CARDIOVASCULAR DISEASE Dariush Abtahi MD Anesthesiologist Cardiovascular disease

CARDIOVASCULAR DISEASE Dariush Abtahi MD Anesthesiologist

Cardiovascular disease is the leading cause of death. Coronary artery disease, peripheral vascular disease, and risk for coronary artery disease increase operative risk.

Recent myocardial infarction, the presence of congestive heart failure, and aortic stenosis are the most common major risk factors.

CORONARY ARTERY DISEASE

In 40% of the adult patients who undergo surgery annually in the United States. Increased rates of morbidity and mortality when coronary artery disease is present.

Routine preoperative cardiac evaluation: physical examination evaluation of exercise tolerance cardiac symptoms ECG

The most common symptoms: shortness of breath with exercise in men and fatigue in women angina at rest orthopnea paroxysmal nocturnal dyspnea dizziness or fainting
 exercise stress testing transthoracic or transesophageal")
More specialized procedures: ambulatory ECG monitoring (Holter monitoring) exercise stress testing transthoracic or transesophageal echocardiography radionuclide ventriculography (determination of ejection fraction) dipyridamole-thallium scintigraphy cardiac catheterization angiography

More specialized procedures: NO MORE INFORMATION!

Patient History Patients can remain asymptomatic despite 50% to 70% stenosis of a major coronary artery.

CARDIAC RESERVE Limited exercise tolerance in the absence of significant pulmonary disease is the most striking evidence of decreased cardiac reserve.

Evidence of significant cardiac diseaseinability to: lie flat awakening from sleep with angina or shortness of breath angina at rest or with minimal exertion

If a patient can climb two to three flights of stairs without symptoms, cardiac reserve is probably adequate.

ANGINA PECTORIS Stable: no change for at least 60 days.

Unstable: chest pain or shortness of breath produced with less than normal activity or at rest, or lasting for increasingly longer periods Signal an impending myocardial infarction.
. 70% of ischemic episodes- 15% of acute myocardial infarctions!")
Silent myocardial ischemia (asymptomatic). 70% of ischemic episodes- 15% of acute myocardial infarctions!

Women and diabetics have a more frequent incidence of painless myocardial ischemia and infarctions.

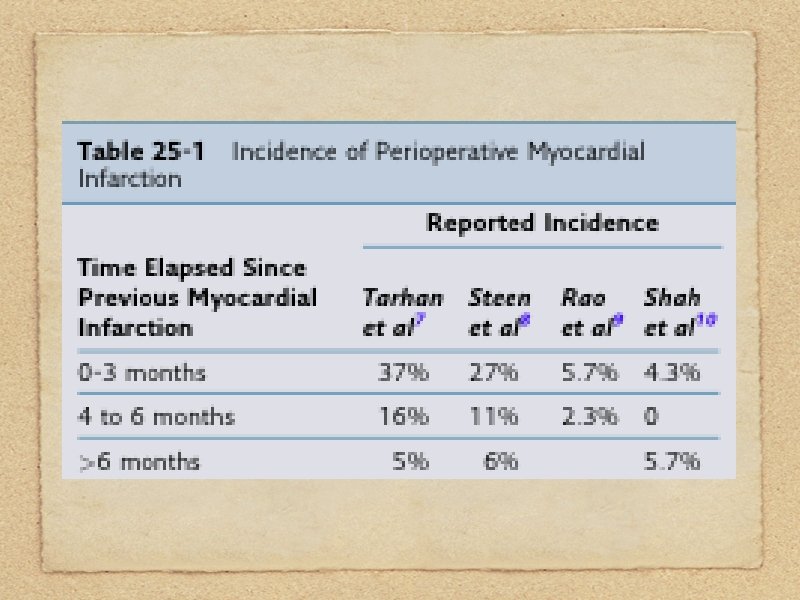
MYOCARDIAL INFARCTION The incidence of perioperative myocardial reinfarction does not stabilize at 5% to 6% until 6 months after the prior myocardial infarction.

Elective surgery, especially thoracic, upper abdominal, or other major procedures are delayed for a period of 2 to 6 months after a myocardial infarction.

After 6 months, the 5% to 6% incidence of myocardial reinfarction is about 50 times more frequent than the 0. 13%.

Most perioperative myocardial reinfarctions occur in the first 48 to 72 hours postoperatively.

Several factors influence the incidence of myocardial infarction in the perioperative period: Intra-thoracic or intra-abdominal operations lasting longer than 3 hours.

