Neoplasia lecture 3 Dr Heyam Awad FRCPath 2016






")



































- Slides: 48
Neoplasia lecture 3 Dr Heyam Awad FRCPath 2016
Topics to be covered • Dysplasia and carcinoma in situ • Cancer stem cells • Epidemiology of neoplasia
Dysplasia and carcinoma in situ • Dysplasia = from Greek word Bad or difficult Formation or division
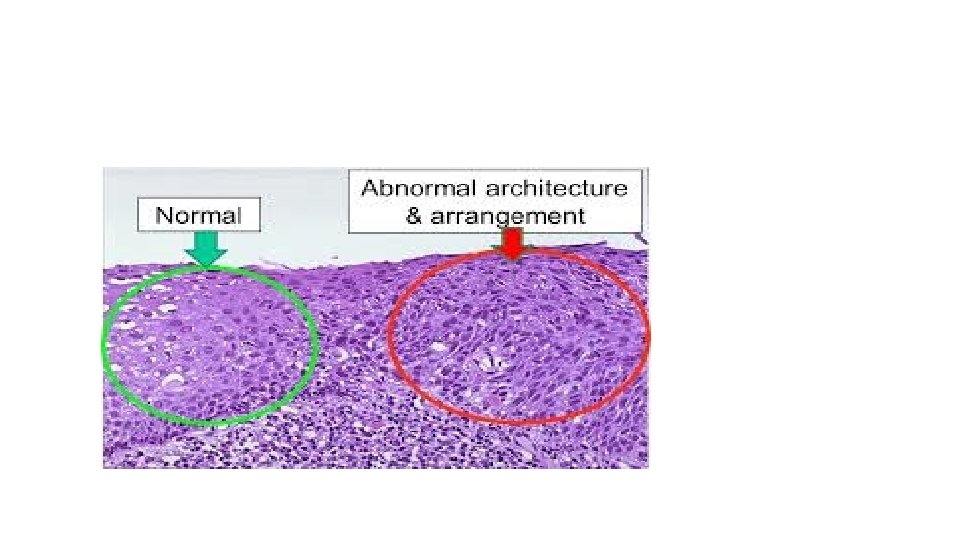
dysplasia • Disordered but non-neoplastic proliferation. • Loss of uniformity of individual cells and in their architectural orientation • Expansion of immature cells • Seen mainly in epithelial lesions
Disorganized proliferation= polarity lost = arrangement disturbed
Dysplasia/ microscopically • Loss of orientation • Pleomorphis • Large cells • Hyperchromatic nuclei • More mitoses than normal • Mitosis in an abnormal location ( normal location is at the basal layers of epithelium… abnormal: mitosis seen in more superficial layers)
Dysplasia. Note the intact basement membrane (no invasion)
Dysplasia in glandular epithelium
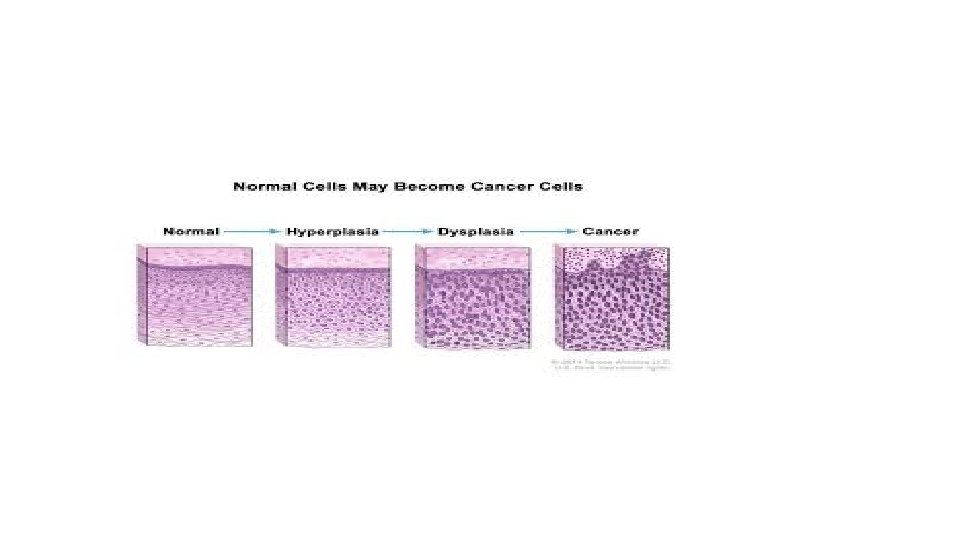
Dysplasia divided to mild, moderate and severe according to extent of involvement and degree of nuclear abnormality
• Although non neoplastic, dysplastic cells can accumulate mutations and transform to malignant lesions. . But not always and not commonly.
