 N=233 N=113 N=30 Circulation. 2006; 113: 20 -29
ADA and ACC Consensus Statement on Lipoprotein Management in Patients with Cardiometabolic Risk Treatment Goals Highest-risk patients, including those with 1) known CVD or 2) Diabetes plus one or more additional CVD risk factor High-risk patients, including those with 1) no diabetes or known clinical CVD but 2 or more additional major CVD risk factors or 2) Diabetes but no other CVD risk factors LDL-C Non-HDL-C Apo. B (mg/d. L) < 70 < 100 < 80 < 100 < 130 < 90 Brunzell JD, Davidson M, Furberg CD et al. Diabetes Care 2008; 31: 811 -822
Canadian Medical Association Recommendations for Management of Dyslipidemia F F Apo B has been standardized and most labs have the equipment to measure it Population levels (Canadian) • • • 90 mg/d. L 20 th percentile 105 mg/d. L 50 th percentile 120 mg/d. L 75 th percentile Genest J et al. CMAJ 2003; 168: 921 -924
Canadian. Target Levels Risk Level Initiate treatment if: Primary LDL-C High Consider treatment in all patients <2 mmol/L CAD, PVD Or ↓ 50% LDL-C Atherosclerosis Most Pts with Diabetes FRS ≥ 20% Class I Level A A RRS ≥ 20% Primary Alternate Apo. B<0. 80 Class I Level A A Moderate (strive towards ) FRS 10 -19% LDL-C>3. 5 mmol/L TC/HDL >5. 0 hs. CRP >2 men 50+, women 60+ Family history and hs. CRP modulate risk <2 mmol/L Or ↓ 50% LDL-C Apo. B<0. 80 Class AIIA Level A Class. A IIA Level A Low FRS<10% ↓ 50% LDL-C>5. 0 mmol/L A
Clinical Cutpoints for LDL Percentile: 20 th 50 th 80 th Optimal High LDL Cholesterol Framingham Offspring 70 MESA 100 130 160 190 220 250 mg/d. L LDL Particle Number 700 1000 1300 1600 1900 Percent of Subjects 2200 2500 nmol/L
Population Equivalent Cutpoints for Alternate LDL Measures (LDL-C, Measured Apo B and NMR LDL-P) Biomarker Population LDL-C (mg/d. L) Measured Apo B (mg/d. L) Percentile Equivalent Concentration < 5 th 20 th 50 th 80 th Framingham 1 < 70 100 130 160 Framingham 1 < 60 80 100 120 Framingham 1 < 850 1100 1400 1800 MESA 2 < 700 1000 1300 1600 NMR LDL-P (nmol/L) 1 2 Contois, et al. Clinical Chemistry 2009; 55: 407 -419 Cromwell WC. Clinical Challenges in Lipid Disorders. Oxford: Clinical Publishing, 2008: 249 -259.
Treatments that Alter the Cholesterol Content of LDL Change LDLc and LDLp Differentially Cholesterol per particle decreases with: Cholesterol per particle increases with: • statins • fibrates • statin + ezetimibe • niacin • estrogen replacement therapy • glitazones • low fat, high carb diet • omega 3 FAs • exercise • low carb diet LDLc More LDLp More
Treatment Considerations Combination therapy (statin + other agent[s]) may be necessary to achieve both goals. Combination agents which increase LDL size (niacin or fibrates) generally lower LDL-P more than LDL-C.