Decrease the risk: Intensive hemodynamic monitoring using an intra-arterial catheter Prompt pharmacologic intervention or fluid infusion to treat physiologic hemodynamic alterations

CURRENT MEDICATIONS Do Not Stop: beta-blockers, calcium channel blockers, nitrates, statins, or angiotensin-converting enzyme inhibitors in the perioperative period.
 myocardial ischemia (2) prior MI (3) cardiac hypertrophy (4)")
Electrocardiogram ECG examined for: (1) myocardial ischemia (2) prior MI (3) cardiac hypertrophy (4) abnormal cardiac rhythm (5) electrolyte abnormalities

The exercise ECG simulates events such as direct laryngoscopy, tracheal intubation, and surgical incision.

The resting ECG in the absence of angina pectoris may be normal despite extensive coronary artery disease.

Management of Anesthesia care for patients with known coronary artery disease, or two risk factors for coronary artery disease should begin as soon as the patient is identified as needing surgery.

Risk Factors: age older than or equal to 60 years hypertension diabetes significant smoking history hyperlipidemia

Avoid: persistent tachycardia systolic hypertension arterial hypoxemia diastolic hypotension

Maintaining heart rate and systemic blood pressure within 20% of the awake values is commonly recommended.

Monitoring with an intraarterial catheter facilitates the ability to maintain stable systemic blood pressures.

A single 1 -minute episode of myocardial ischemia detected by 1 mm ST-segment elevation or depression increases the risk of cardiac events tenfold and the risk for death twofold.

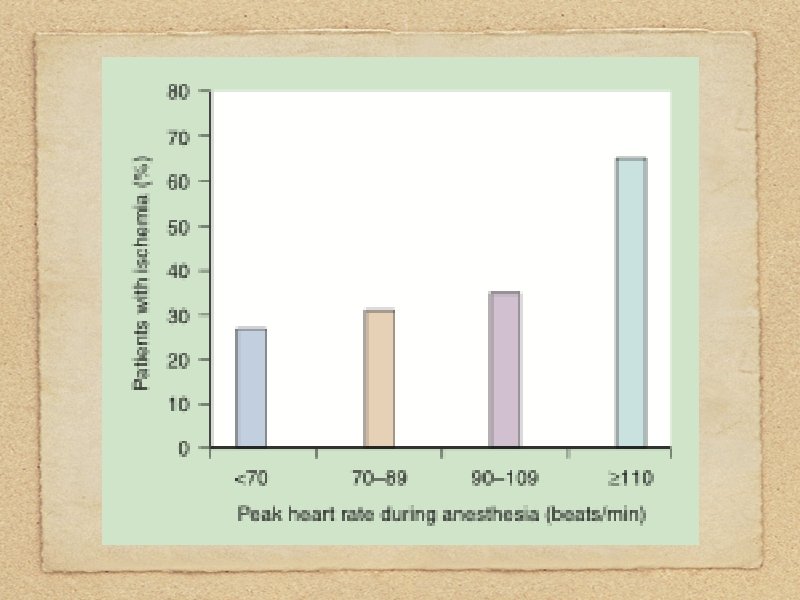
Tachycardia for 5 minutes above 120 beats/min in the postoperative period can increase the risk of death tenfold.

MONITORING Anticipation of problems and avoidance of potential disasters is a key component in successful anesthetic management in patients with cardiovascular disease. Prophylactic therapy and more extensive monitoring reduce risk.

Rapid changes in hemodynamics can quickly lead to cardiac arrest Monitoring can quickly identify those changes

When operations are completed, monitoring should be continued into the recovery room or intensive care unit (ICU).

Loss of a pulse oximeter signal: hypoxia inadequate arterial blood pressure

INDUCTION OF ANESTHESIA Preoperative anxiety can lead to preoperative myocardial ischemia. Patients should receive their routine medications except for oral hypoglycemic drugs.
. Propofol is popular,")
Etomidate is a popular anesthetic to induce anesthesia (limited hemodynamic effects). Propofol is popular, but the dose should be reduced to avoid hypotension with induction.

Myocardial ischemia may accompany the tachycardia and hypertension that results from the stimulation of direct laryngoscopy.

Adequate anesthesia and a brief duration of direct laryngoscopy is important in minimizing the magnitude of these circulatory changes.

MAINTENANCE OF ANESTHESIA Avoiding tachycardia with the use of long -acting beta-blockers is more important than anesthetic choice.