Carcinoma in situ • Means= severe dysplasia involving the whole thickness of the epithelium
Carcinoma in situ
• Carcinoma in situ is considered a pre-invasive stage of cancer
Dysplasia, behavior • Non- neoplastic • Dysplastic foci usually seen adjacent to areas of malignant transformation and can predict malignant transformation. • They are precursors of malignancy. • However, mild and moderate dysplasia Can regress if initial insult removed
• The presence of dysplasia preceding cancer is utilized clinically for screening purposes • Cervical cancer in the majority of cases originates from dysplasia… screening for dysplasia by cervical smear (pap smear) helps to detect these precancerous lesions and treatment to prevent cancer can be offered. • Colon cancer can occur in patients with inflammatory bowel disease. . Again dysplasia preceded invasive cancer… surveillance helps detecting these precancerous lesions.
Cancer stem cells • Cancer cells keep growing and proliferating. They are immortal and with limitless proliferative capacity. • So: they must contain cells with stem-like properties.
Stem cells are immortal
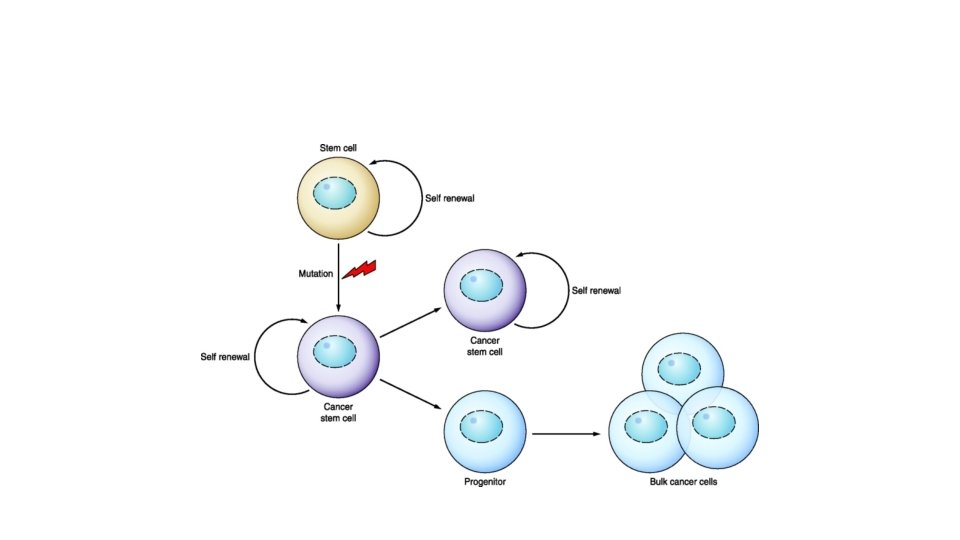
Cancer stem cell hypothesis • It is thought that only a special subset of cells within a tumor has the capacity for self renewal (act as stem cells) • This means that a cancer mass is composed of two types of cells: the “differentiated “ cells that have limited self renewal capacity and stem cells that are immortal and can divide asymmetrically and keep the tumor mass immortal. • SO : TUMOR MASS IS IMMORTAL BUT NOT EVERY TUMOR CELL IS IMMORTAL.