Candidates for Quantitative Lipoprotein Testing Primary Prevention § High-risk history (family) § Isolated lipid abnormalities § High triglyceride § Low HDL cholesterol § Assess “residual risk” near NCEP values § Metabolic syndrome § Diabetes Secondary Prevention § Few or no modifiable risk factors § Assess “residual risk” near NCEP goal § Recurrent events § Diabetes § Metabolic syndrome
Lipoprotein Associated Phospholipase A 2 Lp. PLA 2 (PLAC test) Cardiospecific inflammatory marker
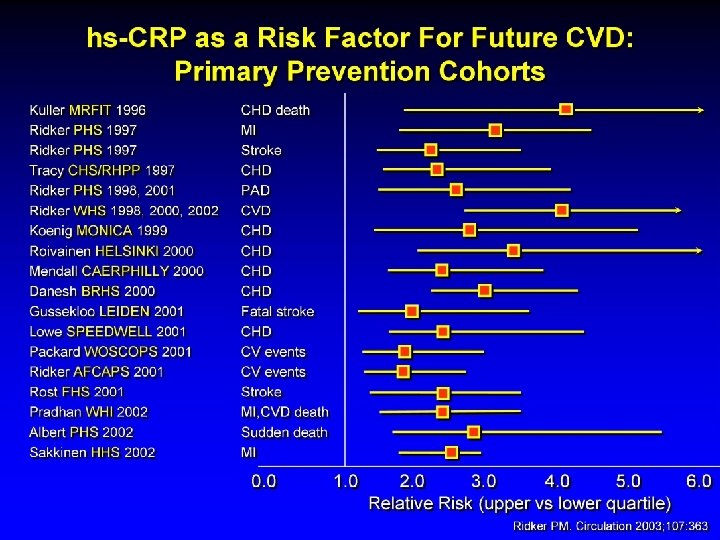
Elevated Lp-PLA 2 is Consistently Associated with a Doubling of Risk for Cardiovascular Disease Packard (WOSCOPS) - CHD 2000 Blake (WHS) - CHD 2001 Blankenberg (Athero. GENE) - CAD 2003 Ballantyne (ARIC) – CHD LDL < 130 2004 Winkler - CHD 2004 Oei (ROTTERDAM) - CHD 2005 Brilakis (Mayo Heart) - CHD 2005 Ballantyne (ARIC) - Stroke 2005 Oei (ROTTERDAM) - Stroke 2005 Winkler (LURIC) - CHD 2005 Khuseyinova (HELICOR) - CHD 2005 Koenig (KAROLA) - CVD 2005 Yang – Endothelial dysfunction 2006 Intermountain Heart - CHD 2006 Caslake (PROSPER) - CVD 2006 Jenny (CHS) - MI 2006 Daniels (Rancho Bernardo) - CHD 2006 Elkind (NOMAS) – Stroke 2006 O’Donoghue (PROVE IT) - CVD 2006 Corsetti (THROMBO) - CHD 2006 Gerber (Olmsted Cty) – Death S/P MI 2006 Sabatine (PEACE) - CVD 2006 0. 5 1 1. 5 2 2. 5 3 3. 5 4 4. 5
Lp-PLA 2 Predicts Major CV Events in CHD Patients: Mayo Heart Study 95% of patients with Lp-PLA 2 < 200 ng/ml were Event Free at 4 years Brilakis ES et al. Mayo Heart Study. Euro Heart J 2005
Case
C. F. 44 yr white male with Type I DM and normal Lipid profile Needs convincing to take a Statin LDL cholesterol 74
C. F. 44 yr IDDM Statin or No Statin? PMH hypothyroid Meds: Insulin, Ace. Inh, Synthroid Hg. Aic 8. 6 LDL-P 736 Lipoprotein (a) 24 mg/d. L Lp. PLA 2 347
Proposal for Clinical Use of Lp-PLA 2 as an Aid in Cardiovascular (CV) Risk Stratification Initial Risk Assessment and Physical Examination Low Risk § 0 -1 major risk factors § Low Framingham risk score, ten year risk: < 10% Moderate Risk § 2+ risk factors and ten year risk: 10 -20% OR High Risk § Established CHD OR § Age 65 or older OR § CHD risk equivalent (DM, stroke, PAD, ESRD) OR § HTN > 135/85 mm. Hg OR § ABI <. 9 OR § Smoker OR § >50% stenosis on carotid ultrasound OR § FB Glucose > 100 mg/dl § hs-CRP > 3. 0 mg/L Very High Risk § Established CVD PLUS § 3 risk factors OR § Poorly controlled severe risk factors OR § Metabolic syndrome OR § Acute CVS 1 year follow-up If the PLAC test is > 235 ng/ml then it would be reasonable to treat LDL to the target for the next higher risk category; either 100 mg/dl or 70 mg/dl, respectively. Intensify treatment of non-lipid risk factors as well. 2006 CV Risk Stratification Panel: Davidson MH, Braun LT, Corson MA, Gorelick P
Lipid Lowering Medications Shown to Reduce CV Events also Lower Lp. PLA 2 Percent reduction in Lp-PLA 2 Ezetimibe 1 Average Fenofibrate 1, 3 Niacin Statin 1 -4 Omega 3 FA + statin 5 + statin 6 Statin Niacin Omega Added 3 FA To Statin Added To Statin 1. Saougos VG, et al. ATVB 2007: 27. 4. Muhlestein JB, et al. Am H Journal. 2006; 48: 396 -401. 2. Albert M, et al. Atherosclerosis 2005; 182: 193 -198. 5. Kuvin J, et al. Am J Cardiol. 2006. 3. Schaefer EJ, et al. Am J Cardiol. 2005; 95: 1025 -1032. 6. Schalwitz R, et al. ATVB Annual Mtg abstract 2007.
Patient Candidates for Lp-PLA 2 Testing 1. Intermediate risk persons with 1 -2 traditional risk factors, such as Metabolic Syndrome patients or hypertensives 2. High risk coronary risk equivalent patients, even if treated, to see if their plaque is still unstable 3. A “tie breaker” for borderline lipids, how aggressive should we be if LDL is 131 or HDL is 39? 4. A “tie breaker” for apparently healthy persons with borderline hypertension. Their risk for stroke may be 3. 5 to 6. 8 times higher than those with low blood pressure and low Lp-PLA 2. 5. When is the job done? That is, is the plaque stable?