A regional anesthetic is an excellent technique in patients with coronary artery disease.

Decreases in systemic blood pressure associated with a regional anesthetic that are more than 20% of the pre-block value probably should be treated with an intravenous infusion of crystalloid solutions or a vasoconstrictor such as phenylephrine.

NEUROMUSCULAR BLOCKING DRUGS Cisatracurium do not evoke histamine release and associated decreases in systemic blood pressure, even with the rapid intravenous administration of large doses.

The systemic blood pressure lowering effects of atracurium are usually modest, especially if the drug is injected over 30 to 45 seconds to minimize the likelihood of drug-induced histamine release.

Pancuronium increases heart rate and systemic blood pressure, but these changes are usually less than 15% above pre-drug values, making this drug a possible choice for administration to patients with coronary artery disease.

Block can be safely antagonized with anticholinesterase drugs combined with an anticholinergic drug.

TREATMENT OF MYOCARDIAL ISCHEMIA Tachycardia: propranolol, esmolol. Excessive increases in systemic blood pressure: narcotics, inhaled agents, betablockers, nitroprusside.

Nitroglycerin: when myocardial ischemia is associated with a normal systemic blood pressure. Hypotension: phenylephrine, IV fluids.

Shivering on awakening! Postoperative pain relief!

Postoperative Care Postoperative care is based on: perioperative anti- ischemic agents (betablockers or clonidine, statins) analgesia sedation Intensive and continuous postoperative monitoring

VALVULAR HEART DISEASE

The net effect of valvular heart disease is interference with forward flow of blood from the heart into the systemic circulation.

Patients with valvular heart disease should receive appropriate antibiotics in the perioperative period for protection against infective endocarditis.

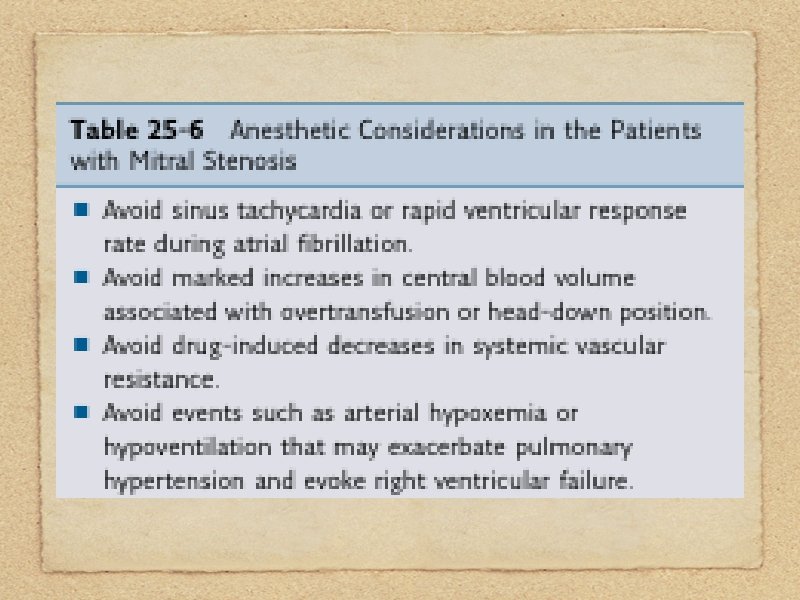
Mitral Stenosis Increase in left atrial and pulmonary venous pressure.
. More susceptible to")
Atrial fibrillation- systemic emboli. Chronic anticoagulation or anti-platelet therapy (or both). More susceptible to the ventilatory depressant effects of sedative drugssupplemental oxygen!

Tachycardia: atropine in reverse! Allowing the nondepolarizing neuromuscular blockade to be eliminated.