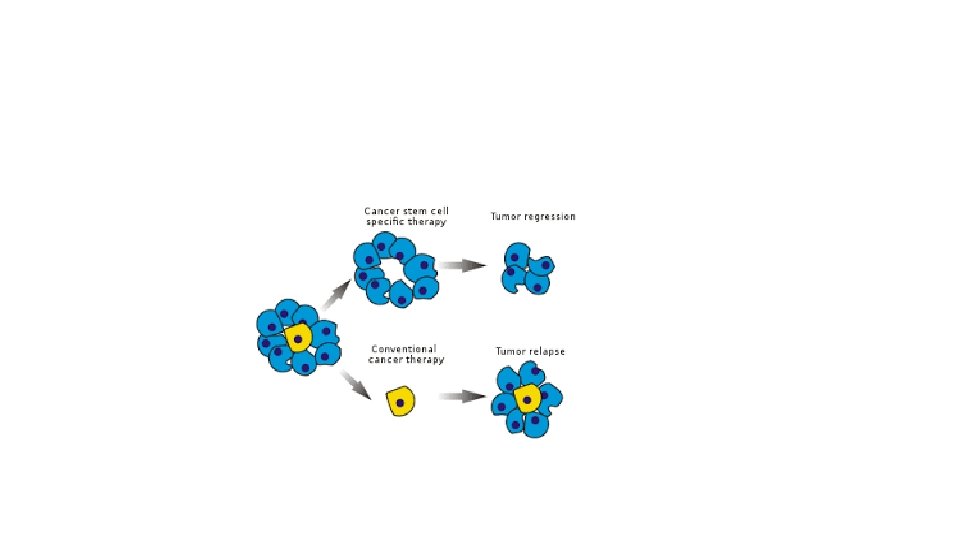
Cancer stem cells • Cancer stem cells are essential for tumor persistence… so elimination of these stem cells is important to cure patients • If cancer stem cells not eliminated… tumor is immortal… no cure
Problem with cancer stem cells • They resist therapy. • Why? 1. Because of their low rate of cell division. Note: the available chemotherapy targets highly dividing cells • 2. because they produce factors that make them resistant to chemo. . Like MDR 1= multiple drug resistance 1
MDR 1 • MDR 1 gene encodes a glycoprotein that makes cells resist drugs by several mechanisms, including efflux of the drug and decreased uptake of the drug by the cells… • So as if MDR 1 is swiping away the drug from the cancer cells. • MDR 1 is expressed in cancer stem cells making them resistant to chemotherapy.
Why we are failing to cure cancer • Probably because of the stem cells… • Chemotherapy kills the proliferating mass of tumor leaving the cancer stem cells that can proliferate and cause recurrence and metastasis
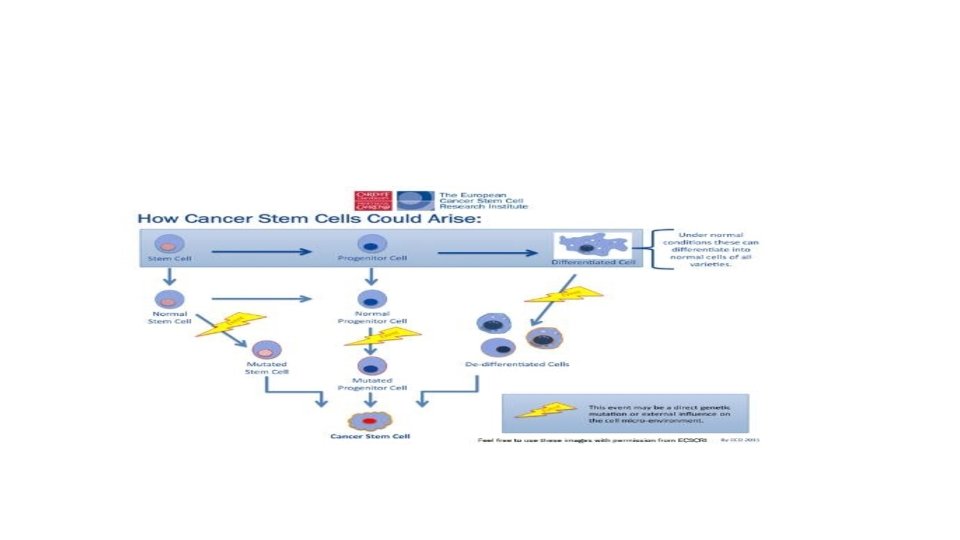
Origin of cancer stem cells • Can arise from normal tissue stem cells or from differentiated cells transforming to stem cells with ability of self renewal. • Note: do not mix normal tissue stem cells with cancer stem cells…they mean different things!!!!
• There is evidence that cancer stem cells can originate from tissue stem cells or from differentiated cells • Example: chronic myelogeous leukemia (CML) originates from hematopoietic stem cells, whereas acute myeloid leukemia are derived from differentiated myeloid precursors
• Cancer epidemiology
USA 2010
Cancer incidence/USA 2013
Notes • In USA. . The leading cause of cancer death in both sexes is lung cancer • In USA the most common cancer in women is breast cancer and in men is prostate cancer
NOTES • In men. . Cancer death rates increased in the last decades. . But now started to decline • In women: overall death rate decreased slightly. . Due to decline in cervical cancer, colon and stomach • Lung cancer in women is increased
Jordan • National cancer registry • According to 2013 stats the most common cancer among Jordanian males is colorectal cancer followed by lung cancer • According to 2013 stats, the most common cancer among Jordanian females is breast followed by colorectal cancer.