Lipoprotein (a)
What Is Lipoprotein(a)? l An atherogenic lipoprotein containing apo(a) and apo. B. l 20 -30% of people have levels suggesting C-V risk. l Black subjects have Lp(a) normal range twice as high as white and Asiatic subjects. l Apo(a) sequence similar to plasminogen, and Lp(a) interferes with spontaneous thrombolysis. l Lp(a) levels highly genetic, resistant to diet and drug therapy, although niacin and oral estrogen may help. Apo(a) “LDL” -S-S-
Lp(a) – NHLBI Recommendations 1. It is essential that Lp(a) assays used in clinical and epidemiologic studies be validated for their ability to provide accurate values independently of the size of apo(a) in the samples. 2. The expression of Lp(a) values in terms of total Lp(a) mass (mg/d. L) should be abandoned as this reflects protein component of Lp(a) and not its lipid and carbohydrate content. 3. To correctly reflect the number of Lp(a) particles and to compare data from different studies, the values should be expressed in terms of nmol/L of Lp(a). Marcovina SM, et al. Clin Chem. 2003; 49: 1785 -1796.
Lp(a) – NHLBI Recommendations 4. 5. 6. Lp(a) screening in the general population is not recommended. Measurement of Lp(a) is recommended in individuals with an increased risk of CVD, particularly those with borderline LDL-C or high apo B. On the basis of currently available data, individuals with Lp(a) values exceeding the 75 th percentile are at increased risk for CVD. For Caucasians, based on the Framingham data, this corresponds to an Lp(a) value of > 75 nmol/L. If methods sensitive to apo(a) isoform size are used for risk assessment, samples with values > 50 nmol/L should be remeasured by referral laboratories using validated methods. Marcovina SM, et al. Clin Chem. 2003; 49: 1785 -1796.
Clinical Situations in Which Lp(a) Testing May Be Useful Intermediate-risk individuals for better risk stratification F Familial history of cardiovascular disease F Established coronary heart disease with a "normal" lipid profile F Hypercholesterlemia refractory to therapy F History of recurrent restenosis F
Effects of Lipid-Modulating Drugs on Lp(a) F Niacin and estrogen reduce Lp(a) levels F Apheresis reduces Lp(a) levels F No benefit from statins F No consistent benefit with fibrates, although studies are variable
hs. CRP
JUPITER Primary Trial Endpoint : MI, Stroke, UA/Revascularization, CV Death Placebo 251 / 8901 0. 08 HR 0. 56, 95% CI 0. 46 -0. 69 P < 0. 00001 0. 06 0. 04 - 44 % Rosuvastatin 142 / 8901 0. 00 0. 02 Cumulative Incidence Number Needed to Treat (NNT 5) = 25 0 1 2 Follow-up (years) Ridker et al, NEJM 2008; 359: 2195 -207 3 4
Drugs and CRP F Statins lower hs. CRP F Niaspan lower hs. CRP F Fibrates lower hs. CRP F Omega 3 Fatty Acids lower hs. CRP F Glitazones lower hs. CRP F Estrogen increases hs. CRP
All-Cause and Cardiovascular Mortality in 25 -Hydroxyvitamin D Quartiles Data from the Ludwigshafen Risk and Cardiovascular Health (LURIC) study Dobnig et al. Arch Intern Med 2008; 168: 1340 -1349.
All-Cause Mortality According CAD Status Determined by Coronary Angiography Dobnig et al. Arch Intern Med 2008; 168: 1340 -1349.
Could Barb’s Massive Heart Attack been prevented? No risk factors? Lets look at her NMR lipoprofile
LDL Particle Numbers LDL particle: 2148 nmol/L Optimal: <700 nmol/L LDL-P Small LDL-P Lipids LDL-C nmol/L Optimal Near or above optimal Borderline-high 2148 <1000 - 1299 HDL-C High Very High 1600 - 2000 >2000 nmol/L Optimal Moderate Borderline-high High 1522 <600 - 849 850 - 1200 <1200 mg/d. L Optimal 125 <100 Near or above Borderline-high optimal 101 -129 mg/d. L Vitamin D low 20 1300 - 1599 46 130 - 159 mg/d. L Triglycerides 78 High Very High 160 - 200 >200 Total Cholesterol mg/d. L 187 Subclass Particle Numbers VLDL Subclasses She appears to have had a risk factor after all P E R C E N T I L E LDL Subclasses HDL Subclasses 75 th 50 th 25 th Large Medium VLDL-P Small VLDL-P IDL-P Large LDL-P Small LDL-P Large HDL-P Medium HDL-P Small HDL-P
Maybe Not…. . But Lipoproteins certainly do