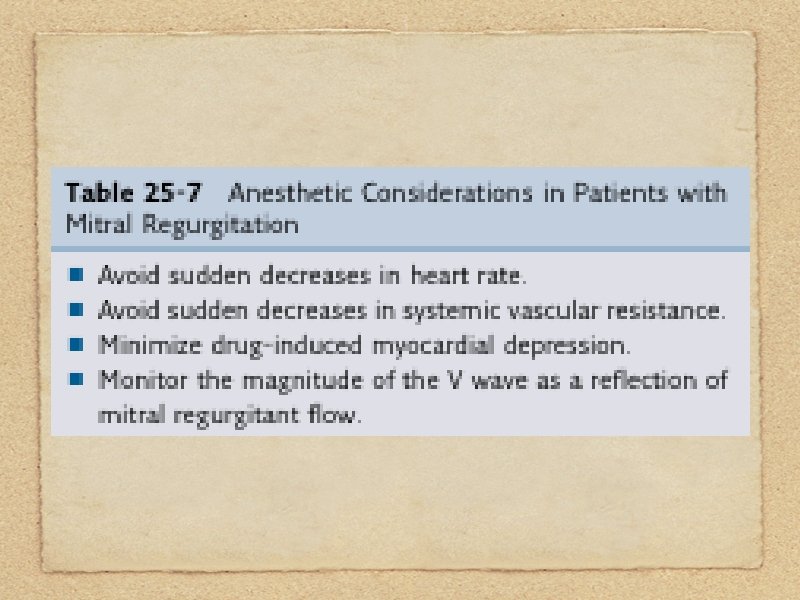
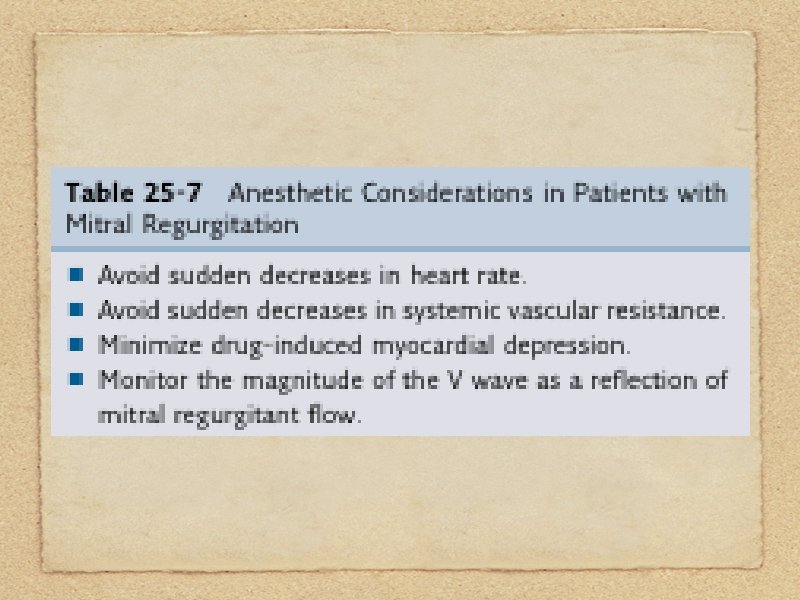
Mitral Regurgitation Back-flow of part of blood through the incompetent mitral valve back into the left atrium.

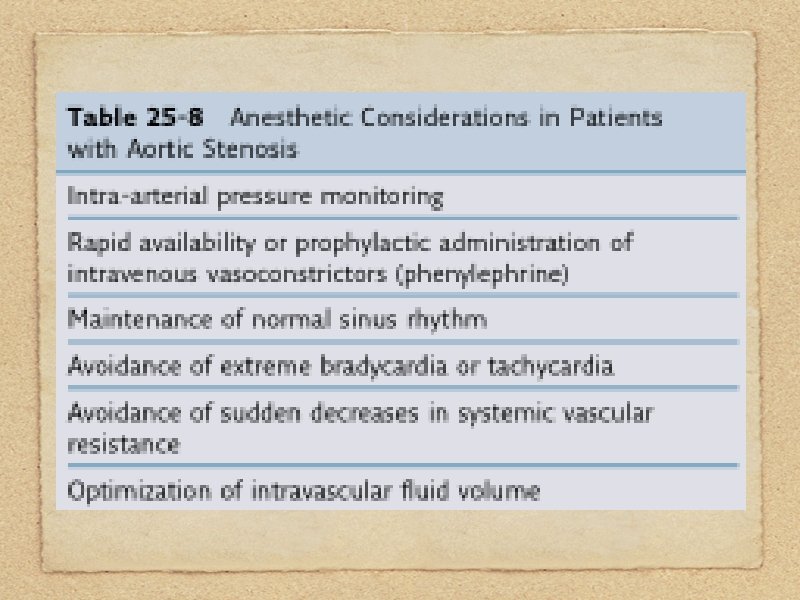
Aortic Stenosis Increased left ventricular systolic pressure to maintain the forward stroke volume through a narrowed aortic valve.

May be asymptomatic! It is important to listen for this cardiac murmur. Sudden death!