Cancer in Jordan
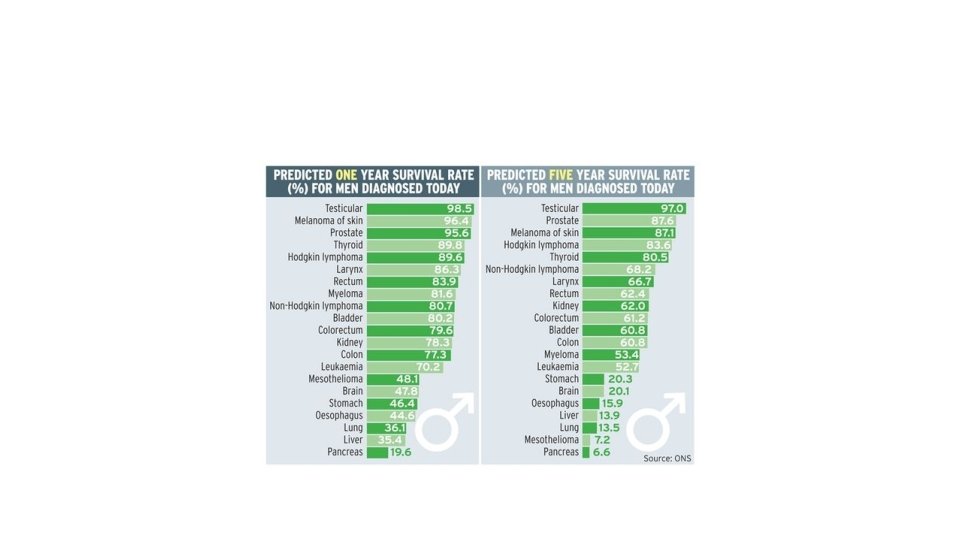
Five year survival • Five-year absolute survival rates describe the percentage of patients alive five years after the disease is diagnosed.
Geographic and environmental factors • Environmental factors are the predominant cause of cancer • Geographic variations in cancer incidence are due to different life styles and to environmental factors • When people move from one geographic area to another, subsequent generations acquire the same risk of cancer development as original population. • Table 5 -2 , page 171 about occupational cancer. . Have a look please.
Cancer and age • In general , frequency of cancer increases with age. • Why: accumulation of mutation takes time! And immunity declines with aging. • However, cancer occurs in children. It is responsible for 10% of all deaths in children younger than 15 years. • Most common childhood tumors: leukemias, lymphomas, CNS tumors and soft tissue and bone sarcomas.
heredity • Some cancers have inherited predisposition. , but still the majority of these need environmental factors to develop cancer • Only 5 -10% of cancers are inherited • This inheritance is usually indirect and its effect is subtle
Autosomal dominant cancer syndromes • Single gene mutations • Typically linked to inheritance of a cancer suppressor gene. • E: g Retinoblastoma. . More will be discussed later
Autosomal recessive syndromes • Usually the problem in DNA repair genes • Example: xeroderma pigmentosum… more later!
Familial cancers of uncertain inheritance • All common cancer types can occur in familial forms with unclear pattern of inheritance • Familial cancers are characterized by: early age, arise in 2 or more close relatives of the index case, can be multiple and bilateral • Familial cancers are not associated with a specific phenotype. Colon cancer can be sporadic, autosomal dominant inheritance ( associated with polyps) or familial with no previous polyps • Predisposition to cancer in these familial cases is probably dominant but incomplete penetrance or multifactorial inheritance cannot be excluded
• Genotype may affect the likelihood of developing environmentally induced cancer • Polymorphism in drug metabolizing enzymes affect lung cancer development among smokers • Genome wide association studies GWAS in lung cancer found variants in a nicotine acid receptor being associated with lung cancer…. These variants were associated with number of cigarettes smoked, so they indirectly increase lung cancer risk by increasing nicotine addiction
Acquired pre-neoplastic syndromes • = preneoplastic or precancerous lesions • These increase the likelihood of cancer but the majority do not progress to cancer • They are important for screening • Also if removed. . Can help decreasing cancer incidence • They contain genetic mutations found in the cancer arises from them
Examples of preneoplastic lesions • Squamous metaplasia and dysplasia of bronchial mucosa in smokers • Endometrial hyperplasia and dysplasia • Leukoplakia • Colonic adenomas
Are benign tumors precancerous • In general no • Some have more risk than other, colonic adenomas have increased risk of malignant transformation and risk depending on degree of dysplasia ( high grade dysplasia carries more risk of malignant transformation than low grade dysplasia)