Aortic Regurgitation Decreased forward left ventricular stroke volume due to regurgitation of part of the ejected stroke volume from the aorta back into the left ventricle through an incompetent aortic valve.

Management of anesthesia in patients with aortic regurgitation is as described for patients with mitral regurgitation.

Mitral Valve Prolapse Abnormality of the mitral valve support structure.

Most patients are asymptomatic, emphasizing the usually benign course of this abnormality.
 sympathetic nervous system stimulation (2) decreased systemic vascular resistance (3) performance of")
Avoid: (1) sympathetic nervous system stimulation (2) decreased systemic vascular resistance (3) performance of surgery with patients in the head-up or sitting position.

ESSENTIAL HYPERTENSION

Essential hypertension: systolic blood pressure > 160 mm Hg or a diastolic blood pressure > 90 mm Hg independent of any known cause.

Treatment of essential hypertension decreases the incidence of stroke and congestive heart failure. Hypertension is a risk factor for coronary artery disease.

Management of anesthesia: preoperative evaluation of drug therapy and extent of the disease exaggerated systemic blood pressure responses-intraoperative stimulation

Preoperative Evaluation Adequacy of systemic blood pressure control Review of the antihypertensive drugs Antihypertensive drugs should be continued throughout the perioperative period.

The incidence of hypotension and evidence of myocardial ischemia on the ECG during the maintenance of anesthesia is increased in patients who remain hypertensive before the induction of anesthesia.

Induction of Anesthesia Any anesthetic is acceptable if used with appropriate dosing and careful monitoring. Etomidate or combinations of midazolam and fentanyl are frequently used.

Maximal attenuation of sympathetic nervous system responses should be attempted during direct laryngoscopy by administering anesthetics, intravenous opioids, and beta-blockers before attempting tracheal intubation.

In difficult airway: heart rate control is of prime importance selecting alternative approaches such as fiberoptic intubation.

Hypoxia, tachycardia, hypotension, hypertension, and myocardial ischemia must be avoided. An excessive concentration or dose of anesthetic drugs can produce hypotension, which is as undesirable as hypertension.

Limit the duration of direct laryngoscopy to less than 15 seconds if possible. Laryngotracheal lidocaine immediately before Intubation.

Maintenance of Anesthesia Adjust the concentrations of anesthetics so tachycardia and wide fluctuations in systemic blood pressure can be avoided.

Changes in surgical stimulation may lead to changes in blood pressure and heart rate. Heart rates above 120 beats/min increase mortality rate.

Continuous IV infusions of nitroprusside, nitroglycerine, or esmolol can be used to maintain normotension during the intraoperative period.

Postoperative Management If hypertension persists despite betablockers and adequate analgesia: continuous IV infusion of nitroprusside, nitroglycerin, or intermittent injections of hydralazine (5 to 20 mg IV).


CONGESTIVE HEART FAILURE

Elective surgery should not be performed on patients with congestive heart failure unless optimally treated.

Etomidate may be useful for the induction. Small concentrations of volatile anesthetics. In the presence of severe congestive heart failure, the use of opioids in large doses in combination with benzodiazepines (midazolam).

Positive-pressure ventilation of the lungs may be beneficial. The resumption of negative intrathoracic pressures with spontaneous ventilation following extubation can lead to worsening heart failure.

Regional anesthesia should be considered for patients with congestive heart failure requiring peripheral or minor surgery.


ANEURYSMS OF THE AORTA

Most patients are hypertensive. A dissecting aneurysm: allows blood to enter and penetrate between the walls of the vessel, producing a false lumen.

Endovascular aneurysm repair is less invasive and may require only regional anesthesia. Open procedures require general anesthesia.

Monitoring: intra-arterial pressures pulmonary arterial pressure transesophageal echocardiography
, nitroprusside, or nitroglycerine (for hypertension).")
Intraoperatively: continuous IV infusion of phenylephrine (for hypotension), nitroprusside, or nitroglycerine (for hypertension).

Preoperative hydration and prompt intraoperative replacement of blood loss. Diuresis is often facilitated by intraoperative administration of a diuretic (mannitol, furosemide, or both) with or without dopamine.

Hypotension can accompany unclamping of the abdominal aorta.

Systemic blood pressure decreases can be minimized by infusing intravenous fluids before removal of the aortic cross-clamp.

Gradual removal of the aortic cross-clamp minimizes decreases in systemic blood pressure by allowing time for return of pooled venous blood to the circulation.
- Slides: 107